The Role of BCL-2 and BAK Genes in Chronic Kidney Disease and Haemodialysis Patients
Abstract
Background:
Polymorphonuclear leucocytes are the first line of defence against foreign invaders and constitute the major cell type involved in certain types of acute and chronic inflammatory diseases.
Aim of the Work:
The aim of the present study was to investigate the changes in expression of BCL-2 and BAK genes by real time PCR and to study whether they were involved in the accelerated neutrophil apoptosis which might be responsible for the recurrent bacterial infections seen in chronic renal disease and hemodialysis patients. Subjects and Methods: This study was conducted on sixty two subjects. Patients were selected from those admitted to Theodor Bilharz Research Institute (TBRI). Patients under study were classified into three groups; CKD patients (group I) kept on conservative treatment (22 cases), ESRD patients (group II) maintained on dialysis therapy, HD (20 cases). In addition, twenty healthy individuals served as a control group (group III) were involved. Results: There was significant increase in level of BAK gene in both patients' groups compared to control group with more increase in CKD group than ESRD group. Significant difference between the 3 groups was encountered with a higher expression level in CKD and ESRD groups than controls. There was decrease in level of BCL2 gene in both groups less than control group with more declines in ESRD group than CKD group.
Conclusion:
Bcl2 and Bak genes could have a role in survival and apoptosis of the studied groups and suggested their impact in controlling the inflammatory mechanisms and eventually their therapeutic potential.
Article Information
- Received
- Accepted
- Published
Academic Editor: Sebastian P. Galuska, Justus Liebig University Giessen
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Hanan Nour, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Samah Mohamed Abd, Elhamid, 48 Saudi buildings, Maadi —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
This study was processed in Kasr Al Aini main laboratory & TBRI, Hematology department. We thank our patients for their willing participation in our research.
Citation:
Introduction
Polymorph nuclear leucocytes PMNLs are the first line of defense against foreign invaders and constitute the major cell type involved in certain types of acute and chronic inflammatory diseases 1. The high frequency of bacterial infections in end stage renal disease (ESRD) patients suggests that PMNLs dysfunction may be involved in the immune deficiency observed among this patient population 2. PMNLs undergo programmed cell death through two major pathways; extrinsic and intrinsic3. Neutrophils are the most abundant cells of the innate immune system and are major players in the body's fight against infection. Neutrophils contribute significantly to the inflammatory response in normal physiology and there are important regulatory mechanisms that allow limitation and resolution of this response 4
Impaired function of apoptotic neutrophils was suggested as a disorder; results in high frequency of bacterial infections that are the main cause of hospitalization and mortality among haemodialysis patients5. In vitro studies have observed accelerated neutrophil apoptosis obtained from uremic and dialyzed patients. In addition, uremic plasma obtained from uremic and dialyzed patients accelerate apoptosis of neutrophils obtained from healthy donors5.
The BCL-2 family contains pro- and anti-apoptotic proteins that are found in the outer membranes of mitochondria. The balance between the pro- and anti-apoptotic members of this family is the central factor in the opening and closing of permeability transition pores 6 which is a critical pathway for cytochrome c release from mitochondria and causes apoptosis by activating caspase-97.
The present work was aimed to investigate the changes in gene expressions of proapoptotic BAK and antiapoptotic BCL-2 genes; members of the BCL-2 family which may be involved in the accelerated neutrophil apoptosis and hence recurrent bacterial infections seen in CKD and hemodialysis patients and to clarify their potential therapeutic benefit.
Patients and Methods:
Patients:
Sixty two participants were enrolled in this work. Selected patients were classified into 3 groups; group I included 22 patients suffering from chronic kidney disease (CKD) on conservative treatment with no previous history of dialysis, they composed of 13 females (59%) and 9 males (41%) with a mean age of 51.72±12.70. Group II included 20 end stage renal disease (ESRD) patients maintained on hemodialysis programs 3 sessions weekly; 4h each; for a period of ≥3 months, they were represented by 5 females (25%) and 15 males (75%) with a mean age of 56.41±11.62. In addition to group III encompasses 20 healthy individuals serving as control group, they were represented by 9 males (45%) and 11 females (55%) with a mean age value 28.90 ± 6.83. The procedures used in this study were approved by Theodor Bilharz Research Institute (TBRI) ethics committee according to Helsinki Declaration. The two patient groups were selected from the Nephrology Medicine department, Theodor Bilharz Research Institute (TBRI). The normal control group was recruited from the hospital staff. This study was conducted during the period from October 2013 to April 2014.
All participants were subjected to detailed history taking attributed mainly to bacterial infection anywhere; the onset of the disease to determine whether it is of acute or chronic onset, the underlying etiology of renal failure. Thorough clinical examination to exclude patients who have splenomegaly, hepatomegaly, jaundice, other signs of hepatic failure or any sign of autoimmune disease and laboratory investigations including complete blood count, kidney function tests, liver function tests, hepatitis markers (HBs Ag & HCV Ab) and special laboratory investigations (for patients and controls) for detection of hSC-reactive protein in the serum by ELISA technique and neutrophil apoptosis genes (Bcl2 and BAK) by real time polymerase chain reaction technique according to the method described by Livak.1999 8.
Methods:
Sample collection:
Ten milliliters of venous blood were collected from each patient and each individual of the control group by sterile venipuncture under complete aseptic conditions and divided as follows: 2 ml of venous blood on ethylene diamine tetra-acetic acid (EDTA) sterile vacutainer for performing complete blood picture, 5 ml on plain sterile vacutainer for performing KFT, LFT, hepatitis markers and hSCRP and 3 ml on EDTA for the study of neutrophil apoptosis genes (Bcl2 and BAK) by real time polymerase chain reaction technique.
Detection of HSC-reactive protein in serum with DRG diagnostic enzyme-linked immunosorbent assay (ELISA) as previously described.
Study of neutrophil apoptosis genes (Bcl-2 and BAK) by real time polymerase chain reaction technique
I. Neutrophil isolation
Leucocyte rich plasma was separated on a gradient of percoll after dextran sedimentation of RBCs. Percoll has a higher density than that of erythrocytes and granulocytes. Diluted blood is layered onto the density gradient (percoll). During the centrifugation process which follows, erythrocytes and granulocytes settle above the density gradient on account of their lower density
II. RNA isolation from neutrophils by using GeneJET Whole Blood RNA Purification Kit
III. Reverse transcription (Complementary DNA synthesis) by using Maxima First Strand cDNA synthesis kit
IV. Real time quantitative PCR
QuantiFast Probe Assays are predesigned assays based on hydrolysis probe detection (also known as TaqMan® assays). Each QuantiFast Probe Assay consists of a premixed primer pair and hydrolysis probe. Two dye labels are available: FAM™ (for all genes) and MAX™ (for selected reference genes). All QuantiFast Probe Assays are labeled with IBFQ (Iowa Black™ fluorescent quencher). IBFQ is a dark quencher with a broad absorbance spectrum ranging from 420 to 620 nm.
Kit for BAK gene assay (cat.no:QF00531048)
Kit for BCL2 gene assay (cat.noQF00301434)
The gene sequences for BAK, BCL-2, and ACTB were from the NCBI database (http://www.ncbi.nlm.nih.gov/Refseq)
Relative mRNA expression levels of BCL-2 gene (cat.noQF00301434) and BAK gene (cat.no:QF00531048) and ACTB gene (cat.no: QF00531209) were determined according to the 2-ΔΔCT method which asses fold change protein ratio calculated as follow: Calculation of the mean and standard deviation values of the sample results then we calculated the ΔCT value by ΔCT = CT target – CT reference. After that we calculated the standard deviation of the ΔCT value and the ΔΔCT value by ΔΔCT = ΔCT test sample – ΔCT calibrator sample. Then we calculated the standard deviation of the ΔΔCT value. Finally we incorporating the standard deviation of the ΔΔCT values into the fold-difference with 2–ΔΔCT
Statistical Analysis
Results for subjects’ demographic and clinical characteristics are given as means ± standard deviations (SD) for continuous variables and n (%) for categorical variables. Results for mRNA expression and apoptosis percentages are given as means ±SD and median. For continuous variables, groups were compared using a two-sample t-test or a Mann–Whitney U test if data were not normally distributed. A Pearson chi-square test was used for categorical variables. Comparison between more than two groups was done by ANOVA test. Statistical significance was set at P < 0.05. Statistical analyses used SPSS 15.0 software.
Declaration of Ethics
Oral and written informed consent was obtained from all patients according to Helsinki guidelines of research ethics.
Results
The patient's and the control groups demographic, clinical and laboratory characteristics are summarized in Table 1.
Table 1. Demographic, clinical and laboratory characteristics of the 3 studied groups| Item | CKD group(No; 22) | ESRD group(No; 20) | Control group(No; 20) |
|---|---|---|---|
| Age (years)RangeMean ± SD | 29-7251.72±12.70 | 26-7056.41±11.62 | 21-4128.90 ± 6.83 |
| Sex no. (%)MalesFemales | 9 (41%)13 (59%) | 15 (75 %)5 (25 %) | 9(45%)11(55%) |
| Diabetic nephropathy no. (%)PresentAbsent | 10 (45 %)12 (55 %) | 9 (45 %)11 (55 %) | 0 (0 %)20 (100%) |
| Hypertensive nephropathyno. (%)PresentAbsent | 14 (64 %)8 (36 %) | 10 (50 %)10 (50 %) | 0 (0 %)20 (100%) |
| Lower limb oedema no. (%)PresentAbsent | 4 (18 %)18 (82 %) | 9 (45 %)11 (55 %) | 0 (0 %)20 (100%) |
| Oliguria no. (%)PresentAbsent | 1 (5 %)21 (95 %) | 3 (15 %)17 (85 %) | 0 (0 %)20 (100%) |
| Hb (g/dl)RangeMean ± SD | 6.20 – 14.209.65 ± 1.89 | 6.00 – 12.009.45 ± 1.80 | 12.00 - 15.7012.94 ± 1.29 |
| TLC (× 10³)RangeMean ± SD | 3.20-10.207.18± 2.00 | 1.70-8.806.23± 1.67 | 4.40 – 8.206.69 ± 1.11 |
| Platelets (× 10³ /cmm)RangeMean ± SD | 62.00-800.00283.68 ± 134.24 | 104.00 – 339.00216.35 ± 68.09 | 150.00 – 390.00236.09 ± 57.89 |
| Urea (mg/dl)RangeMean ± SD | 33.00-300.00140.54 ± 71.48 | 80.00 – 171.00118.65 ± 23.90 | 15.00 – 36.0023.27 ± 6.69 |
| Creatinine (mg/dl)RangeMean ± SD | 1.65-12.006.28 ± 2.79 | 1.20 – 9.065.81 ± 2.49 | 0.40 –1.000.67 ± 0.19 |
| HSCRP (mg/dl)RangeMedian | 0.80- 32.606.50 | 0.80 – 9.403.60 | 0.78 – 5.202.07 |
Expression levels of BAK and BCL-2 genes in CKD and ESRD groups showed an increase in expression level of BAK gene in both groups with higher level in CKD group than ESRD group. Median and mean values of BAK relative quantification (RQ) in CKD group were 1.17 and 2.01 respectively while median and mean values of RQ in ESRD group were 0.29 and 1.17 respectively. Level of BCL-2 shows low expression in both groups of patients with more declines in ESRD group than CKD group. Median and mean values of BCL-2 RQ in CKD group were 0.86 and 1.15 respectively and median and mean values of RQ in ESRD group were 0.32 and 0.9 respectively. Comparison of expression levels of BAK and BCL-2 genes in the 2 studied patient groups (Table 2).
Table 2. Statistical comparison of expression levels of BAK and BCL2 genes in the 2 studied patient groups| Item | CKD group(No; 22) | ESRD group(No; 20) | P value |
| BAK RQ | |||
| Range | 0.02 – 10.18 | 0.07 – 4.10 | |
| Median | 1.17 | 0.29 | 0.04 |
| Mean±SD | 2.01±2.2 | 1.17±1.51 | S |
| BCL2 RQ | |||
| Range | 0.04 – 3.61 | 0.02 – 3.42 | 0.1 |
| Median | 0.86 | 0.32 | NS |
| Mean±SD | 1.15±0.96 | 0.90±1.12 |
Comparison between CKD group and ESRD group subjects as regards expression levels of BAK and BCL-2 genes revealed a statistically significant difference between the two groups with a higher expression level of BAK gene in CKD than ESRD group (P= 0.04).
There was no statistically significant difference between the two groups regarding expression level of BCL-2 gene however a lower expression level of BCL-2 was elicited in ESRD than CKD group (P= 0.1).
Comparison of expression levels of BAK and BCL-2 genes in the 3 studied groups are shown in Table 3 & Figure 1,Figure 2, Figure 3.
Table 3. Statistical comparison of expression levels of BAK and BCL2 genes in the 3 studied groups| Item | CKD group | ESRD group | Control group | P value |
| (No; 22) | (No; 20) | (No; 20) | ||
| BAK RQ | ||||
| · Range | 0.02 – 10.18 | 0.07 – 4.10 | - | 0.05 |
| · Median | 1.17 | 0.29 | 1 | S |
| · Mean ± SD | 2.01±2.2 | 1.17±1.51 | 1.00±0.00 | |
| BCL2 RQ | ||||
| · Range | 0.04 – 3.61 | 0.02 – 3.42 | - | 1 |
| · Median | 0.86 | 0.32 | 1 | NS |
| · Mean ± SD | 1.15±0.96 | 0.90±1.12 | 1.00±0.00 |
Figure 1. Photography of Amplification Plot of housekeeping gene ACTB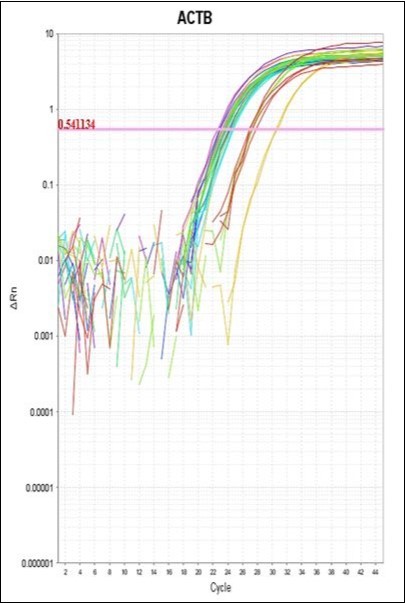
Download figure
Figure 2. Photography of Amplification Plot of BAK gene
Download figure
Figure 3. Photography of Amplification Plot of BCL-2 gene
Download figure
Comparison between CKD group, ESRD group subjects and controls as regards expression levels of BAK and BCL-2 genes revealed a marginally statistically significant difference between the 3 groups with a highest expression level of BAK gene in CKD than other two groups (P= 0.05).
There was no statistically significant difference between the 3 groups regarding expression level of BCL-2 gene however the lowest expression level was noticed among ESRD group than other two groups (P=1.00).
Comparison between CKD, ESRD and control groups as regards demographic and laboratory data (Table 4)
Table 4. Statistical comparison between CKD, ESRD and control groups as regards demographic and laboratory data| Items | CKD group (No; 22) | ESRD group (No; 20) | Control group (No; 20) | P value | |
| Age (years)RangeMean ± SD | 29-7251.72±12.70 | 26-7056.41±11.62 | 21-4128.90 ± 6.83 | 0.001HS | |
| Sex no. (%)MalesFemale | 9 (41%)13 (59%) | 15 (75 %)5 (25 %) | 9(45%)11(55%) | 0.001HS | |
| Laboratory data: | |||||
| Hb (g/dl)RangeMean ± SD | 6.20 – 14.209.65 ± 1.89 | 6.00 – 12.009.45 ± 1.80 | 12.00 - 15.7012.94 ± 1.29 | 1.20NS | |
| TLC (× 10³)RangeMean ± SD | 3.20-10.207.18± 2.00 | 1.70-8.806.23± 1.67 | 4.40 – 8.206.69 ± 1.11 | 1.25NS | |
| Platelets (× 10³ /cmm)RangeMean ± SD | 62.00-800.00283.68 ± 134.24 | 104.00 – 339.00216.35 ± 68.09 | 150.00 – 390.00236.09 ± 57.89 | 0.08NS | |
| Urea (mg/dl)RangeMean ± SD | 33.00-300.00140.54 ± 71.48 | 80.00 – 171.00118.65 ± 23.90 | 15.00 – 36.0023.27 ± 6.69 | 0.001HS | |
| Creatinine (mg/dl)RangeMean ± SD | 1.20 – 9.065.81 ± 2.49 | 1.65-12.006.28 ± 2.79 | 0.40 –1.000.67 ± 0.19 | 0.001HS | |
| HSCRP (mg/dl)RangeMedian | 0.80- 32.606.50 | 0.80 – 9.403.60 | 0.78 – 5.202.07 | 0.001HS | |
Comparison between CKD group, ESRD group and control group subjects as regards clinical and laboratory data revealed statistically significant difference between the three groups concerning age and sex distribution and urea, creatinine and HSCRP levels with more prevalent age and males distribution among ESRD than other 2 groups and highest levels of urea, creatinine and HSCRP in CKD group than other 2 groups (P=0.001). However non-significant changes between the three groups according to Hb level, TLC and platelet count were shown.
Comparison between ESRD and CKD groups as regards clinical and laboratory data (Table 5)
Table 5. Statistical comparison between CKD and ESRD groups as regards demographic, clinical and laboratory data| Items | CKD group (No; 22) | ESRD group (No; 20) | P value | |
| Age (years)RangeMean ± SD | 29-7251.72±12.70 | 26-7056.41±11.62 | 0.22NS | |
| Sex no. (%)MalesFemales | 9 (41%)13 (59%) | 15 (75 %)5 (25 %) | 0.001HS | |
| Clinical data | ||||
|---|---|---|---|---|
| Diabetic nephropathy no. (%)PresentAbsent | 10 (45 %)12 (55 %) | 9 (45 %)11 (55 %) | 1.00NS | |
| Hypertensive nephropathy no. (%)PresentAbsent | 14 (64 %)8 (36 %) | 10 (50 %)10 (50 %) | 0.53NS | |
| Lower limb oedema no. (%)PresentAbsent | 4 (18 %)18 (82 %) | 9 (45 %)11 (55 %) | 0.09NS | |
| Oliguria no. (%)PresentAbsent | 1 (5 %)21 (95 %) | 3 (15 %)17 (85 %) | 0.33NS | |
| Laboratory data | ||||
| Hb (g/dl)RangeMean ± SD | 6.20 – 14.209.65 ± 1.89 | 6.00 – 12.009.45 ± 1.80 | 0.72NS | |
| TLC (× 10³)RangeMean ± SD | 3.20-10.207.18± 2.00 | 1.70-8.806.23± 1.67 | 0.1NS | |
| Platelets (× 10³ /cmm)RangeMean ± SD | 62.00-800.00283.68 ± 134.24 | 104.00 – 339.00216.35 ± 68.09 | 0.06NS | |
| Urea (mg/dl)RangeMean ± SD | 33.00-300.00140.54 ± 71.48 | 80.00 – 171.00118.65 ± 23.90 | 0.19NS | |
| Creatinine (mg/dl)RangeMean ± SD | 1.65-12.006.28 ± 2.79 | 1.20 – 9.065.81 ± 2.49 | 0.56NS | |
| HSCRP (mg/dl)RangeMedian | 0.80- 32.606.50 | 0.80 – 9.403.60 | 0.001HS | |
Comparison between ESRD group and CKD group subjects as regards clinical and laboratory data revealed a highly statistical significant difference regarding sex distribution and HSCRP level. There was more prevalent females distribution and a higher level of HSCRP in CKD group (P=0.001) meanwhile there was no significant changes between the 2 groups in other clinical and laboratory data.
Discussion
PMNL apoptosis is an important mechanism regulating the extent of an inflammatory response, rendering it self-limiting thus preventing excessive tissue damage. At sites of inflammation, complex interplay between proapoptotic and survival signals must control the outcome of the response. Therefore, it is important to prevent a reduced immune function in the case of increased apoptotic cell death or a state of increased inflammation in the case of reduced PMNL apoptosis 9. PMNLs undergoing apoptosis are dysfunctional. This dysfunctional pattern is similar to that of uremic PMNLs, which demonstrate altered oxidative burst, impaired chemotaxis, aggregation and phagocytosis. Therefore it is possible to speculate that uremia induced apoptosis may be partly responsible for the PMNL dysfunction commonly encountered in patients with CRF 5, 10. The depression of the immune response in the uremic patient is global, including both humoral and cellular sectors. Accordingly, chronic hemodialysis patients are highly susceptible to infection with its sequel of morbidity and mortality. Moreover, the infections are sustained not only by opportunistic microorganisms but also by common bacteria10.
Furthermore, it has been noticed that immune system dysregulation in uremic patients may be accentuated by dialysis. In fact, during dialysis treatment cytokines and many other soluble uremic toxins may be partly responsible for a variety of functional disturbances that contribute to an increased risk of infection by interfering with essential functions of the non specific immune response such as chemotaxis, phagocytosis and oxidative metabolism 11.
The aim of this study was to investigate the changes in gene expressions of proapoptotic BAK and antiapoptotic BCL-2 genes; members of the BCL-2 family which may be involved in the accelerated neutrophil apoptosis which may play a role in the recurrent bacterial infections seen in CKD and hemodialysis patients and to clarify their potential therapeutic benefit.
The study was conducted on 62 participants classified into 3 groups; group I included CKD patients kept on conservative treatment with no previous history of dialysis (22 cases), group II included ESRD patients maintained on haemodialysis therapy (20 cases), both groups were selected from those admitted to the Nephrology Departments and Hemodialysis Unit, Theodor Bilharz Research Institute (TBRI). In addition, group III included healthy individuals served as a control group. All individuals enrolled in the study were subjected to the following routine investigations; complete haemogram, kidney function tests, liver function tests and hepatitis markers HBs Ag, HCV-Abs, HIV Abs. In addition, inflammatory state was evaluated by estimation of CRP using HSCRP ELISA technique. Basically, this work was undertaken to study changes in relative gene expression of BCL-2 and BAK genes in neutrophil by using real time quantitative PCR technique (RQ-PCR).RQ-PCR system is based on the detection and quantification of fluorescent reporter. This signal increases in direct proportion to the amount of PCR product in a reaction. By recording the amount of fluorescence emission at each cycle, it is possible to monitor the PCR reaction during exponential phase where the first significant increase in the amount of PCR product correlates to the initial amount of target template12.
In our study we utilized QuantiFast Probe Assays which are predesigned assays based on hydrolysis probe detection (also known as TaqMan® assays). Each QuantiFast Probe Assay consists of a premixed primer pair and hydrolysis probe. Two dye labels are available: FAM™ (for all genes) and MAX™ (for selected reference genes). All QuantiFast Probe Assays are labeled with IBFQ. IBFQ is a dark quencher with a broad absorbance spectrum ranging from 420 to 620 nm.
Detection of relative expression of BAK and BCL-2 genes were done using 2–ΔΔCT method which asses fold change protein ratio mentioned previously in methodology.
The present study revealed a statistically significant increase in the mean level of BAK gene (pro-apoptotic gene) in CKD group than in ESRD group (median values 1.17, 0.29 and mean values 2.01±2.2, 1.17±1.51 respectively) (P=0.04). Furthermore a marginally statistically significant difference between all patients groups (CKD, ESRD) and control groups was encountered with a higher mean expression level in CKD and ESRD groups than in controls (median values 1.17, 0.29 and 1 respectively) and (mean values 2.01±2.2, 1.17±1.51, and 1±0.0 respectively) (P= 0.05).These data means that BAK gene might play a role in acceleration of neutrophil apoptosis in uremic patients and consequently increases liability to recurrent bacterial infections known to occur among those patients.
In contrary to our findings Zhang et al. 13 who studied the role of BAK gene in delaying neutrophil apoptosis in chronic obstructive pulmonary disease, they reported relative reduction of BAK gene expression which prolong survival of neutrophil and consequently may be an important factor in the persistent inflammation associated with these patients. This difference could be attributed to the difference in patient's health problems, which may in turn responsible for release of factors that affect gene expression.
Our study revealed also that there was decrease in the expression level of BCL-2 gene (anti-apoptotic gene) in both groups of patients compared to the control group with more decline in ESRD group than CKD group (median value 0.32, 0.86,1 respectively and mean values1.15±0.96,0.90±1.12respectively).These difference were not statistically significant between CKD group and ESRD group (P= 0.1); as well as between the three studied groups and each other (P= 0.1).These data mean that BCL-2 gene may play role in neutrophil apoptosis in ureamic patients and its decline help in acceleration of neutrophil apoptosis. These findings are matched with those of Majewska et al. 14 who reported lower expression of BCL-2 protein in patients suffering from ESRD compared to controls (mean value 41.1±19.9, 27.7±13.9 respectively). Unlike the present data the authors found that the difference between two groups was statistically significant.
In contrast with the results of the present work concerning BCL-2 expression, Friedrich et al. 15 studied acute effects of haemodialysis on pro-/anti- apoptotic genes in peripheral blood leukocytes by analyzing transcript levels of the BCL-2, BCL2L2 and other genes using real time PCR technique, their study revealed no significant increase in gene expression levels of the analyzed BCL-2 and BCL2L2 during the HD treatment.
In agreement with the results of this work, Crokera et al. 16 studied the role of Bid, BAK and Bax as proapoptotic genes; BCL-2 and Mcl-1 as antiapoptotic genes in acceleration of Fas-mediated mice bone marrow neutrophil using microarray analysis. Results of their study show that Bid, BAK, and Bax accelerated Fas-mediated neutrophil apoptosis and BCL-2 and Mcl-1 inhibit Fas-mediated neutrophil apoptosis. This acceleration of apoptosis may be as a result of increased BAK and decreased BCL-2 expression in comparison to the control group which were recorded in this work.
Dounousi et al. 17 investigated levels of specific apoptotic and inflammatory markers across CKD stages on peripheral blood mononuclear cells. They demonstrated that expression of BCL-2 decreased significantly in the course of CKD. A change in BCL-2 expression in vitro has been shown in predialysis and dialysis patients compared with healthy controls, which was linked with immune defects, but not with renal function. The mechanism that leads to gradually lower BCL-2 expression in CKD as well as its clinical importance is poorly understood. It has been speculated that the diminished expression of BCL-2 is responsible for the failure of uremic lymphocytes to rescue from apoptosis.
Data obtained from the present work regarding increase in expression level of BAK gene which is proapoptotic gene were in accordance with those of Zahran et al. 6. They studied neutrophil apoptosis with technique other than PCR; by flowcytometry and light microscopy on the same three groups of the like ours. Neutrophil apoptosis was evaluated by estimation of Annexin V expression on neutrophil by flowcytometry. The authors contributed this increase in neutrophil apoptosis in part to neutrophil activation as they found positive correlation between the percentage of apoptptic neutrophils and neutrophil surface expression of CD 18 which was estimated in the same study.
Musiał & Zwolin´ska 18 studied new markers for apoptosis E-cadherin, extracellular matrix metalloproteinase inducer (EMMPRIN) and matrix metalloproteinase (MMP)-8 in serum using ELISA technique. They revealed for the first time elevation of E-cadherin, EMMPRIN and MMP-8 concentrations in children with CKD, pointing at their potential role as markers of apoptosis in patients with different stages of CKD, higher in pre-dialysis patients than in controls and increased progressively with renal failure aggravation. These results were also in accordance with our results though the techniques are different.
Our study was in agreement with those of Preiananagam et al. 19; Sardenberg et al. 20 and Cohen et al. 10 who reported that uremic toxins seemed likely to play an essential role in PMNL apoptosis and that dialysis may correct or normalize apoptosis rates. Consistent with this notion Kennedy and DeLeo 21 stated that it is possible that the existence of mixture of a large number of various toxic uremic solutes in serum of ESRD patients may accelerate neutrophil apoptosis. Also, they speculated that each uremic toxin has distinct effects on PMNL viability and function. Cohen et al. 10 reported that uremia induced apoptosis may be partly responsible for the PMNLs dysfunction commonly encountered in patients with CRF.
Among several different inflammatory biomarkers, CRP is said to independently predict mortality in CKD patients 22. It is a marker of low-grade chronic inflammation. It had been shown to be such a strong predictor of cardiovascular mortality in the general population, suggest that the association between inflammation and atherosclerosis is particularly strong in uremic patients. It can be considered as independent determination of hospitalization in HD patients 23. In the present work, estimated serum HSCRP in the studied patients showed that CKD group had highly significant increase level when compared to ESRD group (P=0.001).Both had highly significant increase compared to control group (P=0.001). (Ranges: 0.80- 32.60, 0.80 – 9.4 and 0.78 – 5.20 & medians: 6.50, 3.60 and 2.07 respectively). These data confirm a state of low grade chronic inflammation among the studied patients.
These findings are in agreement with those of Abraham et al. 24 who reported that high rate of inflammation in non- dialysis patients as seen by HSCRP levels. Lee et al. 25 results suggest that correction of uremic milieu through dialysis has beneficial effects. Therefore, initiation of dialysis might have the advantage of improving inflammatory and nutritional status, and correcting immune dysfunction in ESRD patients. They studied HSCRP which was high in uremic patient and improved with starting dialysis.
Zahran et al. 5 studied serum level of CRP using semiquantitive latex technique in the same three groups like the groups we have studied in additional to two groups CKD with infection and ESRD with infection. They showed that there was significant increase when the CKD and HD groups were compared with control group, and CKD with infection and HD with infection had highly significant increase compared to CKD, HD and control groups. Therefore, the association of a micro inflammatory state and uremia could be speculated, and might further be aggravated by the superimposed infection.
Assessment of the kidney function tests revealed that serum creatinine level reached the peak of elevation in the CKD group followed by ESRD and both groups showed highly significant increase when compared to control group (6.28 ± 2.79, 5.81 ± 2.49 , 0.67 ± 0.19 respectively P=0.001). Also serum level of urea reached the peak of elevation in the CKD group followed by ESRD and both groups showed highly significant increase (P= 0.001) compared to control group(140.54 ± 71.48, 118.65 ± 23.90 m , 23.27 ± 6.69 respectively).
Comparison between CKD, ESRD and control groups as regards mean age values (51.72±12.70 ; 56.41±11.62 ; 28.90 ± 6.83 respectively ) and sex distribution revealed statistically significant difference between the three groups with more prevalent age and males distribution among ESRD group than other 2 groups (P=0.001). Comparison between CKD and ESRD groups as regard sex distribution revealed a highly statistical significant difference with more prevalent females in CKD group. Most of other studies on neutrophil apoptosis like revealed no statistical significant difference as regard demographic data 5.
Conclusions
So regarding our study in uremic patients there was an increased BAK gene expression which is proapoptotic gene to a higher level in CKD group than ESRD group. On the other hand there was a decrease in expression level of bcl2 gene which is antiapoptotic gene with a level lower in ESRD compared to CKD group. These finding suggested a role of these two genes in acceleration in rate of neutrophil apoptosis and hence decrease in their life span. These finding through the light on the role of evaluated genes in survival and apoptosis of the studied groups and suggested their impact in controlling the inflammatory mechanisms and eventually their therapeutic potential.
Ethical approval
All procedures performed in this study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study is approved by Theodor Bilharz Research Institute ethical committee (TBRI-IRB number 01/16).
References
- 1.Witko-Sarsat V, Rieu P, Descamps-Latscha B, Lesavre P, Halbwachs-Mecarelli L. (2000) Neutrophils: molecules, functions and pathophysiological aspects. , Lab Invest 80(5), 617-53.
- 2.Sarnak M J, Jaber B L. (2000) Mortality caused by sepsis in patients with end-stage renal disease compared with the general population. , Kidney Int 58, 1758-1764.
- 3.Jaber B, Perianayagam M, Balakrishnan V, King A, Pereira B. (2001) Mechanisms of neutrophil apoptosis in uremia and relevance of the Fas (APO-1, CD95)/Fas ligand system. , Journal of Leukocyte Biology 69, 1006-1012.
- 4.Hallett J M, Leitch A E, Riley N A, Duffin R, Haslett C et al. (2008) Novel pharmacological strategies for driving inflammatory cell apoptosis and enhancing the resolution of inflammation. , Trends Pharmacol Sci 29, 250-257.
- 5.Zahran N, William I, Sayed A, Zahran M, Sabry O et al. (2012) Granulocyte macrophage colony stimulating factor mediated modulation of polymorphonuclear leukocyte dysfunction in chronic kidney disease and hemodialysis patients. , Journal of American Science 8(6), 731-73.
- 6.Zahran N, Sayed A, William I, Mahmoud O, Sabry O et al. (2013) Neutrophil apoptosis: Impact of GM-CSF on cell survival and viability in chronic kidney disease and hemodialysis patients. In press; accepted in:Arch MedSci.(AMS-0.183-2011-02)
- 7.B Van Raam, Verhoeven A J, Kuijpers T W. (2006) Mitochondria in neutrophil apoptosis. , Int J Hematol 84, 199-204.
- 8.Livak K J. (1999) Allelic discrimination using fluorogenic probes and the 5′ nuclease assay. , Genet Anal 14, 143-149.
- 9.Pluskota E, Soloviev D, Szpak D. (2008) Neutrophil Apoptosis: selective regulation by different ligands. , of Integrin α M β2 (Mac-1). J Immunology 181, 3609-3619.
- 10.Cohen G, Raupachova J, Wimmer T, Deicher R, Horl W. (2008) The uremic retention solute para-hydroxy-hippuric acid attenuates apoptosis of polymor-phonuclear leukocytes from healthy subjects but not from hemodialysis patients. , Nephrol Dial Transplant 23, 2512-2519.
- 11.Banche G, Allizond V, Giacchino F, Mandras N, Roana J. (2006) Effect of dialysis membrane biocompatibility on polymorphonuclear granulocyte activity in dialysis patients. , Nephrol Dial Transplant 21, 3532-3538.
- 12.Hongbao M. (2005) Development of Polymerase Chain Reaction (PCR). , The Journal of American Science 1(3), 512.
- 13.Zhang J, He J, Xia J, Chen Z, Chen X. (2012) Delayed apoptosis by neutrophils from COPD patients is associated with altered bak, bcl-xl, and mcl-1 mRNA expression, Diagnostic Pathology. 7, 65.
- 14.Majewska E, Baj Z, Sulowska Z, Rysz J, Luciak M. (2003) Effects of uremia and hemodialysis on neutrophil apoptosis and expression of apoptosis related protiens. , Nephrol Dial Transplant 18(12), 2582-8.
- 15.Friedrich B, Janessa A, Schmieder R, Risler T, Alexander D. (2008) acute effects of haemodialysis on pro-/anti- apoptotic genes in peripheral blood leukocytes;. , Cell PhysiolBiochem 22, 423-430.
- 16.Crokera B, O’Donnella J, Nowellc C, Metcalfa D. (2011) Fas-mediated neutrophil apoptosis is accelerated by Bid, Bak, and Bax and inhibited by. Bcl-2 and Mcl-1 ; PNAS 108(32), 13135-13140.
- 17.Dounousi E, Koliousi E, Papagianni A, Ioannou K, Zikou X. (2012) Mononuclear Leukocyte Apoptosis and Inflammatory Markers in Patients with Chronic Kidney Disease. , Am J Nephrol 36, 531-536.
- 18.Musiał K, Zwolin´ska D. (2013) New markers of apoptosis in children on chronic dialysis. , Apoptosis 18(1), 77-84.
- 19.Perianayagam M, Balakrishnan V, Guo D, Pereira B, Jaber B. (2003) Quantification of Bax and Bcl2 in polymorphonuclear leukocytes from haemodialysis patients: relation to hydrogen peroxide. , Euro J Clin Invest 33, 905-911.
- 20.Sardenberg C, Suassuna P, Andreoli M C, Watanabe R, Dalboni M A. (2006) Effects of uraemia and dialysis modality on polymorphonuclear cell apoptosis and function. , Nephrol. Dial. Transplant 21, 160-165.
- 21.Kennedy A, DeLeo F. (2009) Neutrophil apoptosis and the resolution of infection. , Immunologic Research 43(3), 8049-6.
- 22.Stenvinkel P. (2006) C-reactive protein--does it promote vascular disease?. , Nephrol Dial Transplant 21(10), 2718-20.
- 23.Panichi V, Scatena A, Migliori M, Marchetti V, Paoletti S. (2012) . Biomarkers of Chronic Inflammatory State in Uremia and Cardiovascular Disease, Hindawi Publishing Corporation.2012 360147.
Cited by (4)
This article has been cited by 4 scholarly works according to:
Citing Articles:
Biomolecules (2026) Crossref
BMC Nephrology (2025) OpenAlex Crossref Semantic Scholar
Frontiers in Veterinary Science (2023) OpenAlex Crossref Semantic Scholar
Molecular Biology Reports (2022) OpenAlex Crossref Semantic Scholar