
Anti-DPPX-Encephalitis in A Patient with Cerebral Vasculitis and Connective Tissue Disease
Abstract
Since the first description in 2013, 39 cases of anti-DPPX-encephalitis have been described. Main features of this autoimmune encephalitis characterized by antibodies against the potassium-channel-associated regulatory protein DPPX are gastrointestinal symptoms, cognitive dysfunction and signs of CNS hyperexcitability. While the majority of patients responds to immunotherapy relapses are frequent and often successfully treated with rituximab.
Here we report another case of anti-DPPX-encephalitis presenting with the above mentioned triad. However, this is the first case of anti-DPPX-encephalitis in the context of a connective tissue disease combined with cerebral arteriopathy along with brain parenchymal lesions that we interpreted as a secondary, CTD-associated cerebral vasculitis. While the latter resolved under immunosuppressive treatment, comprising glucocorticosteroids, cyclophosphamide, rituximab and plasmapheresis, deterioration of the CTD and multiple infectious complications finally led to the patient's death. As histological evidence for cerebral vasculitis is lacking, other differential diagnoses for the observed cerebral arteriopathy, especially reversible cerebral vasoconstriction syndrome, have to be considered.
Author Contributions
Academic Editor: Prabhat Singh, Assistant Professor, MGM Navi Mumbai India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Eva Krause, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
In 2013 Boronat et al. described an autoimmune encephalitis with gastrointestinal symptoms, cognitive dysfunction and signs of CNS hyperexcitability like myoclonus, hyperekplexia, tremor or epileptic seizures characterized by antibodies against "dipeptidyl peptidase-like protein 6" (DPPX) 1. DPPX is a regulatory protein associated with the Kv4.2-potassium-channel on the surface of central and peripheral neurons. DPPX-antibodies reversibly decrease DPPX and Kv4.2 protein on hippocampal neurons thereby causing hyperexcitability of enteric and central nervous system neurons 2, 3. So far, the disease has been described in 39 patients 2. In three patients the disease was associated with systemic lymphoma 2, 4.
Like anti-DPPX-encephalitis, CNS vasculitis is a rare disease presenting with variable neurological symptoms. According to the etiology CNS vasculitis can be classified as a primary angiitis of the CNS (PACNS) or a secondary form associated with systemic disorders like infections, malignant or connective tissue diseases as well as systemic vasculitides 5. Diagnosis of CNS vasculitis is challenging as mimics like reversible cerebral vasoconstriction syndrome (RCVS) have to be considered and as there is no single test permitting definitive diagnosis 6.
Case Presentation
At age 27 this woman of Turkish origin was diagnosed with a connective tissue disease (CTD) comprising features of systemic sclerosis (skin sclerosis, interstitial lung disease, pulmonary fibrosis) and Sjøgren's syndrome (mild sicca syndrome, ANA 1:40.000, anti-SSA/Ro and anti-SSB/La positive, anti-scl-70 negative). To prevent progression of skin sclerosis and pulmonary fibrosis she was treated with prednisone, azathioprine and ciclosporin. At age 32, persistent diarrhea and vomiting caused weight loss of 20kg (BMI 13,6kg/m²). Gastroenterological work-up was inconspicuous. However, personality changes (especially increased anxiety), memory disturbances, concentration deficits, disorientation, impoverished and slowed speech gradually developed over a few months accompanied by exaggerated startle, tremor, insecure gait, burning pain of the lower legs, dysphagia and incontinence. Initially, atypical anorexia nervosa was suspected and she was admitted to a psychotherapeutic unit. Three days after a first generalized epileptic seizure she was transferred to our department. On admission she was disoriented to time, displayed a slight dysarthria, dysphagia, saccadic smooth pursuit eye movements, intention tremor, ataxia, myoclonus of all limbs and exaggerated acoustic and tactile startle. Reflexes were brisk, atavistic reflexes were positive.
Cerebral MRI revealed multiple supra- and infratentorial FLAIR-hyperintense lesions involving both cortex and white matter. A cerebellar lesion was partially hyperintense on DWI, though without concomitant hypointensity on ADC, and showed weak contrast enhancement (Figure 1A). MR- and digital subtraction angiography displayed segmental narrowing and dilation of proximal as well as distal vessels in all territories (Figure 1C). Analysis of CSF showed normal cell count (3 cells/µl) while cytological examination revealed presence of activated lymphocytes. Glucose and lactic acid levels were normal, protein level was elevated (168mg/dl) and there was intrathecal IgM- and IgG-synthesis. Infectious causes were ruled out (including panbacterial and panfungal PCR, QuantiFERON-TB Gold in Tube Test©, CMV, EBV, enterovirus, HIV, FSME, VZV, hepatitis B/C, cryptococcus neoformans, candida and aspergillus species, borrelia burgdorferi, treponema pallidum). We diagnosed cerebral vasculitis and due to the patient's rapid decline directly administered a methylprednisolone pulse followed by an oral tapering with prednisolone without performing a biopsy. Four days after the start of steroid-therapy basal ganglia hemorrhage caused left-sided hemiplegia and anarthria. By that time, MRI showed progression of the aforementioned FLAIR-hyperintense lesions (Figure 1C) without any contrast enhancement along with new cerebellar microbleeds and bilateral narrow subdural hygroma (after lumbar puncture). On MRA intracranial artery changes had resolved. We intensified immunosuppression by administration of cyclophosphamide.
Figure 1.Imaging findings. (A) MRI-images on admission showing multiple supra- and infratentorial FLAIR-hyperintense lesions involving both cortex and white matter and one cerebellar lesion with weak contrast enhancement and partial DWI-hyperintensity. (B) Digital subtraction angiography showing segmental narrowing and dilation of proximal as well as distal vessels in all territories. (C) MRI-images 4 days after start of steroid-therapy showing progression of the FLAIR-hyperintense lesion. (D) MRI images after administration of methylprednisolone and cyclophosphamide showing nearly full regression of parenchymal lesions. (E) MRI shortly before the patient's death showing blood degradation products in the right frontal subarachnoid space and right basal ganglia.
Owing to the uncommon clinical presentation of cerebral vasculitis we screened for antineuronal-autoantibodies. Anti-DPPX-antibodies were detected in CSF and serum (both 1:100, cell-based indirect immunofluorescence assay) establishing the additional diagnosis of anti-DPPX-encephalitis. Whole body FDG-PET/CT did not suggest underlying malignancy. After cyclophosphamide and plasmapheresis the FLAIR-hyperintense lesions on MRI disappeared almost completely and MRA still showed normalization of intracranial arteries (Figure 1D). Anti-DPPX-titer dropped to 1:32. Hyperekplexia and myoclonus decreased under symptomatic treatment with clonazepame. Therapy with rituximab was started. After two months she was transferred to a rehabilitation unit from where she returned three weeks later somnolent, tetraplegic and anarthric. EEG revealed non-convulsive status epilepticus that was successfully terminated by valproate, also leading to some clinical improvement. However, as anti-DPPX-titer had risen to 1:1000 we initiated a second plasmapheresis-cycle. Thereafter anti-DPPX-titer dropped to 1:100. Another cycle of rituximab and treatment with azathioprine were started. Five weeks later she was again transferred to the rehabilitation unit, where she improved markedly, being able to use a wheelchair independently, walk over short distances in a gait training device, use her right arm and ingest food orally.
Four months after initiation, azathioprine was stopped due to leuko- and thrombocytopenia. One month later, myoclonus increased, her cognition deteriorated, and she developed infectious complications requiring readmission to our hospital. Cerebral MRI including MRA showed timely resorption of basal ganglia hemorrhage without any further pathologies. Anti-DPPX-titer had risen to 1:320. Since FACS-analysis showed complete peripheral depletion of B-lymphocytes we only conducted a third plasmapheresis-cycle.
Thereafter she developed pneumonia with sepsis and respiratory failure requiring mechanical ventilation. Thoracic CT and echocardiography suggested exacerbation of slightly preexisting, CTD-associated pulmonary fibrosis and pulmonary hypertension causing congestive heart failure. Tracheotomy became necessary. After successful weaning from mechanical ventilation right heart catheterization confirmed severe pulmonary hypertension (PA pressure ~80 mmHg) along with right heart failure. A therapy with Macitentan and Tadalafil was started. Blocked tracheostomy was kept in place to prevent aspiration due to dysphagia and CTD-associated disturbance of gastrointestinal motility. Nutrition was maintained via the PEG feeding tube. Communication was realized non-verbally and via a communication board. In addition to the left-sided hemiparesis limb contractures limited the patient's mobility. Altogether the patient was functionally completely dependent and predominantly bedridden.
During early neurological rehabilitation pulseless ventricular tachycardia required cardiopulmonary resuscitation. Multiple infectious complications, especially concerning the lungs and urinary tract, deteriorated the patient's condition even more so when she returned back home she required 24-hour intensive care by a nurse.
21 months after initial contact, the patient was admitted to our hospital's internal medicine unit because of an acute renal failure with urosepsis requiring hemodialysis. In addition cardiac cirrhosis with ascites was diagnosed. In the neurological examination the patient was somnolent, showed a spastic, left-sided hemiparesis and a newly increase of myclonus. Cerebral MRI displayed blood degradation products in the right frontal subarachnoid space, a new microbleed in the left temporal white matter as well as whole brain atrophy (Figure 1E). Anti-DPPX-titer had risen to 1:32000. In the further course, the patient developed aspiration pneumonia eventually causing septic shock with multiple organ failure that lead to her death at the age of 34. An autopsy was not performed (Figure 2).
Figure 2.Overview of disease course. 21 months follow-up of antibody (ab) titers in serum in parallel with immunosuppressive/immunomodulatory interventions and specific clinical events as indicated. The clinical course is represented by different colors from dark red (unfavorable) to dark green (good).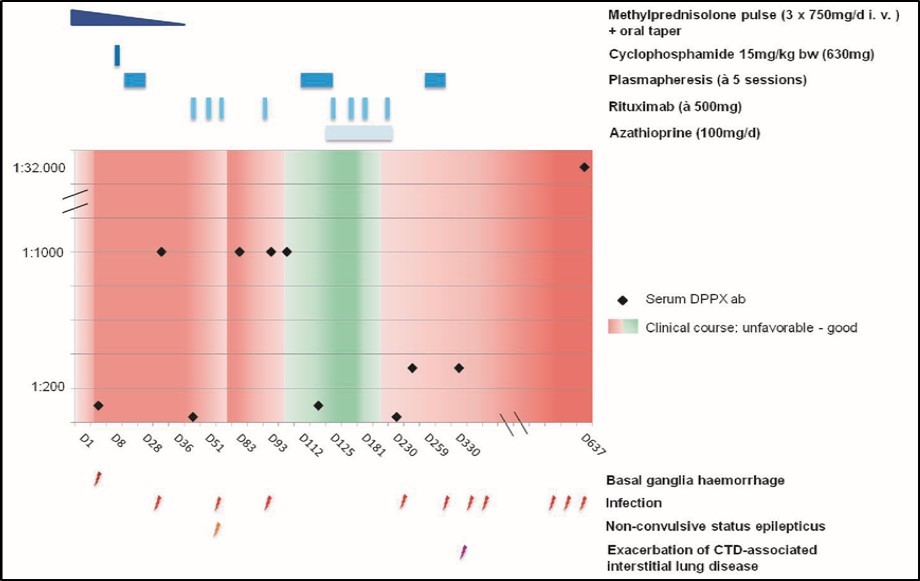
Discussion
This patient presented with the triad characteristic for anti-DPPX-encephalitis comprising gastrointestinal symptoms, cognitive dysfunction and signs of CNS hyperexcitability 2. Like in 17% of cases reported so far, the disease ended fatally, which can be attributed primarily to infectious complications due to immunosuppression and exacerbation of the associated CTD.
What should be highlighted with respect to anti-DPPX-encephalitis is, that this case supports the notion that anti-DPPX-antibodies cause cardiac arrhythmias 4 as there were three reported episodes of ventricular tachycardia in this patient, one of them requiring cardiopulmonary resuscitation.
What is new about this case compared to all previous ones, is the association with cerebral arteriopathy presenting with reversible segmental narrowing and dilation of proximal and distal vessels in all territories along with MRI-findings suggestive of reversible cerebral vasogenic edema, cerebellar ischemia and subarachnoid bleeding as well as basal ganglia hemorrhage and few microbleeds.
Because of the inflammatory changes in CSF we explained these findings by cerebral vasculitis that we interpreted as a secondary, CTD-associated form, even though very uncommon in systemic sclerosis 7.
While retrospectively the inflammatory changes in CSF can be explained by anti-DPPX-encephalitis, there is no evidence that the cerebral arteriopathy together with the MRI changes is caused by anti-DPPX-antibodies. Besides, considering the fact, that the observed arteriopathy resolved within less than three weeks, especially one differential diagnosis has to be taken into account: a reversible cerebral vasoconstriction syndrome, even though the patient never suffered from thunderclap headache or any other kind of headaches. This notion is supported by the acute onset with a generalized epileptic seizure and the marked changes of intracranial arteries found on digital subtraction angiography as well as by the occurrence of a deep parenchymal hemorrhage and probable subarachnoid bleeding, all features that have been described as characteristic of RCVS and not so much of cerebral vasculitis 6.
Other differential diagnoses in the context of immunosuppression potentially being able to cause the observed cerebral arteriopathy, namely intravascular lymphoma and lymphomatoid granulomatosis were judged to be unlikely as FDG-PET was inconspicious and cerebral arteriopathy resolved rapidly.
In summary, we cannot clearly define what exactly caused the cerebral arteriopathy in our patient as histological evidence is lacking. Therefore we would like to sensitize other neurologists for the potential link between anti-DPPX-encephalitis and cerebral vasculitis / reversible cerebral vasosconstriction syndrome especially in patients with an autoimmune disposition aiming to close this gap.
Conflicts of interest:
Eva Krause declares that there is no conflict of interest regarding the publication of this article.
Timolaos Rizos was payed for lectures and received travel / accommodation / meeting expenses from Bayer Health Care, Böhringer Ingelheim, Daichii Sankyo, BMS Pfizer.
Mike Soehendra declares that there is no conflict of interest regarding the publication of this article.
Norbert Blank declares that there is no conflict of interest regarding the publication of this article.
Hans-Michael Meinck declares that there is no conflict of interest regarding the publication of this article.
Silvia Schönenberger declares that there is no conflict of interest regarding the publication of this article.
Simon Nagel is a consultant for Brainomix, was payed for lectures (including service on speaker bureaus) by Bayer, Pfizer and Medtronic and received travel/accommodations/meeting expenses unrelated to the aforementioned from Brainomix and Böhringer Ingelheim.
References
- 1.Boronat A, Gelfand J M, Gresa-Arribas N. (2013) Encephalitis and antibodies to dipeptidyl-peptidase-like protein-6, a subunit of Kv4.2 potassium channels. , Annals of neurology 73, 120-128.
- 2.Hara M, Arino H, Petit-Pedrol M. (2017) DPPX antibody-associated encephalitis: Main syndrome and antibody effects. , Neurology 88, 1340-1348.
- 3.Piepgras J, Holtje M, Michel K. (2015) Anti-DPPX encephalitis: pathogenic effects of antibodies on gut and brain neurons. , Neurology 85, 890-897.
- 4.Tobin W O, Lennon V A, Komorowski L. (2014) DPPX potassium channel antibody: frequency, clinical accompaniments, and outcomes in 20 patients. , Neurology 83, 1797-1803.
- 5.Dutra L A, de Souza AW, Grinberg-Dias G, Barsottini O G, Appenzeller S. (2017) Central nervous system vasculitis in adults: An update. , Autoimmunity reviews 16, 123-131.