
Neck, Shoulder and Low Back Musculoskeletal Pain in Greek Physical Education University Students: A Series of Three Cross-Sectional Studies
Abstract
Several studies examine the musculoskeletal pain (MSP) in university students sustaining physical load as part of their compulsory learning. However, only two somewhat outdated cross-sectional studies examine the physical education teacher (PET) students. This study aimed to explore the neck, shoulder and low back MSP prevalence in Greek PET students in a series of academic years. The Nordic Musculoskeletal Questionnaire was used to record the past 12-month neck, shoulder and, low back pain, across three academic years (n = 479). The year association to MSP prevalence was examined with the cross-tabulation analysis (using the column proportion test for the year comparison) and, the gender association to MSP prevalence with the χ2 test (SPSS 22.0, p ≤ 0.05). The year association to MSP prevalence was not significant (p > 0.05). The overall prevalence was 67.6%, with multiple pain at 25.7% and, the low back presenting the highest prevalence (40.9%). Women reported a higher prevalence of neck (36%) and low back (47%) pain (p ≤ 0.05). The majority of pain and time loss duration was 1-7 days. The low back required higher medical attention (19.0%) than the neck (9.2%) and the shoulder (12.9%). The recurrent pain was at 30%, with the previous injury/accident rate at 5.8%, 14.4% and 14.6% for the neck, shoulder and low back. Our PET students present an alarming MSP prevalence. Due to their distinct work demands as PE teachers, entering working life with the healthiest possible musculoskeletal system is of critical importance. Thus, university authorities should consider strategies for the prevention of MSP risk.
Article Information
- Received
- Accepted
- Published
Academic Editor: Subita Patil, Assistant Professor, Department of Community Medicine, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Analina A. Emmanouil, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Elissavet Rousanoglou, Sports Biomechanics Lab, Section of Sport Medicine & Biology of Exercise, School of Physical Education & Sport Science, National &, Kapodistrian, University of Athens, Greece —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Musculoskeletal pain (MSP) is a highly prevalent and disabling condition that affects people of all ages, gender and socio-demographic characteristics, with subsequent increased health care utilization 1, 2. In spite of the different social and cultural substrate of the studied populations, the MSP prevalence in the general population rises approximately to 30% (range 13.5–47%) 1. Epidemiological surveys document a worrying MSP prevalence in young populations and underline the need for early prevention and detection 3. The MSP development in university students is of particular interest as it may affect their daily life 4 and academic success 5. The MSP may also have a significant impact on their future musculoskeletal health 6. Pain tends to persist 7, 8 and predisposes to a higher risk of future MSP 8, 9.
In university students, the MSP is usually associated with the physical load that they must sustain to meet the demands of their learning compulsory activities 10. The studies on university students examine either a variety of disciplines 4, 11 or distinct disciplines as dental hygiene 12, medicine 13, nursing 14, physiotherapy 15 and, physical education teacher 6, 17. The physical education teacher (PET) students constitute a distinct university discipline because of the inherent injury risk associated to the physical load of the compulsory sports participation required by their study curriculum. Cross-sectional studies examined the injury prevalence in PET students a long time ago 18, with an ongoing research interest 19, 20, 21. However, to the best of our knowledge, only two outdated studies appear to examine the MSP prevalence in PET students 16, 17, indicating the lack of research during the last decade. In particular, Brennan et al. 16 reported a 30% prevalence of low back pain, using a past 12-month retrospective questionnaire to examine a single only site of pain. Fliciński 17 examined a variety of pain sites and reported an almost 50% prevalence in their PET students, who claimed as most frequent the knee, shoulder, and ankle pain. In the study of Fliciński 17, sports injuries were the most critical risk factor for MSP (42.4% and 50.5% of women and men, respectively reported a total of 1065 casualties) with participation in specific sports identified as the primary injury risk factor.
The pain prevalence in PET students is of particular interest due to the physical load and injury susceptibility associated not only to their academic but also to their future working life as Physical Education (PE) teachers 22, 23. In fact, the PE teachers claim their rather high prevalence of musculoskeletal disorders as a limiting factor of their working capacity 22, 23, 24. The prospective studies about multiple MSP in university students 7, 8, 11 conclude that the average sites of pain appear to be settled by age 20, and little variation occurs thereafter 8. Thus, PET students with multisite pain will most probably enter their working life as PE teachers already suffering from multiple MSP. However, there appear no prospective data regarding the MSP prevalence in PET students. The lack of prospective or serial cross-sectional research on MSP prevalence in PET students highlights the necessity for more and up to date studies. Such studies may contribute to MSP prevention and management during their physically demanding academic years. Thus, this study aimed to explore the prevalence of neck, shoulder and low back pain in a series of academic years in Greek PET students.
Methods
Study Design & Sample
A total of 479 students of the School of Physical Education and Sports Science of National and Kapodistrian University of Athens, Greece, participated in the study after signing an informed consent. Participants derived from three academic years (Y1: 2011-2012, Y2: 2015-2016 and Y3: 2017-2018). All students in Y1, Y2 and Y3 were eligible to participate in the study, In Y1, Y2 and Y3, respectively, the participants (n=123, n=160, and n=196) correspond to 17.6%, 22.9%, and 28.0% of the active students, and 12.3%, 16.0% and 19.6% of the officially registered students. Among the officially registered students, the percentage of active students rises to about 70%. Thus, the total of 479 students corresponds to 22.8% and 16.0%, respectively, of the active and the officially registered students. The protocol of the study was submitted to and approved by an institutional review board for testing of human subjects.
Study Instruments
The Standardized Nordic Questionnaire (SNQ) 25, which is a validated measure of musculoskeletal pain, was selected to assess MSP complaints. The questionnaire, translated into the Greek language and adapted for PET students, was pretested on forty students to ensure understandability of the questions. The responses provided in the pretest questionnaire showed a good understanding and a clear comprehension. Respondents were instructed to report whether they had experienced any pain or discomfort in 3 body regions over the past 12 months, naming the neck, shoulder and low back. The questionnaire was also supplemented by a ‘‘pain-site drawing” to illustrate the body regions of interest pictorially. The questionnaire also sought information about the sociodemographic characteristics (gender, age, body mass index, spine disorders, weekly coursework hours and daily computer use hours), as well as, general (pain prevalence and medical attention required) and specific (days of pain duration and days of time loss). Additional information regarding the time before the past 12 months was also sought (previous pain incidence and previous injury/accident regarding the reported site of pain). The same questionnaire was delivered at the beginning of the winter semester in all three academic years, with the single exception of the computer use hours that was not included in Y1 of data collection. The questionnaire was delivered during auditorium lectures regarding compulsory courses. The timetable of the auditorium lectures is usually constant across academic years for all study years, thus this sampling approach allowed us to contact a large number of students at a similar time period of the winter semester across the years of the study. Students are not obliged to present themselves in the auditorium lectures; however, it is typical that a large number of students attend these courses at the beginning of each semester. Practical constraints did not allow to deliver the questionnaire in consecutive academic years or at academic years with even Intervals between them.
Statistical Analysis
The cross-tabulation analysis was used to test the academic year association to MSP prevalence. The column proportion comparison test included in the cross-tabulation analysis was used to test the difference of MSP prevalence between academic years. This option computes pairwise comparisons of column proportions and indicates which pairs of columns (for a given row, with columns indicating the academic years) are significantly different. In the column proportions comparison, the Bonferroni correction was used to adjust the p-values for multiple comparisons. Chi-Square tests (χ2) were applied to test the gender association to pain prevalence. All statistical analyses were conducted using the SPSS statistical software version 22 (IBM Corp., Armonk, NY, USA), with the level of significance set at p ≤ 0.05.
Results
The characteristics of the 479 students (Men: 48%, Women: 52%) who completed the questionnaire along the three years are presented in Table 1. Across all three years, 67.6% of the students reported MSP symptoms, with 25.7% of them reporting more than one pain site (Table 2). The gender association to the neck and low back pain was significant (Figure 1), with women demonstrating a significantly higher pain prevalence in almost all three years (p ≤ 0.05), whereas the gender association to shoulder pain was not significant (p > 0.05). Association of the other demographics to pain (age, body mass index, coursework hours, computer use, and spine disorders) was not examined as their distribution was predominantly in a single category.
Table 1. Characteristics of the participants. Values indicate the percentage and count of the year total % (n).| Y12011-2012 | Y22015-2016 | Y32017-2018 | All Years | Year association | ||
| Total respondents | (n = 123) | (n = 160) | (n = 196) | (n = 479) | *p ≤ 0.05 | |
| % (n) | % (n) | % (n) | ||||
| Gender | Men | 45.5 (56) | 52.5 (84) | 45.9 (90) | 48.0 (230) | χ2 = 1.939 |
| Women | 54.5 (67) | 47.5 (76) | 54.1 (106) | 52.0 (249) | p = 0.379 | |
| Age (years) | 18-25 | 95.9 (118) | 91.9 (147) | 93.2 (179) | 93.7 (445) | χ2 = 1.911 |
| 26-33 | 4.1 (5) | 8.1 (13) | 6.8 (13) | 6.3 (30) | p = 0.385 | |
| Body Mass Index | < 18.5 | 4.1 (5) | 2.5 (4) | 5.6 (11) | 4.2 (20) | |
| (kg / m2) | 18.5-24.9 | 88.6 (109) | 86.9 (139) | 88.2 (172) | 87.9 (420) | χ2 = 5.578 |
| 25.0-29.9 | 7.3 (9) | 10 (16) | 6.2 (12) | 7.7 (37) | p = 0.444 | |
| < 30.0 | 0 (0) | 0.6 (1) | 0 (0) | 0.2 (1) | ||
| Spine disorder † | Normal | 77.2 (95) | 73.8 (118) | 80.0 (156) | 82.2 (393) | χ2 = 1.950 |
| Disorder | 22.8 (28) | 26.3 (42) | 20 (39) | 17.8 (85) | p = 0.381 | |
| Coursework | < 20 | 96.7 (119) | 67.5 (108) | 59.6 (109) | 72.1 (336) | χ2 = 53.133 |
| (h / week) | ≥ 20 | 3.3 (4) | 32.5 (52) | 40.4 (74) | 27.9 (130) | p = 0.000* |
| Computer use | < 10 | na | 91.3 (146) | 98.4 (186) | 95.1 (332) | χ2 = 9.593 |
| (h / day) | ≥ 10 | na | 8.8 (14) | 1.6 (3) | 4.9 (17) | p = 0.002* |
Figure 1. Gender association to pain prevalence in neck, shoulder and low back. *significant gender difference at p ≤ 0.05.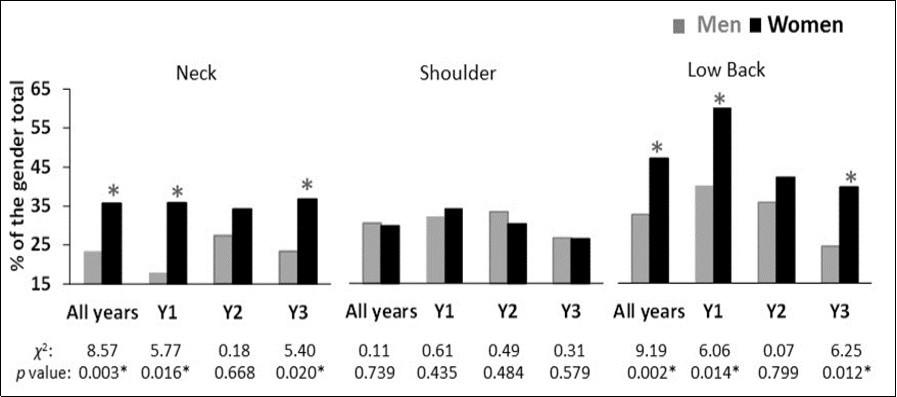
Download figure
Pain General Characteristics
Overall for gender and across all three years (Table 2), the low back was the site with the highest past 12-month prevalence followed by the shoulder and the neck. The low back pain required medical attention at a higher percentage (19.0%) than the neck (9.2%) and the shoulder (12.9%) MSP (Table 2). More than 30% of the participants reported their pain as a recurrent incidence (neck: 32.4%, shoulder: 33.6%, low back: 44.1%) (Table 2). The percentage of students with previous injury/accident at the site of pain raised to 5.8%, 14.4% and 14.6% for the neck, shoulder and low back, respectively (Table 2). About 4% of those with low back pain reported a hospitalization due to a pain incidence before the past-12 month period (Table 2). A significant year association, indicating a decreasing trend, was found for the low back past 12-month and recurrent pain (p ≤ 0.05) (Table 2). A significant year association, indicating a decreasing trend, was found for the shoulder previous injury/accident (p ≤ 0.05) (Table 2). In specific, Y3 demonstrated a significantly lower prevalence (p ≤ 0.05) of low back past 12-month and recurrent pain, as well as, of shoulder previous injury/accident.
Table 2. MSP prevalence and pain characteristics in the three years (Y1, Y2, Y3). Values indicate the percentage and count of the year total % (n) for the “YES” responses in each category.| Y12011-2012 | Y22015-2016 | Y32017-2018 | All Years | Year association | ||
| Total respondents | (n = 123) | (n = 160) | (n = 196) | (n = 479) | * p ≤ 0.05 | |
| % (n) | % (n) | % (n) | % (n) | |||
| Number of pain sites | ||||||
| No pain | 24.4 (30) | 31.3 (50) | 38.3 (75) | 32.4 (155) | ||
| 1 site | 42.7 (58) | 41.3 (66) | 39.3 (77) | 42.0 (201) | χ2 = 11.122 | |
| 2 sites | 17.9 (22) | 22.5 (36) | 16.8 (33) | 19.0 (91) | p = 0.085 | |
| 3 sites | 10.6 (13) | 5.0 (8) | 5.6 (11) | 6.7 (32) | ||
| Past 12-month pain | ||||||
| Neck | 48.0 (59) | 30.6 (49) | 30.6 (60) | 35.1 (168) | χ2 = 0.387, p = 0.824 | |
| Shoulder | 33.3 (41) | 32.5 (52) | 31.1 (61) | 32.2 (154) | χ2 = 2.039, p = 0.361 | |
| Low back | 55.3 (68) | 40.0 (64) | 32.7 (64) | 40.9 (196) | χ2 = 14.062, p = 0.001* | |
| Medical attention | ||||||
| Neck | 8.9 (11) | 10.6 (17) | 8.2 (16) | 9.2 (44) | χ2 = 2.777, p = 0.249 | |
| Shoulder | 15.4 (19) | 12.5 (20) | 11.7 (23) | 12.9 (62) | χ2 = 0.956, p = 0.620 | |
| Low back | 25.2 (31) | 18.8 (30) | 15.3 (30) | 19.0 (91) | χ2 = 0.507, p =0.776 | |
| Recurrent pain | ||||||
| Neck | 32.5 (40) | 31.9 (51) | 32.7 (64) | 32.4 (155) | χ2 = 2.085, p = 0.353 | |
| Shoulder | 35.8 (44) | 33.8 (54) | 32.1 (63) | 33.6 (161) | χ2 = 3.417, p = 0.181 | |
| Low back | 59.3 (73) | 40 (64) | 37.8 (74) | 44.1 (211) | χ2 = 23.067, p = 0.000* | |
| Previous Injury/Accident | ||||||
| Neck | 6.5 (8) | 5.6 (9) | 5.6 (11) | 5.8 (28) | χ2 = 0.232, p = 0.891 | |
| Shoulder | 22.8 (28) | 13.8 (22) | 9.7 (19) | 14.4 (69) | χ2 = 8.997, p = 0.011* | |
| † Low back | 21.1 (26) | 13.8 (22) | 11.2 (22) | 14.6 (70) | χ2 = 0.389, p = 0.823 | |
Pain and Time Loss Duration
The majority of the pain symptoms lasted from 1 - 7 days (neck: 73.8%, shoulder: 49.4%, low back: 57.7%), except the similar shoulder pain duration in Y2 for both 1-7 days (36.5%) and 8-30 days (34.6%) (Table 3). The year association to pain duration was significant for all three pain sites (p ≤ 0.05), with significant year differences indicating a pain site and pain duration specificity (Table 3). For the neck, in Y3 there was an increase of pain lasting 1-7 days with a concomitant decrease of pain lasting >30 days but not every day, both significantly different from Y2, p ≤ 0.05. Regarding the shoulder, in Y3 there was also an increase of pain lasting 1-7 days but with a concomitant decrease of pain lasting 8-30 days, both significantly different from Y1 (p ≤ 0.05). In Y3 compared to Y2, there was a significant decrease (p ≤ 0.05) of the low back pain lasting for more than 30 days but not every day. Course time loss raised to 37.5%, 66.9% and 57.1% for the neck, shoulder and low back respectively (Table 3) with the majority of time loss lasting from 1 - 7 days (Table 3). The year association to time loss duration was significant only for the low back pain, with the year comparison indicating a decrease of the overall time loss in Y3 than Y1 and Y2 (Table 3).
Table 3. Pain and time loss duration across the three years (Y1, Y2, Y3) % (n).| Y1 | Y2 | Y3 | All Years | Year association *p ≤ 0.05 | |
| 2011-2012 | 2015-2016 | 2017-2018 | |||
| (n = 59) | (n = 49) | (n = 60) | (n = 168) | ||
| % (n) | % (n) | % (n) | % (n) | ||
| Pain duration | |||||
| Neck | |||||
| 1-7 daysPD | 76.3 (45) | 57.1 (28) | 85.0 (51) | 73.8 (124) | |
| 8-30 days | 11.9 (7) | 12.2 (6) | 11.7 (7) | 11.9 (20) | χ2 = 25.870 |
| >30 days - not every day | 10.2 (6) | 24.5 (12) | 3.3 (2) | 11.9 (20) | p = 0.000* |
| Every dayPD | 1.7 (1) | 6.1 (3) | 0 (0) | 2.4 (4) | |
| Shoulder | |||||
| 1-7 daysPD | 41.5 (17) | 36.5 (19) | 65.6 (40) | 49.4 (76) | |
| 8-30 days | 22.0 (9) | 34.6 (18) | 23.0 (14) | 26.6 (41) | χ2 =15.245 |
| >30 days - not every dayPD | 24.4 (10) | 21.2 (11) | 6.6 (4) | 16.2 (25) | p = 0.015* |
| Every day | 12.2 (5) | 7.7 (4) | 4.9 (3) | 7.8 (12) | |
| Low Back | |||||
| 1-7 days | 64.7 (44) | 43.8 (28) | 64.1 (41) | 57.7 (113) | |
| 8-30 days | 11.8 (8) | 17.2 (11) | 15.6 (10) | 14.8 (29) | χ2 = 16.574 |
| >30 days - not every dayPD | 14.7 (10) | 32.8 (21) | 14.1 (9) | 20.4 (40) | p = 0.031* |
| Every day | 8.8 (6) | 6.3 (4) | 6.3 (4) | 7.1 (14) | |
| Time loss duration | |||||
| Neck | |||||
| 0 days | 69.5 (41) | 65.3 (32) | 53.3 (32) | 62.5 (105) | |
| 1-7 days | 23.7 (14) | 30.6 (15) | 28.3 (17) | 27.4 (46) | χ2 = 9.826 |
| 8-30 daysTLD | 6.8 (4) | 4.1 (2) | 0 (0) | 3.6 (6) | p = 0.073 |
| >30 days | 0 (0) | 0 (0) | 18.3 (11) | 6.5 (11) | |
| Shoulder | |||||
| 0 days | 58.5 (24) | 59.6 (31) | 78.7 (48) | 66.9 (103) | |
| 1-7 days | 31.7 (13) | 28.8 (15) | 14.8 (9) | 24.0 (37) | χ2 = 8.397 |
| 8-30 days | 9.8 (4) | 9.6 (5) | 4.9 (3) | 7.8 (12) | p = 0.154 |
| >30 days | 0 (0) | 1.9 (1) | 1.6 (1) | 1.3 (2) | |
| Low Back | |||||
| 0 daysTLD | 50.0 (34) | 50.0 (32) | 71.9 (46) | 57.1 (112) | |
| 1-7 days | 32.4 (22) | 37.5 (24) | 23.4 (15) | 31.1 (61) | χ2 = 14.897 |
| 8-30 days | 8.8 (6) | 4.7 (3) | 3.1 (2) | 5.6 (11) | p = 0.016* |
| >30 days | 8.8 (6) | 7.8 (5) | 1.6 (1) | 6.1 (12) |
Discussion
The study aimed to examine the neck, shoulder, and low back prevalence of MSP in Greek PET students across three academic years. The 67.6% overall MSP prevalence is higher than the prevalence of 32% and 50%, respectively, reported for PET students by Brennan et al. 16 and Fliciński 17. However, it must be noted that Brennan et al. 16 examined only the low back pain. Furthermore, despite their variety of pain sites (shoulder, elbow, wrist, hand, hip, knee, ankle, and foot), Fliciński 17 did not include the neck and low back in their study. Sports injuries appear as the most critical risk factors for MSP 17 with an ongoing research interest regarding interventions that could prevent the injury incidences in PET students 19, 20, 21, 22. When compared with other disciplines, the overall pain prevalence in the present study was within the range reported in studies including the neck, the shoulder, and the low back to examine the past 12-month pain. In specific, the overall pain prevalence was 64.3% for dental students 12, 75.8-89.3% for medical students 13, 64% for nursing students 14 and, 63% for physiotherapy students 15. When a variety of disciplines was included in the same study, the MSP prevalence ranged from 34% 11 up to 92.7% 4.
In agreement with the majority of previous studies in university students 11, 13, 17 as well as in general population 1, 26 women had a higher MSP prevalence than men. The strong association of gender to MSP prevalence is broadly supported 1, 26, 27, 28. The purpose of this study was not to determine the factors of the gender related MSP differences. However, in general, the explanations for gender differences in MSP are categorized in three groups, in terms that women rather than men: (A) are more willing to report pain, (B) are more vulnerable to develop MSP because of gender-linked factors (hormones, physiology, pain sensitivity), and (C) may possibly sustain a greater accumulative exposure to MSP risk factors when one considers both the working (studying in the case of university students) and typical household-related activities (cleaning, laundry, etc.) 26, 27, 28. Some studies do not succeed in revealing any specific risk factors that could explain the higher prevalence of chronic musculoskeletal complaints in women than men 26. As concluded by Andorsen et al. 26 in their 13-year prospective study, unmeasured factors may also be contributing substantially to the MSP gender differences, which warrants further research focused on such factors.
The increasing trend of MSP highlights a documented worldwide growing health problem that appears to affect people of all ages, gender and socio-demographic characteristics 1, 2. In our study, the MSP prevalence did not reveal a significant year trend for the neck and the shoulder pain. However, it showed a decreasing year trend in the low back past 12-month pain, the recurrent pain, and the shoulder previous injury/accident. The pain and time loss duration did not show a specific year trend profile for the three pain sites, with both significantly increases and decreases in Y3 compared to the other years. The comparison to earlier data is not feasible due to the scarcity of previous serial cross-sectional or prospective studies on university students. To the best of our knowledge, the single MSP prospective study in university students is the nationwide study of Oksanen et al. 11. Oksanen et al. 11, using the previous week rather than the past 12-month symptoms, report an increasing trend of MSP from 2000 to 2012 in Finnish university students. Over a 6.5 year period, there was an increase in the number of pain sites in men but not in women young technical students entering their working life 7, indicating a gender specificity regarding the MSP risk factors. So far, a variety of psychosocial and lifestyle factors have been proposed for the increasing MSP in adolescents (sedentary activities and sleeping, physical activity level, body mass index, alcohol consumption, smoking, and emotional and behavioral factors) 29. However, the reasons for increasing MSP in young adults are not known, and there is still much uncertainty about the factors leading to pain.
In university students, the MSP is associated with the physical load that they need sustain during their compulsory learning activities 12, 13, 14, 15, 16, 17. Oksanen et al. 11 suggest that broad ergonomic information targeted to young people, together with the increase and widening of the preventive health care could lower the future MSP prevalence in university students. Ergonomic information may also regard the use of computers in university students as their daily hours of computer use are associated with musculoskeletal discomfort 10. However, in our study, the vast majority (95.1%) of PET students reported their computer use to be less than 10 hours per day, allowing us to disregard computer use as a factor for their MSP based on the data provided by Noack-Cooper et al. 10. It should not be ignored that, in university students, health complaints are also associated with perceived stress 5, 30. More specifically, Ekpenyong et al. 5 suggest to particularly consider certain factors (i.e., demographics, reaction to stress) when developing interventions for stress-induced MSP among university students.
Regardless of the reasons for their MSP development, the comparison of our PET students with previous PET students is limited to the somewhat outdated cross-sectional studies of Brennan et al. 16 and Fliciński 17 which both used a past-12 month questionnaire. Brennan et al. 16 examined only the low back pain and report a higher (40.1%) than the present (30%) pain prevalence. Fliciński 17 reported the shoulder prevalence about 30% (Men: 28%, Women: 29%) similar to the 30.1% pain prevalence of the present study; however, they did not include the neck and the low back in their study. In the survey of Fliciński 17, sports injuries were the most critical risk factors for MSP (42.4% and 50.5% of women and men, respectively reported a total of 1065 incidences) with participation in specific sports identified as the primary injury risk factor. The recurrent pain in our study is also worrying; more than one-third of the students reported their pain as a recurrent one (32.4%, 33.6% and 44.1% for the neck, shoulder, and low back, respectively). Besides the discomfort itself, pain, and particularly the recurrent one, may limit students’ daily and leisure time 4, 14 and increase the psychical stress 30. Above all, MSP symptoms may impair study success 5 and affect the students’ future musculoskeletal health 6.
The co-occurring MSP is also of particular interest. In the present study, about 36% of our PET students reported multiple pains. This percentage is almost triple than the 12.5% reported by Oksanen et al. 11 in a variety of university students regarding four pain sites (neck-shoulder, low back, limb/joint, temporomandibular). The lower prevalence of multiple pains in Oksanen et al. 11 may be attributed to the student population specificity, as PET students are exposed to a higher physical workload than general student population. However, our 36% multiple pain prevalence is lower than the multiple pain reported for Greek workers 31, young technical school students 7, and the general population 8. In specific, Solidaki et al. 31 in their cross-sectional study, report a 67% multiple pain prevalence for a total of 6 body sites (neck, shoulder, elbow, wrist-hand, low back, and knee). Hanvold et al. 7, in their 6.5-year prospective study, report the baseline multiple pain at 69% for a total of 4 pain sites (neck-shoulder, low back, arm-hand-wrist, hip-knee-leg). Kamaleri et al. 8, in their 14-year prospective site on general population, report the baseline multiple pain at 75% for a total of 10 pain sites (head, neck, shoulder, elbow, hand/wrist, upper back, lower back, hip, knee, and ankle/foot). The pattern of multiple pains has been found to be relatively stable over the years 7, 8, 11 as the average sites of pain appears to be settled by age 20 and little variation occurs after that 8. Furthermore, the pattern of multiple pain sites is more strongly related to work disability 32 and long-term sickness absence 33. Thus, even though the multiple pain prevalence in our Greek PET students is lower than in previous studies 7, 8, 31, it should not be overlooked; multisite pain may persist or reoccur, meaning that those students who report multisite pain will most probably continue to do so during their working life 8. Studies in European and worldwide populations suggest that it is vital to widen the preventive health care 3, 11 and to identify the factors predicting the number of pain sites already at an early age 6. Furthermore, it is essential to provide the young population of students with specific preventive and informative programs including ergonomic, physiological, and psychosocial and lifestyle aspects 4, 5, 11, 17, 21, 30.
In the perspective of the physical load and musculoskeletal disorders associated to the upcoming working life of the PET students 22, 23, 24, 34, the pain prevalence is of particular interest as it may limit their future working ability 24. All over the world, PE teachers face similar essential duties demanding a rather high physical workload 22, 23, 34. The musculoskeletal risk due to their work duties justifies the consideration whether it is possible, or even reasonable, to work as a PE teacher after the age of 60 24. Thus, it is of utmost importance to develop strategies that will allow PET students to enter their working life with the healthiest possible musculoskeletal system. Such strategies aim to prevent the risk factors associated with the study curriculum 21.
When interpreting the results of the present study, one should consider the possible bias as the data was collected through questionnaires. Self-reports may be influenced by, for example, personality dimensions such as negative affectivity (common method bias) 35. Also, self-administered questionnaires tend to be answered primarily by those who perceive the questions to be relevant 36. The population of the study does not reflect a 'general' population due to the mean age and narrow age range limited to the academic years as well as the discipline specificities of the PET population. Furthermore, the physical workload induced by the study curriculum of the Greek PET students may be different than PET students from other countries. Thus, the results from this study cannot be generalized to all PET students. As stated in our introduction, the study was conducted to explore the prevalence of MSP among the Greek PET students rather than to study the risk factors. Nevertheless, the results are alarming, and careful attention should be given by school authorities to increase students’ awareness of MSP prevention and management.
In conclusion, our series of three cross-sectional studies in Greek PET students is in agreement with previous studies among university disciplines when students must sustain a significant physical load as part of their compulsory learning activities (i.e., dental, medical, nursing, and physiotherapy students). Although an increasing trend was not revealed across the three academic years of 2011-2012, 2015-2016 and 2017-2018, the overall pain prevalence in our PET students (67.6%) could be considered somewhat high compared to the general population (30%, ranging from 13.5 to 47%) 1. The reduction of MSP during their academic life is of critical importance, as in their future working life as PE teachers, the PET students will also be susceptible to increased physical load and injury risk due to their distinct work demands. Thus entering their working life with a healthy musculoskeletal system is of critical importance and underlines the need for PE university authorities to take initiatives (i.e., changes of physical curriculum load) for the reduction of MSP.
References
- 1.Cimmino M A, Ferrone C, Cutolo M. (2011) Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 25(2), 173-183.
- 2.Woolf A D, Erwin J, March L. (2012) The need to address the burden of musculoskeletal conditions. , Best Pract Res Clin Rheumatol 26(2), 183-224.
- 3.P Van Wambeke, Morlion B. (2014) The growing burden of musculoskeletal pain and the urgent need for early prevention and detection at young age. , Eur J Pain 18(9), 1221-1222.
- 4.Tse M MY, Tang A, Budnick A, Ng S S M, Yeung S S Y. (2017) Pain and pain management among university students: Online survey and web-based education. Cyberpsycho Behav Soc Netw. 20(5), 305-313.
- 5.C E Ekpenyong, Daniel N E, Aribo E O. (2013) Associations between academic stressors, reaction to stress, coping strategies and musculoskeletal disorders among college students. , Ethiop J Health Sci 23(2), 98-112.
- 6.É P Legault, Descarreaux M, Cantin V. (2015) Musculoskeletal symptoms in an adolescent athlete population: a comparative study. , BMC Musculoskelet Disord 16(1), 210.
- 7.T N Hanvold, Lunde L K, Koch M, Wærsted M, Veiersted K B. (2016) Multisite musculoskeletal pain among young technical school students entering working life. , BMC Musculoskelet Disord 7, 82.
- 8.Kamaleri Y, Natvig B, Ihlebaek C M, Benth J S, Bruusgaard D. (2009) Change in the number of musculoskeletal pain sites: A 14-year prospective study. , Pain 141(1), 25-30.
- 9.Hanvold T N, Veiersted K B, Wærsted M. (2010) A prospective study of neck, shoulder, and upper back pain among technical school students entering working life. , J Adolesc Health 46(5), 488-494.
- 10.Noack-Cooper K L, Sommerich C M, Mirka G A. (2009) College students and computers: assessment of usage patterns and musculoskeletal discomfort. , Work 32(3), 285-298.
- 11.Oksane A M, Laimi K, Löyttyniemi E, Kunttu K. (2014) Trends of weekly musculoskeletal pain from2000to2012:National study of Finnish university students. , Eur J Pain 18(9), 1316-1322.
- 12.M J Hayes, Smith D R, Taylor J A. (2014) Musculoskeletal disorders in a 3 year longitudinal cohort of dental hygiene students. , J Dent Hyg 88(1), 36-41.
- 13.Smith D R, Leggat P A. (2007) Prevalence and distribution of musculoskeletal pain among Australian medical students. , J Musculoskelet Pain; 15(4), 39-46.
- 14.Backåberg S, Rask M, Brunt D, Gummesson C. (2014) Impact of musculoskeletal symptoms on general physical activity during nursing education. , J Nurs Educ Pract 14(4), 385-390.
- 15.Nyland L J, Grimmer K A. (2003) Is undergraduate physiotherapy study a risk factor for low back pain? A prevalence study of LBP in physiotherapy students. , BMC Musculoskelet Disord 4(1), 22.
- 16.Brennan G, Shafat A, Mac Donncha C, Vekins C. (2007) Lower back pain in physically demanding college academic programs: a questionnaire based study. , BMC Musculoskelet Disord 8, 67.
- 17.Fliciński J. (2008) Occurrence and risk factors of musculoskeletal pain and sport injuries in students of physical education inUniversityofSzczecin. , Ann Acad Med Stetin 54(3), 31-47.
- 18.Twellaar M, F T Verstappen, Huson A. (1996) Is prevention of sports injuries a realistic goal? A four-year prospective investigation of sports injuries among physical education students. , Am J Sports Med 24(4), 528-534.
- 19.Bliekendaal S, Goossens L, Stubbe J H. (2017) Incidence and risk factors of injuries and their impact on academic success: A prospective study in PETE students. , Scand J Med Sci Sports 27(12), 1978-1985.
- 20.Goossens L, Verrelst R, Cardon G.De Clercq D (2014)Sports injuries in Physical Education Teacher Education students. , Scand J Med Sci Sports 24(4), 683-691.
- 21.Goossens L, Cardon G, Witvrouw E, Steyaert A.De Clercq D (2016)A multifactorial injury prevention intervention reduces injury incidence in Physical Education Teacher Education students. , Eur J Sport Sci 16(3), 365-373.
- 22.Pihl E, Matsin T, Jurimae T. (2002) Physical activity, musculoskeletal disorders and cardiovascular risk factors in male physical education teachers. , J Sports Med Phys Fitness 42(4), 466-471.
- 23.Sandmark H. (2000) Musculoskeletal dysfunction in physical education teachers. , Occup Environ Med 57(10), 673-677.
- 24.Mäkelä K, Hirvensalo M. (2015) Work Ability of Finnish Physical Education Teachers. The Physical Educator. 72, 384-398.
- 25.Kuorinka I, Jonsson B, Kilbom A, Vinterber H, Biering-Sørensen F. (1987) Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. , Appl Ergon 18(3), 233-237.
- 26.O F Andorsen, Ahmed L A, Emaus N, Klouman E. (2017) A prospective cohort study on risk factors of musculoskeletal complaints (pain and/or stiffness) in a general population. The Tromso study. PLoS One. 12(7), 0181417.
- 27.Wijnhoven H A H, H de Vet, Picavet H S J. (2006) Prevalence of musculoskeletal disorders is systematically higher in women than in men. , Clin J Pain 22(8), 717-724.
- 28.Punnet L, Herbert R. (2000) Work-Related musculoskeletal disorders: is there a gender differential, and if so, what does it mean?. , In: Goldman M B, Hatch MC Eds 474-492.
- 29.Jussila L, Paananen M, Näyhä S, Taimela S, Tammelin T. (2014) Psychosocial and lifestyle correlates of musculoskeletal pain patterns in adolescence: a 2-year follow-up study. , Eur J Pain 18(1), 139-146.
- 30.El Ansari WE, Oskrochi R, Haghgoo G. (2014) Are students’ symptoms and health complaints associated with perceived stress at university? Perspectives from the United Kingdom and Egypt. , Int J Environ Res Public Health 11(10), 9981-10002.
- 31.Solidaki E, Chatzi L, Bitsios P, Markatzi I, Plana E. (2010) Work related and psychological determinants of multi-site musculoskeletal pain. , Scand J Work Environ Health 36(1), 54-61.
- 32.Morken T, Riise T, Moen B, S H Hauge, Holien S. (2003) Low back pain and widespread pain predict sickness absence among industrial workers. , BMC Musculoskelet Disord 4(1), 21.
- 33.Miranda H, Kaila-Kangas L, Heliövaara M, Leino-Arjas P.Haukka E et al (2010) Musculoskeletal pain at multiple sites and its effects on work ability in a general working population. Occup Environ Med. 67(7), 449-455.
- 34.Sandmark H, Wiktorin C, Hogstedt C, Klenell-Hatschek E K, Vingård E. (1999) Physicalwork load in physical education teachers. Appl Ergon. 30(5), 435-442.
Cited by (2)
This article has been cited by 2 scholarly works according to:
Citing Articles:
Slovenian Journal of Public Health (2025) OpenAlex Semantic Scholar Crossref
International Journal of Environmental Research and Public Health (2022) OpenAlex Semantic Scholar Crossref