Abstract
Four cases are reported with splanchnic aneurysms of the branches of the main arteries. Three of the cases presented as emergencies. Possible rupture was present in Case 2 and true rupture in Case 4. The etiology of Cases 1 and 2 may have been a floxacin antibiotics, Table 1. This report is the first clinical chronological association of the antibiotics and arterial and aortic pathology. This association was supported by nationwide research by Pasternak, 11. Detailed experimental work done on mice showed connective tissue fragmentation and arterial cell injury. Apparently, the above antibiotic induced mitochondrial DNA damage and dysfunction, 9.
Author Contributions
Academic Editor: Qiang Cheng, Biomedical Informatics Institute, and Computer Science Department, China.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Nicholas J. Demos et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The patient in Cases 1 and 2 gives full permission for the use of his medical history and we have patient consents for Cases 3 and 4.
Case 1
An 84 year old male had an elective percutaneous stent graft treatment of right internal iliac aneurysm in 2014. The 4cm in diameter aneurysm had been detected as an incidental finding in 2011, Figure 1. The CT scan also revealed abdominal aortic and internal carotid dilatations as well as a small mesenteric aneurysm was also present. He had received a six day course of 400mg Avelox (Maxifloxacin) on December 24, 2006. Levaquin (Livofloxacin) was received for six days on February 27, 2012, both courses several years before 2011, Table 1.
Figure 1. Case 1 – Right Internal Iliac Aneurysm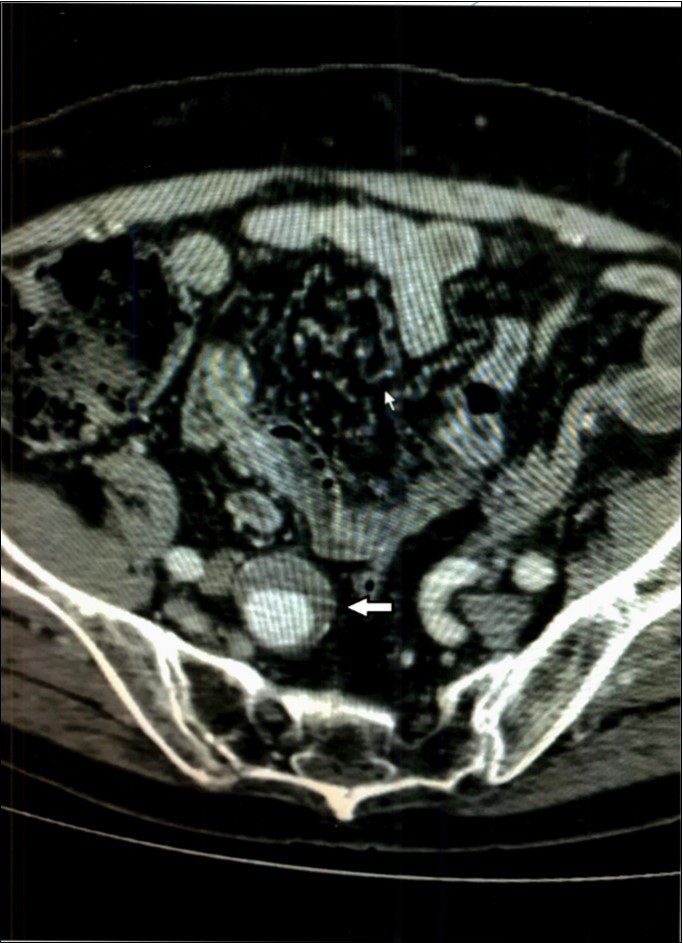
Case 2
On August 31, 2016 an 86 years old man was admitted complaining of acute generalized abdominal pains of 18 hours duration. In the afternoon of the previous day, he suffered upper abdominal pains with vomiting and repeated eructations. No point tenderness was present. He was afebrile.
Complete metabolic panel was normal with normal hemogram. Immediate computed tomography (CT scan) revealed a 1.5 x 2 centimeter mesenteric aneurysm, possibly ruptured, Figure 2, as well as two smaller aneurysms a few millimeters each in diameter and abdominal aortic and carotid dilatation. A few small galls stones were seen. Immediate percutaneous embolization of the large aneurysm was performed two days before the procedure and six days afterward he received Levaquin. Follow up CT scan of the abdomen 18 months later showed the embolized mesenteric aneurysm and no change in the smaller ones. The symptoms have not recurred two years later.
Figure 2. Case 2 – Superior Mesenteric Artery Branch Aneurysm.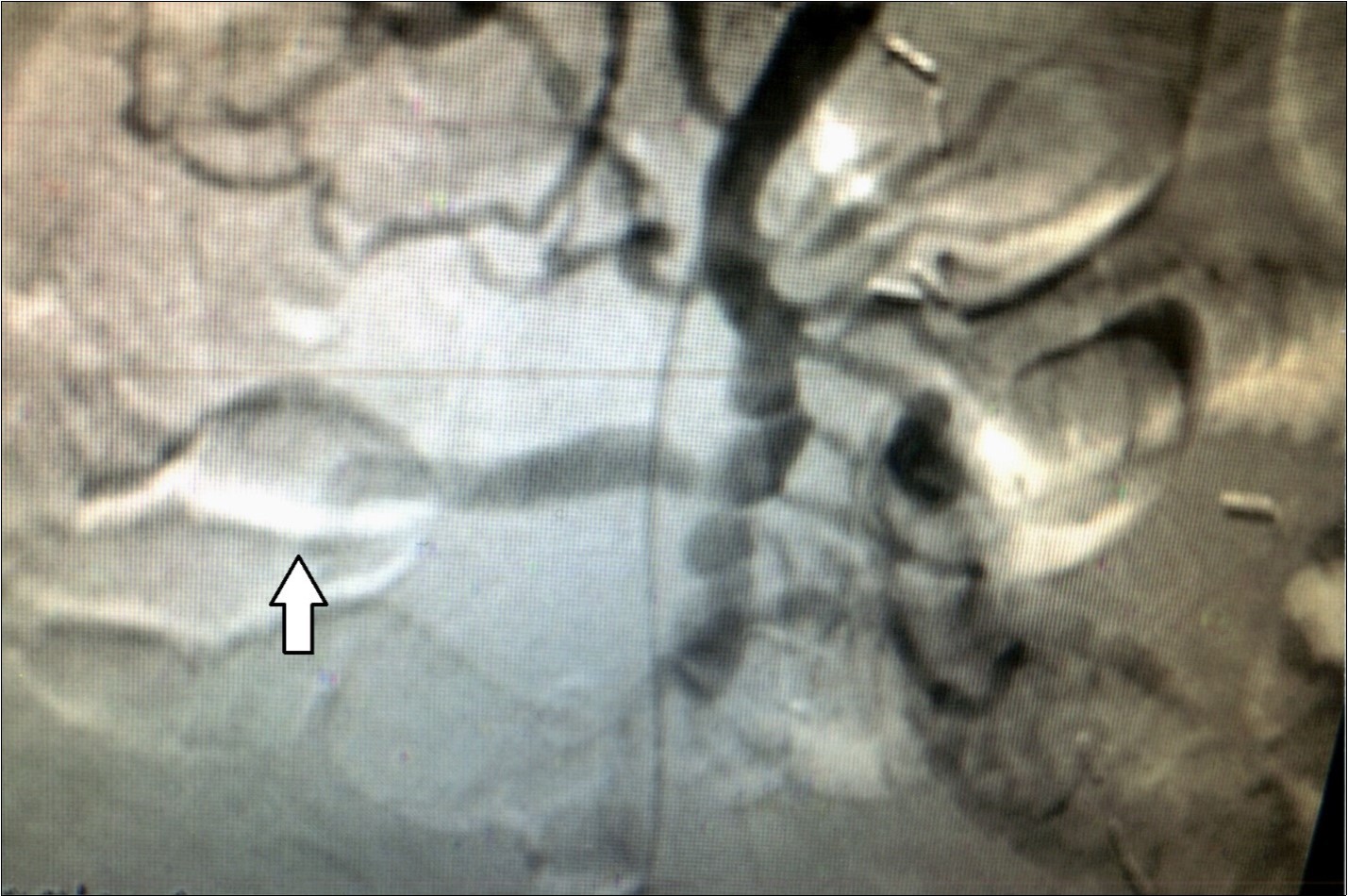
Case 3
A 66 year old man was admitted to Christ Hospital in Jersey City, New Jersey, complaining of abdominal and back pain and weakness of at least one month duration. He had lost 40lbs of weight. Physical examination revealed mild mid abdominal tenderness and mental confusion. The temperature was 97.9. White blood count was 10.3 thousand per microliter. Computed tomography of the abdomen showed a 1.5 x 1.6 centimeter aneurysm of a branch of the superior mesenteric artery surrounded by some “inflammatory” reaction, Figure 3. Small stones were noted in the gall bladder. Immediate percutaneous embolization of the aneurysm was performed. CT scan of abdomen was “normal” before the present admission.
Figure 3. Case 3 – Superior Mesenteric Artery Branch Aneurysm surrounded by a halo.
On the day following admission blood cultures showed enterococcus faecalis treated with Ampicillin and Ceftriaxone. Six days later the blood culture was negative. He was discharged on the following day. He has been well for one year postoperatively. Now he is lost to follow-up.
Case 4
A 50 year old immune compromised patient was admitted to Bayonne Hospital on July 15, 2018, with severe gastrointestinal bleeding and anemia requiring six units packed red cells, two units of platelets and 2 units of fresh frozen plasma. Endoscopy revealed massive upper GI bleeding from duodenal ulcer. Epinepherine injection of the ulcer did not stop the bleeding. Percutaneous arteriogram revealed an aneurysm of the right hepatic artery bleeding into the first part of the duodenum wall. It was embolized, Figure 4. Past history revealed AIDS, Syphilis and tuberculosis. He had been on ventilator which was discontinued several days later. He is still hospitalized to treat his infections and a great deal of confusion, six weeks later. He is presumed deceased.
Figure 4. Case 4 –Hepatic Artery Aneurysm
Discussion
Older reviews of the mesenteric artery such as the one by Demos and colleagues of 42 medical school cadavers and by Jackson in patients, failed to detect aneurysm, 2, 3. Case reports of splanchnic aneurysm have appeared in the last 25 years, 4, 5. Endovascular treatment, such as performed in our four patients, has been stressed by Kasirajan and associates, 6.
Splanchnic aneurysms are reported to be emergencies in 22% of cases, with a mortality of 8.5%, 4. Abdominal pain, followed by CT scan in each of our last three patients. Prompt embolization was performed by percutaneous technique. One can speculate as to the incidental presence of the gall stones causing the pain, perhaps causing injury to the aneurysm as well, Case 2.
In our second patient, Case 2, in addition to the aneurysm, the CT scan indicated “probable” bleeding, Figure 2, without any sign of systemic bleeding or infection, clinically or in the hemogram. The blood cultures were normal six days after treatment. White blood cell counts were normal and only mild anemia was present. Therefore, it is doubtful the aneurysm was mycotic. The “halo” around the aneurysm can be interpreted as pressure effect of the enlarging aneurysm on the surrounding tissues.
In one reported case, Wakana and colleagues found signs of systemic infection and “injected” mural thrombi in an ileocolic aneurysm calling the hallo effect as “dirty fat”, 7.
The etiology of visceral aneurysm has been discussed as inflammatory, infectious, arteriosclerotic or congenital, 8.
Our 4 cases seem to have infections-inflammatory origins. Case 2 is probably arteriosclerotic. Cases 1 and 2 can be classified as arteriosclerotic with a possible deleterious component: Levaquin (generic Levoflaxim) may have been associated with these two aneurysms, 1, Table 1.
Table 1. Chronology of Medications* and Events**| Medication | 2006 | Avelox (Maxifloxacin) |
| Event | 2011 | Diagnosis of Right Internal Iliac Aneurysm |
| Medication | 2012 | Levaquin (Lebofloxacin) |
| Event | 2014 | Embolization of Right Internal Iliac Aneurysm |
| Medication | 2016, March 5 | Levaquin |
| Medication | 2016, August 2 | Levaquin |
| Events | 2016, August 29 | 1) Cat Scan: |
| - Aneurysm branch SMA*** | ||
| -Two smaller aneurysms branch SMA*** | ||
| -Dilatation of abdominal aorta and carotids | ||
| 2) Emergency embolization of aneurysm branch SMA*** |
Our patient received Avelox (Moxifloxacin) on December 24, 2006 and Levaquin (Levofloxacin) on February 27, 2012, each for several days each. In 2011, an internal iliac aneurysm was detected incidental to a CT scan of the abdomen and pelvis. It was percutaneously embolized on January 7, 2014.
This patient received additional two courses of Levaquin on March 15, 2016 and August 2, 2016. After intense abdominal pain on August 31, 2016, CT of the abdomen and pelvis revealed a “possible ruptured” mesenteric aneurysm which quickly was embolized percutaneously, with good recovery to date.
The aneurysm effect of Flocaxin antibiotics was recently supported by the experimental production of aneurysm on mice, 9. Ciprofloxacin fed in mice produced elastic fiber fragmentation and aortic cell injury. There was suppression of cell proliferation and induction of cell death. The antibiotic induced mitochondrial DNA damage and dysfunction, 9. A commentary of the above article advised not using a Fluoroquinone to treat infections, 10. Nationwide research supported evidence of Fluoroquinone toxicity by Pasternak et al, as well, 11.
The authors of this article are indebted to the following persons for their editorial contributions: Tara Jane Becker, Medical Assistant and Ioanna Agams, PhD and to physicians Clifford Sales and Mark Kumar for prompt diagnosis and treatment of Case 2.