
Ice Water Immersion as an Additional Method in Physiology Recovery in the Sport
Abstract
Objective:
Soccer has a reduced overall recovery time. If these situations are not properly controlled they can cause the athlete chronic fatigue, an increase in delayed-onset muscle soreness (DOMS) and thus result in a decrease in athletic performance. There are several therapies that have attempted to improve athletic performance, decrease the percentage of injuries and results in soccer. Training and recovery instances are opportunities to find ways to address this issue. Understanding the physiology of recovery is essential to accelerate some processes, with the aim of shortening the times.
Subjects:
Cryotherapy could improve functional performance tests and decrease pain in soccer players. Our work design is an experimental prospective study.
Method:
Twenty subjects (10 experimental subjects and 10 control group subjects), between the ages of 17 and 23, who are members of a university men's soccer team, participated in the study. The following variables were controlled: power; the number of jumps, the average height of a jump in a 30-second continuous jump test, and DOMS perception through visual analog scale (VAS). Both groups shall be subjected to a more active recovery as well as elongation carried out by the coaching staff. In addition to this, the experimental group shall also be subjected to ice baths (42-47 °F) for three minutes.
Results:
We found significant statistical differences in the number of jumps and the power of the same in the control group, thus obtaining improvements. No significant differences were observed in either group for the average jump height and percentage yield variables. In the assessment of DOMS significant differences were observed, with a lower perception of DOMS seen in the experimental group.
Conclusion:
Ice baths provide favorable results in some aspects of the 30-second continuous jump test, decreasing the perception of leg pain and fatigue, and therefore they can be considered a valid alternative in the management of these athletes.
Article Information
- Received
- Accepted
- Published
Academic Editor: Nasim Habibzadeh, Teesside university, UK.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Jair, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Jaime Hinzpeter, Medical Doctor, University of Chile, Clinical Hospital, Santos Dumont 999, Santiago Chile —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
This study was developed at Sports Center of the National Football Association (ANFP)
Citation:
Introduction
Soccer is considered an acyclic sport, with intermittent motion characteristics, open skills and highly complex when compared to others. Furthermore, it has a high endurance component, with variations in the intensity, and incomplete recuperation periods within a game20.
Soccer workouts are performed on a daily basis, with regular competitions and short recovery times. This entails that the athletes are under constant risk of fatigue and an increase in delayed-onset muscle soreness (DOMS). If the latter is added to an insufficient training plan and above all, if the recovery methods and time invested in these are unsuitable, a decrease in athletic performance may occur.
When reviewing the literature that supports the use of Cryotherapy, we found that few studies have successfully related variables such as performance parameters, types of exercises and intensity of the same, water temperature, duration, and depth of the bath, recovery time and the subsequent effects on the performance of the athlete.
Cryotherapy, whether as a local or systemic application, is the most commonly used superficial thermotherapy physical agent due to the fact that it is a low-cost therapeutic method that is easy to use, requires little preparation time and has limited adverse effects. Among the physiological effects described in the literature, the following were found: a decrease in skin temperature, direct local vasoconstriction generated when the subcutaneous temperature falls below 59 °F19, a decrease in oxygen consumption at temperatures close to 50 °F in which a decrease in metabolic enzyme activity is also obtained7, a decrease in leukocyte migration, influence on the muscle pain-spasm cycle generating analgesia due to a decrease in nerve conduction and receptor activity by competitive inhibition within the CNS, or a combination of both mechanisms22.
The aim of our study is to apply Cryotherapy as a recovery method after strenuous exercise and compare the results obtained after this therapy.
Methods
Prospective Study. Prior written consent, the evaluation was performed on the Metropolitan University of Educational Sciences men’s soccer team. The initial study population consisted of 31 male participants, ages 17 to 23, of which 3 were excluded due to injuries that occurred within the evaluation period, 7 did not meet the minimum criteria of proposed attendance (four evaluations), and 1 was excluded since he exceeded the age limit. The 20 participants were randomly distributed by lot into 2 groups, In this study, we have the approval of the Ethics Committee of the Clinical Hospital University of Chile for the research obtained in all participants.
a. Control group: 10 subjects who performed the training program established by the coaching team. Within the core part of the training session, the subjects executed a continuous jump test for thirty seconds on a diving platform, yielding both the number of jumps as well as the average height of the jumps by each subject. Once the test has been fully executed, the subjects are requested to continue with their group activities. Once the training session has been completed, the athletes will participate in an active recovery as well as elongations established by the coaching team.
b. Experimental group: 10 subjects who in addition to performing the aforementioned for the control group were further subjected to an ice bath at a controlled temperature ranging from 40-47 °F.
During the jump evaluation, parts of the Bosco tests were administered consisting of the following: Squat Jump, Counter Movement Jump (CMJ), and continuous jumps for 30 seconds.
Cryotherapy was based on immersion baths with the following characteristics: the baths were performed in ice water, immersing the lower limbs up to the anterior superior iliac spines. The dose shall consist of an immersion for 3 minutes at a water temperature between 40-47 °F.
Statistical Analysis
Statistical analyses included the Shapiro-Wilk (1965) normality tests for (n less than ≤ 50), (28) in order to be able to prove the type of data distribution in accordance with the criteria of some authors10. In the case in which the data was not distributed normally, the comparisons between treatments were performed using the nonparametric test of comparison of Mood medians (IDEM)12. The level of significance used was α = 0.05. The results were analyzed with the Stata 12 program.
With regards to the characteristics of the sample, they are homogeneous in sex (male) and with an average age of 21 years (SD 1.27 years). In regards to weight and height, we found greater dispersion, in which the average weight is 71.5 kg (SD 7.23 kg) and the average height is 175 cm (SD 5.39 cm).
When making the normality estimate of the data from each study group for the number of jumps variable using the Shapiro-Wilk statistical test, it can be seen that the data from some of the groups that were examined in the variable were significant (p <0.05), demonstrating that they had a normal distribution.
In the power variable obtained in the 30-second continuous jump test, it is observed that the χ2 test was significant (p <0.05), indicating that the groups can be distinguished from each other and that two distinct groups are formed. One that contains all the median values of the control group while the following groups are formed by the medium of the other times studied in the study groups which are lower than those in the control group. The previously obtained results can be explained by the existing relationship in the power formula, which expresses the proportionality between the number of jumps and contact time with the power, generating that a decrease in the contact time on the diving platform will allow for an increase in the number of jumps and hence an increase in the power of the control group.
For the performance percentage variable, it can be seen that the χ2 test was not significant (p> 0.05), indicating that the medians of the groups did not differ from each other. These results remain unchanged because this variable is directly related to the squat jump and the average jump height. The latter evidence, after analysis, does not indicate significant changes throughout the evaluation, maintaining the performance percentage in a stable way.
The statistical program SPSS 15.0 and Minitab 16.0 were used for data analysis.
Results
Average Height in 30-Second Continuous Jump Test
When estimating the data normality results in each group that was studied in the average height variable, it can be seen that the data of one of the groups examined in this variable was significant (p <0.05), which is sufficient evidence to compare the results of the medium between the groups in the average height variable. The results show no statistically significant differences between groups (Figure 1).
Figure 1. Shows the average height achieved in the 30-second continuous jump test by the control groups (4 graphs on the left) and the experimental groups (4 graphs on the right). It can be seen how the median (middle line of the box plots) remains stable in the subsequent evaluations of the control group. The decrease observed in the experimental group was not statistically significant
Download figure
AHCG Average Height of Control Group Jumps (day 1-4). APGC Average Height of Experimental Group Jumps (day 1-4).
Performance Percentage in the 30-Second Continuous Jump Test in Relation to the Squat Jump
This test is performed to normalize the data of the number of jumps and the height of these, making an estimate of what percentage of the height reached during the continuous jumps corresponds to the maximum height achieved in a squat jump. When analyzing the normality of the data from the Percentage Yield data it can be seen that the data from one of the tested groups was significant (p <0.05), thus demonstrating that the sample did not have normal distributed. Figure 2 shows the results of this variable, where there are significant differences between both groups. (Figure 2).
PRGC Performance percentage of Control Group (day 1-4) PRGE Performance percentage of Experimental Group (day 1-4).
Figure 2. Shows the performance percentage relative to a squat jump achieved in the average height during the 30-second continuous jump test by the control groups (4 graphs on the left) and the experimental groups (4 graphs on the right). It can be seen that the median (middle line of the box plots) remains stable in subsequent assessments in both groups clearly demonstrating that there are no statistically significant differences.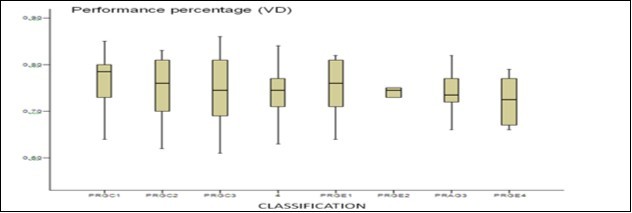
Download figure
Quantification of Delayed Onset Muscle Soreness (DOMS) by Visual Analog Scale
Figure 3 shows the median values of the control group and the study group, which are lower than those in the control group. As the evaluation days passed, a decrease in measurement values using the VAS scale can be observed for both groups. However, this is statistically significant for the experimental group Figure 3.
Figure 3. Shows the value measured using the visual analog scale for the pain variable for the control groups (4 graphs on the left) and the experimental groups (4 graphs on the right). It can be seen that the median (middle line of the box plots) increases in both groups on the second day of assessment and then begins to fall gradually in subsequent evaluations. When analyzing this data, there are statistically significant differences between the evaluated groups in favor of the experimental group.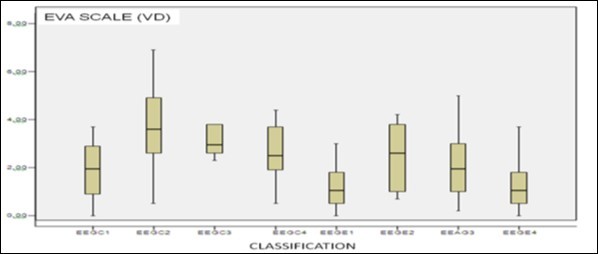
Download figure
ESCG EVA Scale Control Group (Day 1-4) ESEG EVA Scale Experimental Group (Day 1-4).
In the VAS variable, it was found that the χ2 test was significant (p <0.05), indicating that the groups can be distinguished from each other. One group contains all the median values of the control group while the following groups are formed by the medium of the other times studied in the study group, which are lower than those in the control group. The values of this scale decrease in the control group, but this characteristic is more pronounced in the study group.
By plotting the pain variable during the research, a curve can be observed, which starts with an increase, then continues on to form a plateau and then proceeds to decrease. This could be due to the varied physiological effects of Cryotherapy such as a decrease in tissue temperature, decrease in cell metabolism, a decrease of the nerve conduction velocity, delay in the formation of edema, reduction of hypoxic injury secondary to the noxa, decrease in pain, and muscle spasm14, as well as psychological factors.
Discussion
The present research was aimed at evaluation baths in ice water as an additional recovery method to the standard recovery practices planned by the technical team, after strenuous exercise by a University male soccer team. In order to achieve this, differences were evaluated between the control group (traditional training plan) and the experimental group (traditional training plan in addition to Cryotherapy), considering the following variables: performance obtained in the 30 second continuous jump test (number of jumps, average height of jumps, performance percentage in relation to a squat jump, power), and late-onset muscle soreness (DOMS) assessed by using the visual analog scale (VAS). The literature lacks the background that correctly relates variables such as performance parameters, types of exercises and intensity of the same, water temperature, immersion depth and duration, recovery time and the consequential effects on the performance of the athlete. This research considers all these variables and therefore the discussion is framed within this context.
The study data was obtained through the application of a 30-second continuous jump test on the jump pad (Axon Jump three cells) and the delayed onset muscle soreness (DOMS) was measured using the visual analog scale ( VAS).
The data obtained were as follows: a number of jumps, average jump height, performance percentage in the 30-second continuous jump test in relation to the squat jump, the power extrapolated from the continuous jump test data, and VAS pain.
The sample was homogeneous in terms of gender and age but not so for weight and height. When analyzing the initial level of the sample in terms of jump test performance, no significant differences were observed in the research variables for the study groups.
It was found that for this study there is no correlation between an increase in the number of jumps during the 30-second continuous jump test and the application of Cryotherapy through the use of ice water as a recovery method.
The reasons for the improvements in the number of jumps in the control group could be due to the adaptation of the test, generating improvements in inter-and intramuscular coordination, favoring a decrease in the contact time of each jump, a variable that was not analyzed in this study and therefore it is recommended that it be monitored in future research.
In the average height variable in the 30-second continuous jump test, it can be seen that the χ2 test was not significant (p> 0.05), indicating that all groups behaved relatively equally throughout the entire evaluation process.
The vertical jump is determined by a complex interaction of several factors including, among others, maximum strength, the speed that said strength can develop the height of the subject's legs and movement coordination2. From the aforementioned, it is understood that the strength corresponds to one of the main components that influence the height of the vertical jump, a capacity that does not express improvement before a period of 8 weeks23 and which were not able to be observed within the intervention period of two weeks. Due to what has been previously described, the improvements related to the average height variable cannot be attributed to the intervention with Cryotherapy. Despite the many variables that are controlled in this research, there are many factors involved, even with the population used in research, mostly from students majoring in physical education and kinesiology careers, which have a strenuous physical load forming part of their curriculum.
There are a number of factors controlled during the investigation as suggestions such as a decrease in workload after applying active recovery in the control group and post Cryotherapy in the experimental group. It is also indicated to the experimental group the prohibition of taking hot showers four hours after training, the time period associated with the physiological effects of ice8.
One author21, who investigated through a series of test (acceleration test at 20 meters, agility test, and vertical jump test), the effects of recovery using cold baths in a basketball tournament, concluded that all players showed a decrease in performance, except for those participating in the cold water bath. In contrast to our study, there are no significant improvements in the performance variables in the continuous jump test This also coincides with other results, who carried out baths after each game during a simulated soccer tournament that lasted for four days, and determined that cold baths do not influence CMJ performance (using physiological markers, repeated sprints, creatine kinase, and lactic dehydrogenase).
All subjects belonging to the experimental group reported improvements in lower limb pain immediately after immersion in ice water, an un-quantified situation which does not necessarily correlate with a decrease in DOMS but with a reduction in the onset of acute pain.
The results obtained in our research, when analyzed, show no significant differences in performance on the test platform for the 30 second continuous jump test for both groups, and therefore further research is suggested for the future, particularly in the DOMS variable for the experimental group which correlates with the Roswell study, who performed baths at 50 °F and 93 °F after each game during a simulated soccer tournament that lasted four days. Athletes have shown no differences in their physical tests, but the group of players that were subjected to the ice water baths reported feeling less discomfort in their legs and less fatigue overall. The similar conclusion of a study conducted on cyclists by Halson15, which found that cold water baths showed no difference in physiological markers of fatigue compared with participants who were not immersed. However, as in the Roswell study, athletes reported feeling fewer aches and pains, as well as a decrease of general fatigue.
The limitations that arise from the study are uncontrolled factors that may influence athletic performance and recovery from physical activity, such as the sports backgrounds of participants, nutrition and hydration during and after training, hours of sleep, psychological and social recovery, environmental conditions and workloads.
It is proposed as a future line of research, studies that relate Cryotherapy with athletic performance, DOMS and physiological markers of muscle damage post exercise. Furthermore, it is essential to increase the evaluation period in which changes can be quantified in the athlete's performance.
The research is relevant in proposing an intervention protocol with Cryotherapy for future studies, since, great diversity exists in the method that this therapy is applied in different studies and thus, the results on the topic, that use different methods for applying the bath immersion (immersion time, number of immersions, water temperature, etc..), hindering the realization of a therapeutic protocol.
Conclusions
In assessing the effectiveness of Cryotherapy in ice water bath modality as an additional method to a more aggressive recovery in addition to elongation, it is evident that there is no significant difference in performance on the jumping platform evaluated in the 30 second continuous jump test for the control group and experimental group in the variables of average height and performance percentage. However, there is a significant difference in the number and power of jumps variables s in the control group.
There is a significant difference in the valuation of the DOMS perception quantified by VAS between the intervention groups in the last assessment, with the quantification being less than in the experimental group, determining the effectiveness of the method of active recovery, stretching as well as Cryotherapy for this variable.
The hypothesis H1 is rejected in part, without significant improvements being found in performance, but in the DOMS.
Regarding the proposed protocol, it can be concluded that it is effective in reducing DOMS, but it is difficult to determine the effectiveness of this, in the short term performance evaluation.
Ice water baths favor performance in some of the 30-second continuous jump test modalities, also decreasing the perception of fatigue and leg pain. In turn, this may lead them to be considered a valid alternative for the management of these athletes.
References
- 1.Acevedo.Hincapie y Sánchez 2008. Valoración de la manifestación reactiva de la fuerza de los miembros inferiores a las integrantes de la selección Antioquia de voleibol categoría junior rama femenina.2008UniversidaddeAntioquiaMedellín.
- 2.Arangeo F.Efectos sobre la capacidad de saltos en futbolistas a través de un programa con máquinas de musculación en esta etapa de competencia.http://www.efdeportes.com/efd131/capacidad-de-salto-en-futbolistas-de-elite.htm.2009efdeportes,com.
- 3.Barbero J C, Andrín G, Sirotic A C.Estrategias de recuperación post partido en deportes de equipo.http://g-se.com/es/entrenamiento-en-deportes-de-equipo/articulos/estrategias-de-recuperacion-post-partido-en-deportes-de-equipo-909.
- 4.Calleja J, Granados C, Terrados N. (2009) Recuperación en balón mano de alto nivel. Revista de Ciencias del Deporte 5(1), 45-54.
- 5.Chesterton L, Foster N, Ross L. (2002) Skin temperature response to cryotherapy. PMID.11932859. Arch Phys Med.
- 6.Darryl Cochrane. (2004) Alternating hot and cold water immersion for athlete recovery: a review. New Zeland, Elsevier, physical therapy in sports
- 7.Connolly–Stephen, Sayers. (2003) Treatment and prevention of delayed onset muscle soreness. , J. Strength Cond. PMID. 12580677 Res 17(1), 197-208.
- 8.Díaz V. (2009) Metodología de la Investigación Científica y Bioestadística para profesionales y estudiantes de. Ciencias de la Salud. 2009, RIL editores. Santiago. Chile.EnDiaz,Calzadilla Lahipótesisylainvestigacióncientíficaenlasciencia médicasybiológicas.SaludUninorte.Barranquilla (Col.) 25(2), 362-373.
- 10.Gutiérrez Espinoza HJ, Lavado Bustamante IP.Méndez Pérez SJ. Revisión sistemática sobre el efecto analgésico de la crioterapia en el manejo del dolor de origen músculo esquelético.
- 11.Halson S L, Quod M J, Martin D T. (2008) Physiological responses to cold water immersion following cycling in the heat. , Int J Sports Physiol Perform; 27(6), 565-73.
- 12.Kennet J, Hardaker N, Hobbs S. (2007) Cooling Efficiency of 4 Common Cryotherapeutic Agents. , Journal of Athletic Training; 42(3), 343-348.
- 13.Kuligowski–Lephart, Giannantonio. (1998) Effect of Whirlpool Therapy on the Signs and Symptoms of Delayed-Onset Muscle Soreness. PMID: 16558514. , Journal of Athletic training; 33(3), 222-228.
- 14.Lekue J, Calleja J, Lejarreta M. (2000) Propuesta de metodología de recuperación en baloncesto de alto nivel. Revista de la asociación española de médicos del baloncesto;. 1(4), 23-28.
- 17.Montgomery P G, Pyne D B, Hopkins W G. (2009) The effect of recovery strategies on physical performance and cumulative fatigue in competitive basketball. , Journal of Sports Science; 26(11), 1135-45.
- 19.Orquín F, Torres-Luque G, F Ponce de León. (2009) Efectos de un programa de entrenamiento de fuerza sobre la composición corporal y la fuerza máxima en jóvenes entrenados. , Apunts Med Esport 164, 156-62.
- 20.Rodríguez C. (2006) Guías clínicas de la sociedad española del dolor: Valoración y manejo del dolor. España: ARÁNhttp://www.efisioterapia.net/libros/valoracion-y-manejo-del-dolor-guias-clinicas-de-la-sociedad-espanola-del-dolor
- 21.Rowsell G J, Coutts A J, Reaburn P. (2009) Effects of cold-water immersion on physical performance between successive matches in high-performance junior male soccer players. , Journal of Sports Science.PMID: 27(6), 565-73.
- 22.Sandoval M, Herrera Villabona E, Camargo Lemos D. (2007) . Efectos fisiológicos de la crioterapia. Salud UIS;39: 62-73.