Abstract
Leishmaniasis treatment monitoring is an important problem, since patient’s frequently present clinical signs improvements with positive indirect immunofluorescence (IFI) titers of anti-Leishmania antibodies, thus making difficult the clinician understand the therapy efficacy. The study aimed 1) to identify over a short period of 30 days, which of the main changes on the serum proteinogram fractions in patients treated with meglumine antimoniate and allopurinol, can be pointed as indicator to classify patients as slower or faster responsive to treatment. A sample of 56 dogs (n=56) with leishmaniasis diagnosis was followed-up for clinical condition, proteinograms and titers of anti-Leishmania antibodies during the treatment period considering three different time points: M0 (diagnosis moment), M1 (15 days after therapy start), and M2 (30 days after therapy start). Two groups of patients were considered according to their clinical condition evolution rate: faster recovery group (FRG) and slower recovery group (SRG). Statistical significant results were considered for p-value <0.05. Statistically significant differences in proteinogram variations between FRG and SRG were registered for TPs (p= 0.03), and for the fractions β (p=0.04), γ (p=0.04), amongst M0 and M2.The PT, β and γ-globulin fractions of proteinogram, in association with patient clinical assessment evolution should be considered as an indicator and a simple way to appoint the efficacy response of the patients to the therapy.
Author Contributions
Academic Editor: Mohamed Zowalaty, School of Health Sciences University of KwaZulu-NatalWestville Campus, Durban
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Miguel Carreira, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Leishmaniasis treatment monitoring is an important problem, since patient’s frequently present clinical signs improvements with positive indirect immunofluorescence (IFI) titers of anti-Leishmania antibodies, thus making difficult the clinician understand the therapy efficacy. Proteinogram has potential for monitoring the patient response to leishmaniasis therapy (Noli 1999, Martínez-Subiela & Cerón 2005, Cerón, Caldin, Martinez-Subiela 2011, Paim et al. 2013). Electrophoresis is designed to separate serum protein into different fractions, and it is the result of serum exposing to an electrical current allowing obtain the different serum proteins which migrate in bands, separating and quantifying the different fractions in a sample, according to their physical properties, such as size, charge and molecular weight (Eckersal 2008), the proteinogram in domestic animals considers the following fractions: albumin, alpha (α) globulin (α1, α2), beta (β) globulin (β1, β2), and gamma (γ) globulin (Thomas 2000, Meyer, Harvey 2004, Eckersal 2008). Increased serum total proteins (TPs) - hyperproteinemia, and a decreased albumin/globulin (A/G) ratio associated with hyperglobulinemia and hypoalbuminaemia, are the most frequent registered variation in Leishmania-infected dogs’ serum proteinograms showing the disease, since dogs may be infected but clinically healthy (Cerón, Caldin, Martinez-Subiela 2011, Greene 2011). According to Silva et al. (2008), 63.2% of leishmaniasis patients exhibit hypoalbuminemia, which is related to the chronic nature of the disease, renal (glomerulonephritis) and liver failures, and decreased food intake (Cerón, Eckersall, Martínez-Subiela 2005, Solano-Gallego et al. 2011). Increases in α-globulin and β-globulin fractions associated with an acute phase response to the disease are present in 36.0% of the patients (Thomas 2000, Sasanelli et al. 2007, Silva, Lima, Soto-Blanco 2011, Martinez-Subiela S, Strauss-Ayali D, Cerón JJ, Baneth 2011). Acute phase proteins (APP) although not specific, can be considered good biological markers of diseases for which quantification provides early clinical information useful for therapeutic monitoring and prognosis (Noli & Auxilia 2005, Martinez-Subiela, Strauss-Ayali, Cerón, Baneth 2011, Solano-Gallego et al. 2009, Paradies et al. 2012). Restoration of serum proteinogram values is a useful indicator of therapeutic efficacy; however, for it to occur in all the parameters it may require examination up to 6 months after treatment (Noli 1999, Cerón, Caldin, Sasanelli et al 2007, Solano-Gallego et al. 2009, Martinez-Subiela 2011). The clinical efficacy of the treatment should always be evaluated as the result of changes in physical examination and in laboratory medicine, otherwise no conclusion about the issue may be set. The present study was performed in dogs with leishmaniasis diagnosis and clinical recovery, and aimed 1) to identify over a short period of 30 days, which of the main changes on the serum proteinogram fractions in patients treated with meglumine antimoniate and allopurinol, can be pointed as indicator to classify patients as slower or faster responsive to treatment.
Materials and Methods
The study included a sample composed of 56 dogs (n=56) of both genders (35.7% females and 64.3% males) and all breeds, evaluated with a diagnosis of leishmaniasis and submitted to meglumine antimoniate therapy (50 mg/Kg every 12 hours) for 20 days divided into two blocks of 10 days each, separated by a 10 days interval, followed by the use of allopurinol (20 mg/kg/day). Canine leishmaniasis was diagnosed on the basis of history, clinical signs, and clinico-pathological abnormalities compatible with the disease, and a positive sample ratio values (Rz). These animals were regular hospital patients evaluated with a clinical condition (leishmaniasis), from which a blood sample was withdrawn from a peripheral vein for routine analysis and proteinograms. The use of the patient’s laboratory data started only after owners’ written consent forms signed. At no time were these animals used as experimental animals. Serum samples were obtained after collected whole blood with a covered red topped tube type Vacutainer® submitted to a centrifuging at 1,000-2,000 x g for 10 minutes. After, we removed the clot to obtain the serum which was immediately transferred into a clean tube using a Pasteur pipette, stored at 2°C and shipped to the laboratory refrigerated in on a cool pack.18 All the tubes were labeled with the patient identification. Detection and quantification of Leishmania antibodies in the canine serum was made using enzyme-linked immunosorbent assay (ELISA-enzyme-linked immunosorbent assay) Leiscan®, manufactured by Laboratories Hipra and marketed by Esteve Farma. The kit offers the possibility of controlling the test at three different points (negative control, low positive and positive) against the two points traditionally used. It should also be noted that the serology results became issued as sample ratio values (Rz) according to a formula which relates sample absorbance to the absorbance of the low-positive control. The Rz has similarity to IFI, in accordance with represented in Table 1. Leiscan® presents a 100% of specificity, 100% of positive predictive value, 98% of sensitivity value and 98% of accuracy19. For the proteinogram a SAS-1 seric protein kit® from Helena Biosciences Europe laboratory was used. This method makes the separation and quantification of serum proteins by electrophoresis on agarose gel. Serum proteins are separated into 5 main classes: albumin, (α) globulin (α1, α2), beta (β) globulin (β1, β2), and gamma (γ) globulin. Performance characteristics of the method for reproducibility are listed in Table 1. Sensitivity value of the method is 0.3 g/l per band, which is determined as the lowest concentration of protein that can be observe a discrete band on the gel (HIPPRA 2015).The study was carried out for 30 days and considered 3 different time points: M0 (diagnosis), M1 (15 days after therapy start), and M2 (30 days after therapy start), during which patient’s clinical signs assessment was made and blood samples were collected for routine analysis and proteinograms. According to the clinical condition evolution, patients were divided into two groups: those who showed a faster recovery (FRG) and those who presented a slower recovery (SRG). In M0 and M2, IFI titers of anti-Leishmania antibodies were also developed. The inclusion criteria of patients in study were: presence of a leishmaniasis-positive titer, being on stage II (moderate disease) or stage III (severe disease) according to Solano-Gallego et al. (2009) clinical staging of the disease, submitted to meglumine antimoniate and allopurinol therapy, and with one proteinogram for each moment. For statistical analysis we used SPSS Statistics software version 17.0 ®. The Shapiro-Wilk test showed normality of the sample data. ANOVA One-Way test was used to analysis the patients proteinogram significant variations between SRG and FRG, followed by the post-hoc Bonferroni test over the three study considered momentsM0, M1, and M2 for pairwise comparisons. Results were statistically significant for p values <0.05. 95% value was used on the evaluations of the confidence intervals.
Table 1. Performance characteristics of reproducibility of the methods used by the laboratory for the proteinogram and leishmaniasis test.| Leishmaniasis | ||||||
| Concordance ratio between Leiscan / IFI Titulation tests | ||||||
| Ratio | Result | Equivalent IFI titulation | ||||
| Rz < 0,5 | Negative | Negative | ||||
| 0,5 < Rz < 0,7 | Negative | 1/20 to 1/42 | ||||
| 0,7 < Rz < 0,9 | Negative | 1/40 to 1/82 | ||||
| 0,9 < Rz < 1,1 | Dubious | 1/82 | ||||
| 1,1 < Rz < 1,5 | Weak positive | 1/80 to 1/162 | ||||
| 1,5 < Rz < 2 | Strong positive | 1/160 to 1/322 | ||||
| 2 < Rz < 3 | Strong positive | 1/320 to 1/640 | ||||
| 3 < Rz < 4 | Very strong positive | 1/640 to 1/1280 | ||||
| Rz > 4 | Very strong positive | > 1/1282 | ||||
| Proteinogram | ||||||
| Reproducibility | Intra-test (n=16) | Intra-test (n=95) | ||||
| Mean (%) | Coefficient ofvariation (%) | Mean (%) | Coefficient ofvariation (%) | |||
| albumine | 60.1 | 1.7 | 60.4 | 2.3 | ||
| α1- globulin | 4.2 | 7.5 | 4.3 | 7.3 | ||
| α 2- globulin | 11.4 | 4.1 | 10.3 | 7.8 | ||
| β- globulin | 10.5 | 2.1 | 11.2 | 6.8 | ||
| γ- globulin | 13.8 | 3.0 | 13.8 | 5.5 | ||
| Parameter | N total | Type | N partial | % |  ± SD ± SD |
min | max | ||||||
| Age (years) | 56 | - | - | - | 7.1 ± 3.3 | 2 | 11 | ||||||
| Gender | 56 | Male | 35 | 62.50 | - | - | - | ||||||
| Female | 21 | 37.50 | - | - | - | ||||||||
| Breed | 56 | Crossbreed | 24 | 42.86 | - | - | - | ||||||
| Boxer | 11 | 19.64 | - | - | - | ||||||||
| Labrador retiver | 8 | 14.29 | - | - | - | ||||||||
| Pitt-bull | 7 | 12.50 | - | - | - | ||||||||
| German shepard | 5 | 8.93 | - | - | - | ||||||||
| Spitz | 1 | 1.79 | - | - | - | ||||||||
| Clinical signs | 56 | Weight Loss | 28 | 50.00 | - | - | - | ||||||
| Gastroenteric | 24 | 42.86 | - | - | - | ||||||||
| Polydipsia/Polyuria | 22 | 39.29 | - | - | - | ||||||||
| Lethargy | 20 | 35.71 | - | - | - | ||||||||
| Prostration | 20 | 35.71 | - | - | - | ||||||||
| Ocular changes | 16 | 28.57 | - | - | - | ||||||||
| Onychogryphosis | 12 | 21.43 | - | - | - | ||||||||
| Muscle atrophy | 9 | 16.07 | - | - | - | ||||||||
| IFI titres of anti-leishmania antibodies | 56 | M0 | 1/80 | 4 | 7.14 | - | - | - | |||||
| 1/160 | 32 | 57.14 | - | - | - | ||||||||
| 1/240 | 12 | 21.43 | - | - | - | ||||||||
| 1/320 | 8 | 14.29 | - | - | - | ||||||||
| 56 | M2 | 1/80 | 4 | 7.14 | - | - | - | ||||||
| 1/160 | 36 | 64.29 | - | - | - | ||||||||
| 1/240 | 8 | 14.29 | - | - | - | ||||||||
| 1/320 | 8 | 14.29 | - | - | - | ||||||||
| Proteinogram fractions | Moment | Normal range | |||||||||||
| Total proteins(g/dL) | M0 | 5.5-7.5 | 8.62 ±1.35 | 5.50 | 10.51 | ||||||||
| M1 | 8.10 ±1.04 | 6.40 | 9.70 | ||||||||||
| M2 | 7.40 ±1.24 | 6.00 | 10.50 | ||||||||||
| A/G ratio | M0 | 0.6-1.1 | 0.50 ±0.21 | 0.20 | 1.00 | ||||||||
| M1 | 0.51 ±0.23 | 0.30 | 1.10 | ||||||||||
| M2 | 0.67 ±0.22 | 0.40 | 1.20 | ||||||||||
| Albumin(g/dL) | M0 | 2.26 –4.31 | 2.74 ±0.85 | 1.42 | 4.00 | ||||||||
| M1 | 2.66 ±0.87 | 1.75 | 4.30 | ||||||||||
| M2 | 2.79 ± 0.5 | 2.20 | 3.80 | ||||||||||
| α1-globulin (g/dL) | M0 | 0.32-0.75 | 0.54 ±0.36 | 0.10 | 1.00 | ||||||||
| M1 | 0.52 ±0.29 | 0.10 | 0.98 | ||||||||||
| M2 | 0.51 ±0.23 | 0.20 | 0.87 | ||||||||||
| α2-globulin(g/dL) | M0 | 0.5-1.17 | 1.38 ±0.49 | 0.80 | 2.30 | ||||||||
| M1 | 1.24 ±0.46 | 0.30 | 2.02 | ||||||||||
| M2 | 1.04 ± 0.3 | 0.50 | 1.70 | ||||||||||
| β-globulin(g/dL) | M0 | 0.93-2 | 2.14 ±0.63 | 1.00 | 3.30 | ||||||||
| M1 | 2.19 ±0.39 | 1.40 | 2.60 | ||||||||||
| M2 | 1.94 ±0.67 | 1.30 | 3.99 | ||||||||||
| γ-globulin(g/dL) | M0 | 0.39-1.02 | 1.82 ±0.76 | 1.10 | 4.00 | ||||||||
| M1 | 1.42 ±0.52 | 0.87 | 2.80 | ||||||||||
| M2 | 1.05 ±0.55 | 0.40 | 2.69 | ||||||||||
Figure 1. Analysis of proteinogram parameters mean values variations over the three considered moments (M0,M1,M2)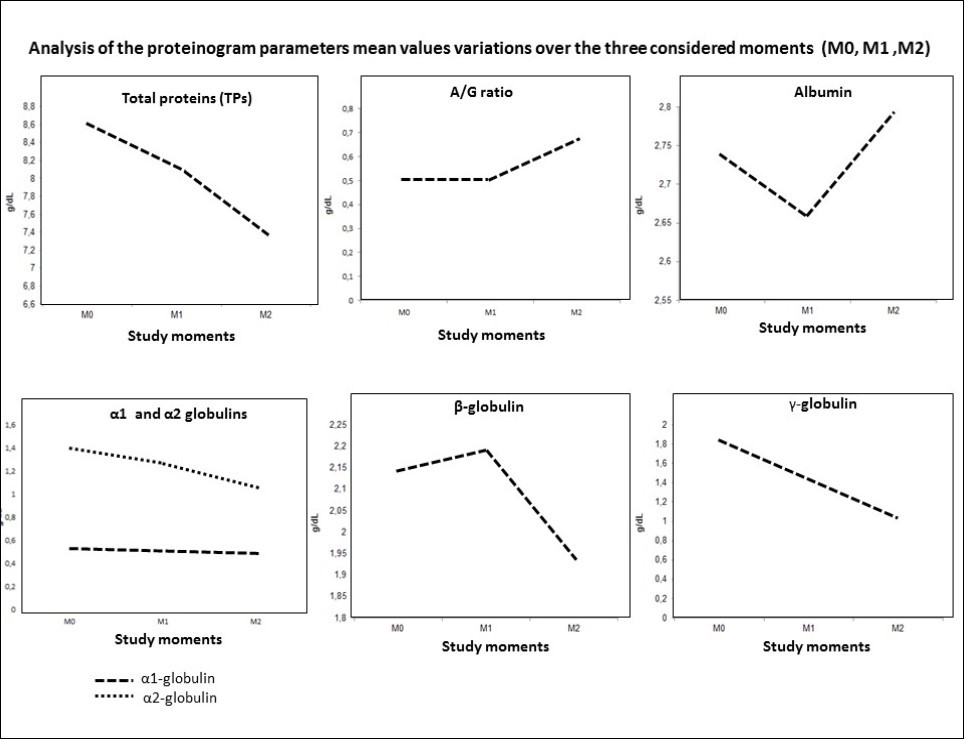
Results
Sample characterization for age, gender, breeds, clinical signs, and IFI titers of anti-Leishmania antibodies are shown in Table 2. Soon after the end of antimonial therapy (M2) antibody titer was not changed in most of the patients (78.6%), and four patients (7.1%) presented increased titers from M0 to M2. Weight loss, gastroenteric and polydipsia / polyuria associated with renal failure were de most registered clinical signs with 50.0%, 42.8%, and 39.2% respectively, and muscle atrophy the lesser with a value of 16.0% amongst all patients. For FRG patients the mean of the recovery of their clinical condition was around 3 weeks, in contrast to the SRG mean of 5 weeks. Variations in proteinogram fractions over time points M1, M2, and M3 are shown in Table 2. At M0 hyperproteinemia was presented in 78.5% of the patients and the A/G ratio was decreased in 71.4%. Hypoalbuminemia was registered in 35.7% of the patients, α1-hyperglobulinemia in 35.7%, α2-hyperglobulinemia in 64.2%, β-hyperglobulinemia in 57.1%, and γ-hyperglobulinemia in all individuals (100%). At M1 the hyperproteinemia maintained it value with 78.5%. but 64.2% of the patients had a A/G ratio less than 0.5. Hypoalbuminemia was presented in 42.8% of the patients, α1-hyperglobulinemia in 42.8%, α2-hyperglobulinemia in 57.1%, β-hyperglobulinemia in 64.2%, and γ-hyperglobulinemia in 71.4%. At M2. 35.7% of the patients showed hyperproteinemia and 35.7% a A/G ratio with values less than 0.5 mg/L. Hypoalbuminemia was noted in 14.2% of the patients. α1-hyperglobulinemia in 21.4%, α2-hyperglobulinemia in 35.7%, β-hyperglobulinemia in 28.5%, and γ-hyperglobulinemia in 50% of the patients. Statistically significant differences in proteinogram variations between the SRG and FRG are presented in Table 3, and were recorded for TPs (p= 0.03), and for the fractions β (p=0.04), γ (p=0.04). According to the Bonferroni test p-value, differences for the parameters were registered only between M0 and M2 for PT TPs (p= 0.03), and for the fractions β (p=0.04), γ (p=0.03) (Table 3).
Table 3. ANOVA One-Way and Post-Hoc Bonferroni tests to analysis the patients proteinogram variations over the three study considered moments M0 (diagnosis); M1 (15 days after therapy start) and M2 (30 days after therapy start)| Parameter | Group of patients | ANOVA One-Way | Moment | Bonferroni-test | |
| sum of squares SS | p-value | p-value | |||
| Total proteins(g/dL) | SRP | 0.83 | 0.88 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 33.00 | 0.03 | M0/M1 | 0.53 | |
| M0/M2 | 0.03 | ||||
| M1/M2 | 0.41 | ||||
| A/G ratio | SRP | 0.06 | 0.74 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 0.15 | 0.54 | M0/M1 | - | |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| Albumin(g/dL) | SRP | 0.07 | 0.95 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 0.55 | 0.77 | M0/M1 | - | |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| α1-globulin(g/dL) | SRP | 0.00 | 0.98 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 0.12 | 0.64 | M0/M1 | - | |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| α2-globulin(g/dL) | SRP | 0.99 | 0.28 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 1.23 | 0.29 | M0/M1 | - | |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| β-globulin(g/dL) | SRP | 0.03 | 0.97 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 2.55 | 0.04 | M0/M1 | 0.37 | |
| M0/M2 | 0.04 | ||||
| M1/M2 | 0.83 | ||||
| γ-globulin(g/dL) | SRP | 1.88 | 0.41 | M0/M1 | - |
| M0/M2 | - | ||||
| M1/M2 | - | ||||
| FRP | 4.97 | 0.04 | M0/M1 | 0.29 | |
| M0/M2 | 0.03 | ||||
| M1/M2 | 1.02 | ||||
| Parameter | Moment | Friedman | Wilcoxon |
| P-value | P-value | ||
| Total proteins(g/dL) | M0/M1 | 0.00 | 0.07 |
| M0/M2 | 0.00 | 0.12 | |
| M1/M2 | 0.00 | 0.01 | |
| A/G ratio | M0/M1 | 0.06 | - |
| M0/M2 | 0.08 | - | |
| M1/M2 | 0.00 | 0.01 | |
| Albumin(g/dL) | M0/M1 | 0.41 | - |
| M0/M2 | 0.70 | - | |
| M1/M2 | 0.39 | - | |
| α1-globulin(g/dL) | M0/M1 | 0.78 | - |
| M0/M2 | 0.72 | - | |
| M1/M2 | 0.53 | - | |
| α2-globulin(g/dL) | M0/M1 | 0.00 | 0.07 |
| M0/M2 | 0.00 | 0.01 | |
| M1/M2 | 0.00 | 0.08 | |
| β-globulin(g/dL) | M0/M1 | 0.01 | 0.25 |
| M0/M2 | 0.34 | - | |
| M1/M2 | 0.01 | 0.01 | |
| γ-globulin(g/dL) | M0/M1 | 0.00 | 0.00 |
| M0/M2 | 0.00 | 0.00 | |
| M1/M2 | 0.00 | 0.00 |
Discussion
Staging the leishmaniasis can be achieve based on patient clinical signs, serological condition, and clinicopathological abnormalities as proposed by the LeishVet group (Solano-Gallego et al. 2009).In the present study after the meglumine antominoate therapy and still under therapy with allopurinol, it was possible to notice that although patients presented a clinical probably associated with the chronic nature of the disease (since albumin is a negative APP), with liver disease (resulting in a reduction of albumin synthesis), and with renal failure (due to selective loss of the albumin associated with the meglumine antimoniate treatment) (Martínez-Subiela & Cerón 2005, Cerón, Eckersal, Martínez-Subiela 2005). At M1 the number of patients with hypoalbuminemia increased 7.1% (from 35.7% to 42.8%), and at M2 decreased 28.6% (from 42.8% to 14.2%), thus showing a good response to treatment. Contrary to the study of Sasanelli et al.(2007), in the present study the albumin serum concentration did not increased progressively but only at the second treatment block, i.e., at day 20 after start the therapy. Variations in the α1- and α2-globulin fraction levels (where the majority of the APP are) were common, with values of 35.7% (more than one third) and 64.2% (almost two thirds) respectively. These results confirm the previously-described acute phase response in dogs infected with Leishmania infantum (Sasanelli et al. 2007, Martinez-Subiela et al. 2011).The fact that the increase of the α1-globulin fraction level was smaller than the α2-globulin fraction may be due to α1-antitrypsin, which plays a leading role in the acute inflammatory process and is therefore no longer high in most patients with Leishmania infection. Moreover, this fraction is also comprised by α1-acid glycoprotein, which also has an anti-inflammatory character (Eckersal et al. 2008, Meyer, Harvey 2004, Silva, Lopes, Faria 2008). The α1-globulin fraction did not showed statistically significant differences between M0 and M2. The higher number of patients showing increases in the α2-globulin fraction may be related to the presence of ceruloplasmin, a vital protein for the regeneration process, which is always associated with chronic inflammatory processes (Martínez-Subiela & Cerón 2005, Cerón, Eckersal, Martínez-Subiela 2005). In addition, ceruloplasmin may have increased the haptoglobin level which is a protein responsible for iron binding, thus decreasing its availability to pathogens. Both proteins were described as high in patients with leishmaniasis (Martínez-Subiela & Cerón 2005, Cerón, Eckersal, Martínez-Subiela 2005, Sasanelli et al. 2007, Silvestrini et al. 2014). Statistically significant progressive decrease in α2-globulin serum mean concentration was observed between over the point moments, with the percentage variation of dogs with α2-hyperglobulinemia from 64.2% at M0, to 57.1% at M1 and to 35.7% at M2. This situation is related to a decrease of some APP during the treatment, in particular haptoglobin (Sasanelli et al. 2007, Martinez-Subiela &, Strauss-Ayali, Cerón, Baneth 2011).The β-globulin fraction levels also fluctuated throughout the study, presenting a statistically significant decrease only from M1 to M2. The serum β -globulin was increased at M1 in more than 50% of the patients in a 7.1% mean (from 57.1% to 64.2%), being associated with the rise in complement factor C3 essential for membrane attack complex development following the classical, alternative, or lectin paths for complement activation by the C-Reactive protein, which is also part of the β-globulin fraction (Noli 1999, Meyer & Harvey 2004). At M2 the β-globulin levels decreased 35.7% (from 64.2% to 28.5%) being related to reduction of C-Reactive protein and C3 levels, with the most patients achieving normal serum concentrations. At an early stage of infection there is a progressive increase in β-globulin followed by a rise in γ-globulins as exhibited by all patients involved in the study (Noli 1999).This can be attributed to immunoglobulin increase since these can migrate either in the β or γ fractions developing a phenomenon named as the "β-γ Bridge", in which it is not possible to observe a clear separation between these two fractions (Kaneko 1997). The γ-globulin serum concentration throughout the study showed statistically significant decreases at the three point moments, associated with a decrease in humoral immune response. Reduction of the levels were from M0 to M1 of 28.6% (from 100% to 71.4%) and from M1 to M2 of 21.4% (from 71.4% to 50%). However. 50% of the patients still experienced at the end of M2 values above the reference limits which can be obtained only six months after the treatment (Sasanelliet al. 2007) so the observed decreases demonstrate a good response to treatment and can interpreted as a significant reduction of the parasite in the patients resulting in an improvement of health (Sarro et al. 2010). Clinical cure is often achieved with the used therapy (Noli & Auxilia 2007, Paradis et al. 2012), nevertheless the patients still may continue to carrier the Leishmania (Geisweid, Mueller, Sauter-Louis, Hartmann 2012, Pennis et al. 2005, Ikeda-Garcia et al. 2007, Manna et al. 2008).
Conclusions
According to the study results not all the patients had exhibited clinical improvement at the end of 30 days of therapy. Although at the end of the study most of the patients had no variations in the initial titers of anti-Leishmania antibodies (Pennisi et al. 2005a, Pennisi et al. 2005, Ikeda-Garcia 2007), it was possible to notice differences between the FRG and SRG regarding to variations on the PT, β-globulin, and γ-globulin fractions of proteinogram. Thus, these parameters in association with clinical assessment should be considered as an indicator and a simple way to appoint the efficacy response of the patients to the therapy.
Acknowledgments
The authors thank to Centre for Interdisciplinary Research in Animal Health – CIISA, of Faculty of Veterinary Medicine of Lisbon, of the University of Lisbon – Portugal (FMV-ULisboa); to Journal Veterinary Healthcare for publishing without any charges, and to Anjos of Assis Veterinary Medicine Centre (CMVAA), Barreiro – Portugal
Conflict of interest and source of funding statement
None of the authors of this paper has a financial or personal relationship with other people or organizations that could inappropriately influence or bias the content of the paper. This research received no specific grant from any funding agency in the public. commercial. or not-for-profit sectors.