
What is the Level of Empathy in Medical Students of University of Ghana Medical School in Accra Ghana?
Abstract
Empathy has been described as a multi-dimensional construct with cognitive and emotional components, both of which are concerned about responsivity to others. It has been touted as a skill essential for medical practice and thus useful to all healthcare professionals. It has been assessed in several countries and among several healthcare cadres however, there is a yawning gap in Ghana about its level in medical students. This study utilised a cross-sectional design to assess empathy using the Multi-Dimensional Emotional Empathy Scale in medical students of the University in Ghana. The scale has an alpha reliability of 0.88. One hundred and eleven students, aged 24 years ±1.5 years completed the study. Overall, there were more males than females. The mean empathy score for the cohort was 101SD 13 and this was adjudged to be low. There was no statistical difference between age, gender and clinical year and empathy in this cohort. The authors recommend that empathy, especially its cognitive aspects, should be taught in medical school curriculum of the University of Ghana Medical School, Accra.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anandakumar Haldorai, Sri Eshwar College of Engineering, Coimbatore, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Henry Lawson
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Henry Lawson —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Empathy appears to have its origin in the German word ‘Einfulung’ which literally means ‘feeling within’. The term ‘empathy’ may also have been coined from two Greek roots, ‘em’ and ‘pathos’ (feeling into).1 Although difficult to define, empathy is regarded as an attempt to understand the patient’s perspective, thereby improving interaction and building trust.2 Empathy improves patient satisfaction and compliance with treatment, reduces lawsuits, and improves competency of doctors when consulting, that is, their ability to make accurate diagnoses and efficiently utilize resources.3 Empathy is a multidimensional construct comprising an affective/emotional ability to be sensitive to and concerned for another person on one hand; and a cognitive capacity to grasp and appreciate the perspective of another person on the other.4 Mercer and Reynolds have defined Clinical Empathy as ‘the ability to understand the patient’s situation, perspective and feelings, and to communicate that understanding to the patient’.1
It is generally accepted that the cognitive portion of empathy is amenable to training hence many medical schools are adjusting their curricula to accommodate methods of enhancing empathy in their undergraduate students.5
There have been several publications on various aspects of empathy in medical students and its relation to sociodemographic variables birth order, gender, age etc. and whether it decreases or increases as one stays longer in a medical school. 3, 4, 6, 7 Apart from patient benefits, medical students and doctors also benefit from exhibiting and practicing empathy skills. Empathy has been linked to ability to pass the OSCE examination. 2, 8
Empathy was assessed for the first time in medical students in 1977 in Australia. Until 2012, empathy had not been assessed in medical students in Africa. Literature confirms that the first published paper on empathy in medical students in Africa was conducted in Jimma University Medical School Ethiopia.6 Subsequently, it has been studied across the continent. In Ghana, as far as the authors are aware, there is no publication on this subject in the state-owned, premier medical school of the country. The country has a total of seven medical schools – five (5) state-owned and two (2) private. We therefore set out to assess empathy in medical students of the University of Ghana Medical School.
Methods
A cross-sectional study was conducted on the campus of the University in Ghana. The Medical School is one of the six schools under the College of Health Sciences of the University in Ghana. The school runs two programmes - a traditional six-year course and a new four-year graduate entry medical programme (GEMP). The traditional programme attracts students qualifying from the senior high school system after 12 years of education whilst the GEMP program enrols students after their first degree in the sciences (16 years of education). Both programmes are divided into the pre-clinical and clinical programmes. The clinical programme is further divided into the first, second and third/final clinical years. The UGMS also runs a similar six-year and four-year programme for dentistry students. Medical and dentistry students in the clinical programme were targeted for this study. The current enrolment of the medical school stands at 583 for clinical year students as at the beginning of the 2014/2015 academic year. Clinical year students who had repeated any year in the previous five years were excluded from the study. We selected the Multi-Dimensional Emotional Empathy Scale was devised by Caruso and Mayer to assess empathy.9 It has 30 statements covering the following factor scales: Empathic Suffering, Positive Sharing, Responsive Crying, Emotional Attention, Feeling for Others, and Emotional Contagion. This is a 5-point Likert rating ranging from 1 to 5 with 6 reverse-scored items (scoring from 5–1).
The alpha reliability (internal consistency) for the total 30-item scale scores is 0.88 (M=3.63, SD=0.57). 10, 11
For differences in the distributions of proportions, Chi-square tests were carried out. For the mean differences, t-tests and Analysis of Variance (ANOVA) were used where assumptions underlying them were met, otherwise their non-parametric equivalents of Wilcoxon Rank Sum and Kruskal-Wallis tests respectively were used. Where appropriate, tests were carried out to investigate significant differences as such. Cutoff points for significance levels were 5% (p<0.05), 1% (p<0.01) and 0.1% (p<0.001). For findings that were not significant, exact p-values are quoted.
Results
A total of 224 medical students were recruited however 111 completed and returned the questionnaire giving a response rate of 49.6%. (Table 1)
Table 1. Background characteristics of respondents| Clinical Year | Males | Females | N (%) | Mean Age (SD) |
| 1st Clinical | 22 | 15 | 37 (33.3) | 23.38 (1.62) |
| 2nd Clinical | 17 | 14 | 31 (27.9) | 23.81 (1.25) |
| 3rd Clinical | 18 | 25 | 43 (38.8) | 24.81 (1.35) |
| Total | 57 | 54 | 111 (100) | 24.05 (1.54) |
Average age was 24 years ±1.5 years. Overall, there were more males than females and the largest group of respondents came from those in the 3rd clinical year. (Table 1) The gender distribution across the year groups is also shown below. There were more male than female respondents in all year groups except 3rd year. (Figure 1)
Figure 1. Gender Characteristics of Respondents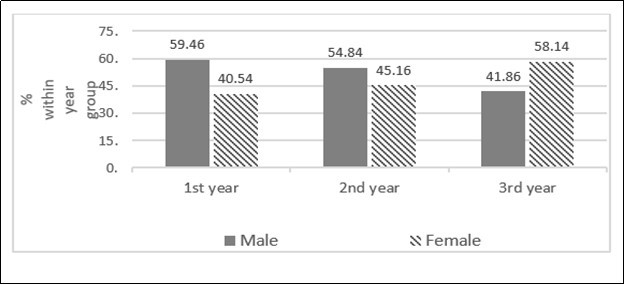
Download figure
The mean empathy score for this cohort was 101.7 (SD 13.0). The mean MDEE scores was higher for females however this difference was not statistically significant (p=0.556). Similarly, even though the second clinical year group had the highest mean MDEE score, and first clinical year group had the lowest, there was no statistically significant difference between the three year groups (p=0.375).
Discussion
Empathy and Gender
The current study found no significant difference in the empathic response of the medical students gender-wise (Table 2). The result of the study therefore goes against the well-established findings of previous studies where the women had significantly higher empathic response than the men (25-30)
Table 2. Influence of gender and level of clinical experience on multi-dimensional emotional empathy (min-max range: 30-150)| Characteristic | N | Mean (SD) of Empathy | p-value |
| Gender | |||
| Male | 57 | 100.7 (12.6) | 0.556 |
| Female | 54 | 102.0 (11.8) | |
| Clinical experience | |||
| 1st year | 37 | 101.9 (12.0) | |
| 2nd year | 31 | 103.3 (12.0) | 0.375 |
| 3rd year | 43 | 99.4 (12.5) | |
| Total | 111 | 101.3 (12.2) |
The results therefore imply that both male and female medical students will not be able to effectively appreciate the plight of their clients during clinical practice. This may therefore be reflected in the handling of the patients during management.(31)
Empathy and Clinical Years
According to Rosenfield and Jones, medical students develop maladaptive responses to cope with the demanding nature of the medical training which decreases the empathetic response of the students.(32) The findings of the current study may be an evidence to that fact because the final year medical students scored the least in terms of empathetic response (Table 2). However, the differences between the various classes were not statistically significant to solidify the evidence. Moreover, there was no significant difference between the first clinical and the final year medical students.
Again, the results of this study speak against the failure of the training program to successfully teach and embed the skill of empathy into the students’ actual experience with the patients thereby leading to the deterioration of the skill. (33, 34)
Empathy and Age
The relationship between the age and the empathic response was negative and a weak one at that (r = -0.13). The result of the study therefore implies that the older the medical student the less empathetic he or she is. Smith et al looked at ‘The complexity of empathy during medical school training: Evidence for positive changes’. They concluded that age did not have a significant effect on initial empathy scores, but did have a significant effect on rate of change, with older students demonstrating a less steep slope of change (p < 0.0).12 However, the relationship obtained in this study, unlike findings obtained in Shiraz Medical School in South Iran, was not statistically significant as the 2-tailed significance (0.894) obtained was more than the p-value of 0.05 (Table 3).
Table 3. Summary of Relationship between Empathy and Clinical year/Age| Variable | Males | Females | F (ANOVA) | Sig (2-tailed) | ||||
| Mean | SD | Std Error | Mean | SD | Std Error | |||
| Empathy | 101.7 | 13.00 | 1.74 | 102.79 | 14.18 | 1.97 | - | 0.43 |
| 1st Clinical | 101.3 | 2.04 | 0.36 | 0.70 | ||||
| 2nd Clinical | 103.46 | 2.21 | ||||||
| 3rd Clinical | 100.70 | 2.39 | ||||||
| Mean | SD | Max | Min | Pearson (r) | Sig (2-tailed) | |||
| Age | 24.05 | 1.54 | 21 | 29 | -0.13 | 0.89 | ||
| Empathy | 70 | 163 | ||||||
The result of the study nonetheless agrees with the findings of Costa et al where there was no significant relationship between the ages and the empathic response of medical students from 33 different medical schools in Portugal. 7, 13 It was then concluded that there were more important variables beyond gender and age and university to explain the empathy of medical students. The same can therefore be said concerning this study. Similarly the study findings are also consistent with those obtained in the nationwide survey of 14,070 medical students in Korea as no significant correlation was found between age and empathic response was obtained.(30) Our results also tally with that obtained by Chen et al as it was also found that age did not affect the empathic scores of the students.(25)
It can also be deduced that age does not place any medical student at a disadvantage when empathy is being considered. Every medical student is therefore placed on an equal platform to be taught and trained to develop the skill of empathy.
Study Limitations
A longitudinal study would have been a more sensitive indicator of the demographic factors that affect empathy. This study was limited by the fact that only the students in the clinical years were involved leaving out those in the preclinical years as the latter students were on vacation. The inclusion of the preclinical students would have enabled the study to fully examine the entire progression of empathy on the much wider spectrum of the medical training.
A lot of students could not be sample due to the fact that the study due to limitations places on them by their peculiar academic calendars. The lengthy nature of the questionnaires was not well received by students as a lot of them opted out of the study upon glancing through the questionnaire. Empathy is a relatively new subject in psychology therefore there was no local literature to help compare this study to.
Conclusion
The mean score for empathy in this cohort was low. Empathy was also not significantly related to age and clinical year however was higher in females than males. It is therefore the recommendation of the authors that the medical institutions must revise their curricula to provide empathetic skills to medical students which will enable them to understand themselves, relate well with their colleagues, cope with the stresses of the profession and empathize with their patient. This will enhance the doctor’s ability to provide a holistic patient-centred care.
References
- 1.Mercer S W, Reynolds W J. (2002) Empathy and quality of care. Br J Gen Pract [Internet]. Oct;52 Suppl(Suppl):S9–12. Available from: https://pubmed.ncbi.nlm.nih.gov/12389763 .
- 2.Light A, Gupta T, Burrows A, Nandakumar M, Daniel A et al. (2019) Learning empathy: the medical student perspective. Clin Teach. 16(1), 76-7.
- 3.Papageorgiou A, Miles S, Fromage M. (2018) Does medical students’ empathy change during their 5-year MBBS degree? Educ Health (Abingdon). 31(3), 142-7.
- 4.Quince T A, Parker R A, Wood D F, Benson J A. (2011) Stability of empathy among undergraduate medical students: a longitudinal study at one UK medical school. BMC Med Educ. Oct;11: 90.
- 5.Patel S, Pelletier-Bui A, Smith S, Roberts M B, Kilgannon H et al. (2019) Curricula for empathy and compassion training in medical education:A systematic review.PLoS One. 14(8), 0221412.
- 6.Dehning S, Girma E, Gasperi S, Meyer S, Tesfaye M et al. (2012) Comparative cross-sectional study of empathy among first year and final year medical students in Jimma University, Ethiopia: steady state of the heart and opening of the eyes. BMC Med Educ. May;12: 34.
- 7.Magalhães E, Salgueira A P, Costa P, Costa M J. (2011) Empathy in senior year and first year medical students: a cross-sectional study. BMC Med Educ. Jul;11: 52.
- 8.Casas R S, Xuan Z, Jackson A H, Stanfield L E, Harvey N C et al. (2017) Associations of medical student empathy with clinical competence. Patient Educ Couns. 100(4), 742-7.
- 9.Caruso D R, Mayer John D. (1998) A Measure of Emotional Empathy for Adolescents and Adults. Available from: https://scholars.unh.edu/cgi/viewcontent.cgi?article=1021&context=personality_lab
- 10.Faye A, Kalra G, Swamy R, Shukla A, Subramanyam A et al. (2011) Study of emotional intelligence and empathy in medical postgraduates. , Indian 53(2), 140-4.
- 11.Alloway T P, Copello E, Loesch M, Soares C, Watkins J et al. (2016) Investigating the reliability and validity of the Multidimensional Emotional Empathy Scale. Measurement [Internet]. Available from: sci-hub.tw/10.1016/j.measurement.2016.05.014 90, 438-42.