Abstract
A reflective piece touches on core physiological concepts and experimental approaches, linking basic mechanisms to clinical insight and education.
Author Contributions
Academic Editor: Maheshkumar Kuppusamy, Department of Physiology, Sri Ramachandra Medical College and Research Institute, Chennai
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Kenneth Warring-Davies
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Physiology is one of the most captivating subjects to be studied and involved in, the number of Nobel Prize winners in physiology and medicine substantiates this fact
Research Physiologist have the privilege of being involved in many physiological research projects. For example, cardiovascular physiology leading on to advances in pacemaker technology, open heart surgery by pass perfusion techniques, cardiac intensive care medicine, resulting in saving many patients lives.
Research physiologist need intuitive, creative, inventive mind sets. For example, producing a unique complete set of haemodynamic empirical physiological formulae inside of HeartSmart®, a major change in our understanding of how the heart and lungs regulate and optimise blood, forming a new method of being able to calculate blood flow and pressures in the heart and lungs (haemodynamics), to guide intravenous infusion using vaso - active drugs and inotropes non - invasively at bedside (resuscitative early goal directed therapy), especially in patients suffering from sepsis-shock or any other serious medical or surgical condition.
The non - invasive HeartSmart® methodology is a disruptive destructive technology to existing haemodynamic monitoring methods.
HeartSmart® can be taught to the most junior members of medical and nursing staff, making haemodynamic monitoring a routine bedside procedure, with many benefits to healthcare providers and most importantly, saving countless numbers of lives, see Figure 5.
HeartSmart® is the only bedside paediatric haemodynamic monitor technology in the world.
Please see Figure 1 through Figure 7 below
Figure 1. Hales Haemodynamic Experiment Copyright Medics Limited
Figure 2. One of the Current Highly Invasive Haemodynamic Right Heart Catheters In -Situ Copyright Medics Limited
Figure 3. The Development of the Laws of Physics Underpinning the HeartSmart® Haemodynamic Cardiovascular Empirical Physiological Formulae Copyright Medics Limited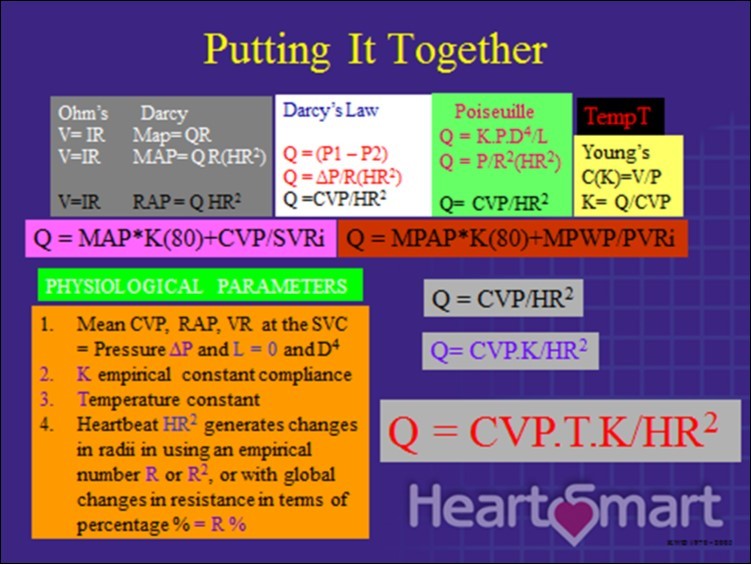
Figure 4. Developing the Value of K in the HeartSmart® Empirical Physiological Formulae Copyright Medics Limited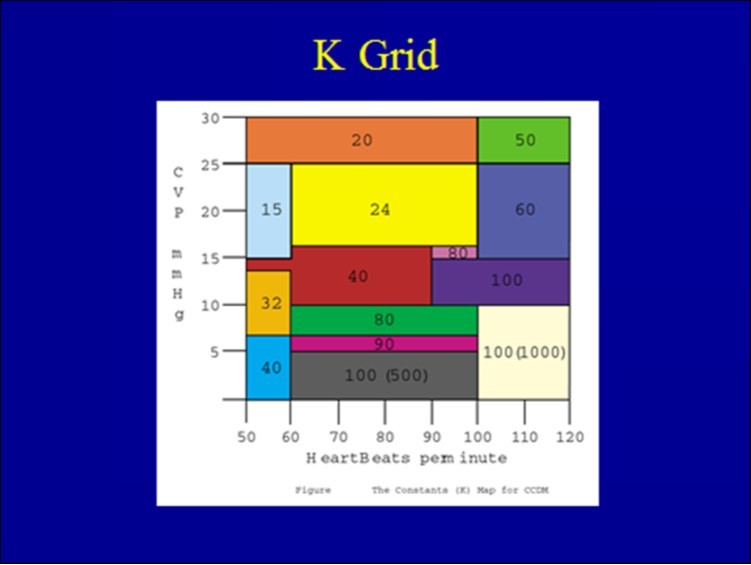
Figure 5. Flowchart Using Empirical Physiological Formulae in the Invasive and Non-Invasive HeartSmart® Haemodynamic Monitors Copyright Medics Limited
Figure 6. The Benefits of Routine Bedside Heamodynamic Monitoring Copyright Medics Limited
Figure 7. HeartSmart® Paediatric Monitoring Post Corrective Heart Surgery in the Cardiac Intensive Care Unit Copyright Medics Limited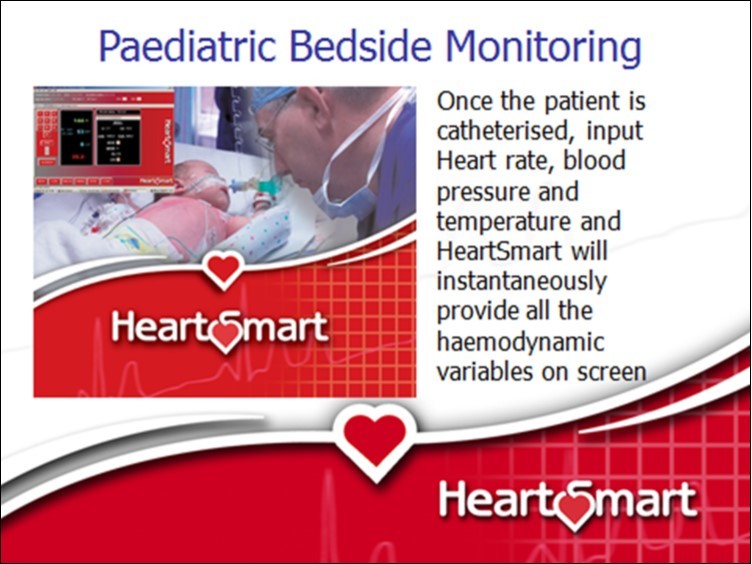
HeartSmart® can be used in many fields of medical research to advance medicine further, not least of all in the future, the potential for the production of an artificial heart not using human donors etc.
So what is the secret to being a research physiologist?
Many physiologist during their career will see in their minds eye, something that is of great interest which previously has not been observed.
Your gut feeling will intuitively tell you to investigate and question further this possible gem in physiology.
Take your time thinking through the design of your study, test and when sure the design is absolutely suitable, do NOT change it, reviewers are suspicious unless you can provide a good reason for change.
The ART of being able to use libraries to research publications in the field of interest, especially evidenced based trial results, then learning to join up the dots together with your research is absolutely critical when publishing convincing findings of fact. Additionally, as your knowledge from your research increases you may become more of a patho-physiologist in nature!
Medical statistics should be accurate and simple, if you don’t want to quickly lose the audiences interest when reading your manuscript.
More importantly if your not a medical statictian get the assistance of one.
Note making of all your doodling thinking moments is absolutely necessary, especially if your original eureka moment does not immediately work out and requires further endeavour.
Persistence and tenacity is a major component to achieve success.
Be prepared to have challenges made concerning your research results. Always remember others have to be able to reproduce your research data results.
What if your hypothesis does not work out?
This is still valuable intellectual property, because your findings inform other research physiologist that this avenue of research is not suitable for further investigation.
It is this capacity to think outside of the box of conventional understanding that makes a research physiologist.
Professional jealousy or institutional thuggery takes courage to face! Galileo and the Curie’s are typical examples of hundreds of such encounters.
The best advice is to totally ignore such debates from so called experts or critics, unfair destructive verbal diarrhoea! Remember you probably know more about your subject than they, so, let your published work speak for you. Publish publish in any media, posters, manuscripts and at conferences etc.
For example, see the diagram of Stephen Hales below a prolific cardiovascular physiologist and medical inventor, Figure 1
Keep your intellectual property thinking and research to yourself. Do not disclose to ANYONE until they sign off a Non Disclosure Agreement.
Patenting, if your work leads on to an invention, for example HeartSmart®, making an application which relatively cheap through a well established firm of patent lawyers, check the firm out do not get convinced by smooth talkers that you should immediately as urgent priority engage their services.
The other very useful tool is to use a major library services. For example Leeds library, that has an enourmous intellectual property patent section.
These librarians are “golden”, they can search databases to search for any other patents to see if a similar one or not has been patented etc. They can assist you in giving advice filling out patent applications, and here is another valuable tip.
When application is filed you have a year before the Patent Office discloses your application in a public domain gazette. It is permissible to pull out your application just before the filing date ends and then immediately refile the application. The disadvantage is you lose the filing priority date. This procedure can be repeated again and again, until you have a commercial partner in place. Hence having a filed application your invention is protected, some applicants use this protective advantageous technique all the time for years as seen on products “patent applied for”.
Best of all, library services are usually FREE OF CHARGE or extremely cheap, providing great invaluable services.
Patient consent with institutional ethical approval in accordance with the Helsinki Convention is a legal requirement.
Without institutional and patient consent peer review medical journals will not accept your manuscript for publication.
Finally, publishing your finished work in peer review journals is crucial to obtaining the recognition for your hard endeavours, but it is challenging as it is rewarding.
For example, see references below.