
Outcome Assessment of Open Foot Injuries in A Teaching Hospital in Ghana
Abstract
Purpose
Foot injuries are common in low- and middle-income countries and continue to increase in incidence due to the surge in the use of motorcycles as means of transport.Yet, there is scanty data on the incidence and outcomes of treatment of open injuries to the foot in the developing world.We aimed to determine the incidence and functional outcomes of open foot injuries that are treated in a teaching hospital in Ghana.
Methods
We used a structured questionnaire to record the type of open foot injury, the mechanism of injury, any concomitant injuries, the time interval between injury and arrival at the hospital for treatment as well as the type of treatment instituted.
Recruited patients were followed up for six months, complications resulting from the injury or its treatment were recorded for each patient. The function of the foot after healing of the injury was measured using a questionnaire-based visual analogue outcome scale of the American Foot and Ankle Society. Regression and chi-square analysis were used to evaluate potential associations.
Results
Over a four-month period, a total of 81 cases of open injuries to the foot were recorded. Out of this figure, 55 patients (67.9%) were males and 26 (32.1%) were females. It was found, that 66.7% aged between 19 and 49 years, 76.5% of the injuries occurred on the road and 29.7% was motor cycle related. Pedestrians are the most afflicted (61.7%). The treatment outcomes of traumatic amputations, open phalangeal fractures, dorsal skin degloving and lacerations were good. Gustillo-Anderson grade IIIB open fractures with associated plantar skin degloving had the worst outcomes with residual pain on weight bearing, bigger foot, inability to wear previous shoes and inability to tiptoe on the affected foot.
Conclusions
Open injuries to the foot are common in Ghana and exert a significant health burden, particularly on active young males. Long term disability may occur, even after adequate treatment of open fractures involving the foot.
Article Information
- Received
- Accepted
- Published
Academic Editor: Sanjeev Chaudhary, Associate Professor, Government Medical College, Nagpur, Maharashtra, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Dominic Konadu-Yeboah, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Correspondence: Dominic Konadu-Yeboah, Orthopaedic and Trauma Surgeon, Korle-Bu Teaching Hospital, Accra, Ghana —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
The prevalence of foot injuries has increased in the last decade in our sub-region because of rising motor vehicular collisions, social conflicts and domestic related accidents 1.
Motorcycle accidents cause severe injuries to the foot with metatarsal fractures being the most common; eventhough, foot injuries have a low mortality rate, they require prompt treatment to minimize long-term morbidity and disability 2.
In addition, foot injuries are often missed or underestimated in the initial care of patients with polytrauma3. However, injuries to the lower extremity impart significant influence on the long-term outcome of polytraumatized patients 3.
It is important to understand the unique features of foot injuries in order to make an accurate diagnosis and offer appropriate treatment. Successful management of open hindfoot fractures for example, is a formidable orthopaedic challenge particularly if associated with soft-tissue disruption 4.
Open fractures of the foot may require long periods of hospital care and immobility. Thus, open injuries involving the hind foot result in posttraumatic osteoarthritis, long term ambulatory dysfunction and joint stiffness. Few patients return to their pre-injury level of activity in spite of accurate reduction and stabilization and multidisciplinary approach and appropriate timing of treatment are necessary to improve outcomes 4.
In open fractures of the calcaneus patients with plantar wounds and multifragmentary fractures are expected to have particularly poor functional results 5. Moreover, open fractures of the hind and midfoot have a high amputation rate 6.
There is scanty data on the incidence and outcomes of treatment of open injuries to the foot in the developing world.This study, therefore, sought to provide information about the functional outcomes of open foot injuries that are treated in a teaching hospital in Ghana.
Methods
Study Design
our study was a prospective cohort study
Study Setting
We undertook this study at the Accident Centre of the Korle-Bu Teaching Hospital. The Korle - Bu Teaching Hospital is situated in Accra, Ghana and provides specialist services to people from all over Ghana as well as people from neighbouring countries. It provides Trauma and Orthopaedic services for patients 24 hours a day.
It is currently the third largest hospital in Africa and the leading national referral hospital in Ghana.
The hospital has 2,000 beds and 17 clinical and diagnostic departments. It has an average daily attendance of 1,500 patients and about 250 patient admissions a day.
Data Gathering
All patients who presented to the accident centre of the Korle-Bu Teaching Hospital with an open injury to the foot over a four-month period, from 1st July 2012 to 31st October 2012 and who met inclusion criteria were recruited into the study, using consecutive sampling method, and followed-up for six months (until 30th April, 2013).
A structured questionnaire was administered to each study participant at the time of presentation to the emergency centre, to record the type of open foot injury, the mechanism of injury, any concomitant injuries, the time interval between injury and arrival at the hospital for treatment as well as the type of treatment instituted. For patients who underwent operative treatment, the type of surgery was recorded.
The study participants were then followed-up for six months, at clinic visits and by telephone interview and complications resulting from the injury or its management were recorded for each patient. The function of the foot after healing of the injury was measured using the validated questionnaire-based subjective visual analogue outcome scale of the American Foot and Ankle Society 13.
The Gustillo-Anderson classification system, which is widely used to classify open fractures 14, 15 was used to classify open fractures of the foot in our study. Clinical examination and radiographs were used as tools of measurement.
All Necessary Radiographic Investigations were Done Accordingly and Findings Recorded
X-rays of the foot were taken to confirm the diagnosis of foot fractures, special views were taken as required. Computerized tomography scan and magnetic resonance imaging were requested as indicated. The imaging results were interpreted with the help of a radiologist. Complications of injury and complications of treatment that arose during the follow-up period were recorded.
Inclusion and exclusion criteria: only patients with injuries to the foot in which there was a full thickness break in the skin of the foot, as determined during the treatment of the injuries, were considered for this study. On the other hand, patients with non-mechanical trauma such as burns and those who had underlying bone disease were excluded from the study as well as patients with diabetes or underlying immunosuppression.
Patients with traumatic foot injuries with lack of clear identification, missing or lack of complete history on mechanism of injury and absence of relevant imaging were not included in the study.
Patients with foot contusions (in which the skin was unbroken) and penetrating wounds were not enrolled into the study.
Statistical Analysis
Descriptive statistics were summarized using means, standard deviations, and ranges to assess demographics, physical examination findings, and outcome data. Analyses used 95% confidence intervals in SPSS version 12.0, and p-values below 0.05 were considered statistically significant.
This study was approved by the Ethical and Protocol Review Committee of the University of Ghana Medical School (project number MS-Et/M.9-P3.1/2012-13).
Results
Over the four (4) months period of this study 81 cases of open foot injuries were recorded. Out of this number, 55 patients (67.9%) were males and 26 (32.1%) were females. The majority of the patients aged between 19 and 49 years accounting for 66.7% of all cases. The youngest patient aged 2years and the oldest 80 years. (Table 1)
Table 1. Distribution of 81 open foot injuries by age, gender, site of injury, mechanism of injury, nature of injury and time lapse from injury to hospital arrival.| Age | Number of patients | Percentage (%) |
|---|---|---|
| 0-5 | 5 | 6.2 |
| 6-18 | 12 | 14.8 |
| 19-49 | 54 | 66.7 |
| >50 | 10 | 12.3 |
| Gender | ||
| Males | 55 | 67.9 |
| Females | 26 | 32.1 |
| Site of injury | ||
| Road | 62 | 76.5 |
| Home | 12 | 14.8 |
| Work | 7 | 8.7 |
| Mechanism of injury | ||
| Motorbike rider | 8 | 9.9 |
| Motorbike pillion | 2 | 2.5 |
| Motorbike related pedestrian | 14 | 17.3 |
| Car related pedestrian | 36 | 44.4 |
| Car driver | 1 | 1.2 |
| Fall by triping | 2 | 2.5 |
| Fall from height | 2 | 2.5 |
| Hit by falling object | 14 | 17.2 |
| Physical assault | 2 | 2.5 |
| Nature of injury | ||
| Open metatarsal fracture | 13 | 16 |
| Open phalangeal fracture | 2 | 2.5 |
| Degloving injury | 8 | 9.9 |
| Avulsion injury | 8 | 9.9 |
| Traumatic amputation of foot | 1 | 1.2 |
| Traumatic amputation of toe | 1 | 1.2 |
| Laceration | 48 | 59.1 |
| Time lapse from injury to hospital arrival | ||
| Within 6hrs | 60 | 74.1 |
| 6-24 | 12 | 14.8 |
| >24 | 9 | 11 |
Most open foot injuries occurred on the road, involved pedestrians and presented to hospital within 6 hours after injuryFalling objects caused the highest number of lacerations. These falling objects included: broken glasses, broken bottles, roofing sheets, and sharp metals.
Six of the open metatarsal fractures involved just one metatarsal (four involved the right foot and two, the left foot). In three patients the fracture involved all the five metatarsals, of which two involved the right foot and one, the left foot. There was no case of bilateral open metatarsal fracture recorded in the period of the study.
In total, nine right feet and four left feet were involved in the open metatarsal fractures. No case of open calcaneal, open talar, navicular, cuboid or cuneiform fracture was found during the study period of four months. Out of the 81 patients studied, only two of them representing 2.5% were detected to be under the influence of alcohol. (Table 2, Table 3).
Table 2. Distribution of injury type by mechanism of injury| Type of injuries | Mechanism of injury |
|---|---|
| Open metatarsal and open phalangeal fracture | Motor bike – pedestrian |
| Traumatic amputation of foot | Car – pedestrian |
| Traumatic amputation of toes | Motor bike – rider |
| Degloving injury | Car – pedestrian |
| Avulsion injury | Car-pedestrian |
| Type of injury | Type of treatment |
|---|---|
| Lacerations | Debridement + suturing |
| Open metatarsal fractures | Debridement, K-wire fixation and P.O.P back slab |
| Avulsion injury | Debridement and P.O.P. back slab, split skin grafting (delayed) |
| Degloving injury | Debridement, suturing and P.O.P back slab, split skin grafting (delayed) |
| Metatarsal + phalangeal fracture | Debridement, K-wire fixation and P.O.P. back slab |
| Traumatic amputation of foot | Debridement, re-fashioning and P.O.P. back slab |
| Traumatic amputation of toes | Debridement, re-fashioning and P.O.P. back slab. |
| Laceration + Degloving injury | Debridement, suturing and P.O.P back slab |
| Laceration + Avulsion injury | Debridement + P.O.P back slab, split skin grafting (delayed) |
Associated Injuries
Ten of the patients sustained associated injuries apart from the injuries they sustained to the foot. This represented 12.3% of the total number of patients in the study. The mechanisms of injury in these patients involved high energy transfer. The table below depicts the type of associated injuries sustained by the 10 patients, the original injury sustained to the foot and the mechanism of injury. (Table 4).
Table 4. Distribution of Patients according to the type of open foot injury the mechanism of injury and the nature of associated injuries.| Nature of open foot injury | Associated injury | Mechanism of injury |
|---|---|---|
| Laceration on dorsum, right big toe | Left palm lacerations | Knock down by falling object |
| Avulsion injury | Closed tibia/fibula fracture | Car – pedestrian |
| Laceration + avulsed toe nail, left big toe | Cervical cord injury + tetraplegia | Fall from height |
| Laceration, dorsum of right foot | Bilateral open tibia/fibula fracture | Car– pedestrian |
| Open metatarsal fracture of the right foot | Facial abrasion | Car– pedestrian |
| Laceration plantar aspect of left 3rd toe | Closed left radial and ulna shaft fracture | Car – pedestrians |
| Open fracture, shafts of all five right metatarsals. | Closed right tibia/fibula fracture | Motor cycle – pedestrian |
| Open left metatarsal fracture | Right parietal scalp laceration | Motor cycle – pedestrian |
| Laceration, dorsum of right foot. | Abrasion on right hand | Physical assault |
| Right 4th toe laceration | Cervical cord injury | Fall from height |
Treatment of Open Foot Injury
The open foot injuries in this study were treated by initial wound debridement followed by other procedures depending on the nature of the injury. Lacerations were debrided and sutured; where tendons were severed they were repaired as necessary, using standard repair methods. Open fractures were, after debridement, stabilized with K-Wires and thereafter, reinforced with a Plaster-of-Paris slab. Where skin defects could not be sutured, wound coverage was achieved by split skin grafting. None of the 81 patients studied required flap cover for a soft tissue defect. (Figure 1, Figure 2).
Figure 1. Open fracture of the shafts of the right 2nd, 3rd ,4th and 5th metatarsals, treated by normal saline irrigation, debridement and kirchner wire stabilisation.
Download figure
Figure 2. Check x-rays, anteroposterior and lateral views of the open right metatarsal fracture in figure 1, showing stabilization with 2.0-mm kirchner wires.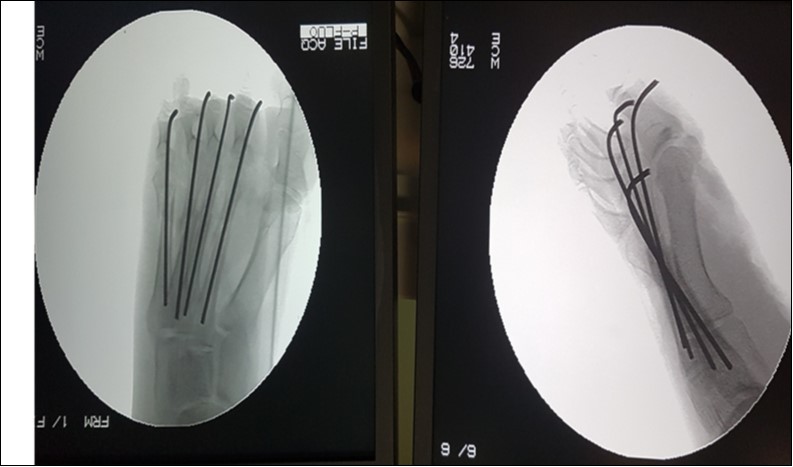
Download figure
Treatment Outcomes of Open Foot Injuries
At the end of the 6-month period, the functional outcomes of treatment were evaluated using a questionnaire-based subjective visual analogue outcome scale of the American Foot and Ankle Society.
Functional outcome of the foot was adjudged as ‘poor’, ‘fair’, ‘good’ or ‘excellent’. The patients who had lacerations without tendon involvement, constituted 34.6% of the patients studied. These patients had outcomes which were excellent. Those patients whose lacerations were associated with tendon division had a good outcome.
Degloving injuries to the foot had fair results and involved 7.4% of the patients, most of whom had complaints of persistent foot pain worsened by weightbearing. The pain was worse in patients in whom the degloving injury involved the sole of the foot. The outcomes of patients who sustained open fractures of one or more phalanges were fair to good. Traumatic toe amputations had a good outcome.
The proportion of patients who sustained open metatarsal fractures constituted 18.5% of the patients studied. The higher the Gustillo-Anderson grade of the open metatarsal fracture, the worse the outcome.
Those who had Gustillo-Anderson grade IIIB open metatarsal fractures with associated plantar skin degloving had the worst outcome with most of them complaining of pain on weight bearing, bigger foot, inability to wear previous shoes and inability to tiptoe on the affected foot.
Degloving injury to the dorsum of the foot with extensor tendon avulsion had persistent foot pain, a limp, itchy scar and moderate limitation in climbing a stair case. There were no late amputations and no deep infections found.
Discussion
It was found, in our study, that of the 81 patients with open injuries to the foot, 66.7% aged between 19 and 49 years, 76.5% of the injuries occurred on the road and 29.7% was motor cycle related. Pedestrians are the most afflicted (61.7%). This finding is similar to a study by Afukaar and others 7 who reported that road traffic trauma is a major cause of morbidity and mortality in Ghana often involving people of the productive age group. The comparatively higher rate of motor cycle-crash foot injury in Ghana could be attributed to the increasingly high utilization of motor cycles as a means of transport in Ghana.
Out of the total number of patients studied, 55 (67.9%) were males and 26 (32.1%) were females. The male preponderance in foot injuries has been found in other studies. In his analysis of the trauma registry, Tadros 8 reported that 7% of all trauma patients presenting to their unit over their study period had foot injuries with a male: female ratio of 10:1 and the mean age was 34 years.
In our study, the gender difference in the likelihood of sustaining open foot injuries was statistically significant with a p-value of < 0.05. However, there was no statistically significant association between gender and the type of injury sustained (p-value= 0.376).
A research on the impact of foot injuries on the rehabilitation of polytrauma patients documented that patients with foot injuries often had more long-term morbidity. This research suggested that more attention needed to be paid to what might be seen as less serious injuries 9. Similarly, the findings of our study confirm this fact that foot injuries impart a significant morbidity on patients, with 18.5% of patients having persistent foot pain, a larger foot, inability to wear their previous shoes and unable to resume their previous occupations, six months following the injury.
Most of the participants of this study suffered car related pedestrian foot injuries (36%). This is similar to a study conducted in Germany by Dietmar Otte and Tim Philemon 12 who reported a high percentage of lower extremity injuries among pedestrians in car collisions on roads.
A study of motorcycle accidents at the Mulago Hospital in Uganda reported the prevalence of about 2-5 % of foot injuries1. In this study, motor cycle related open foot injuries alone accounted for 29.7% of all causative agents put together. Of this percentage, 9.9% were motor cycle riders, 2.5% motor cycle pillions and 17.3% were motor cycle-injured pedestrians. Thus, the proportion of foot injuries due to motor cycles is much higher in Ghana as compared to the findings of the study conducted at the Mulago Hospital in Uganda. The comparatively higher proportion of injuries to the foot in Ghana could be attributable to the recent spate of motorcycle crashes in Ghana.
Outcomes of Treatment
The poor outcome of Gustillo IIIB open fracture of the metatarsals could be explained by the severity of these injuries, which involved extensive disruption of the arches of the affected feet which could not be restored after treatment.
The residual foot pain in these patients limited resumption of previous occupation. This finding agrees with that which showed that injuries below the knee were tied to higher rates of unemployment, longer sick leave time, more pain, more follow-up surgeries and decreased overall outcome as measured by instruments such as American Orthopaedic Foot and Ankle Score 3.
Jeffers and colleagues 2 reported that despite modern soft-tissue management techniques and the greater number of implant options, good clinical outcomes following traumatic foot injuries can be difficult to achieve 10.
Similarly, it was observed in this study that all the patients who had severe soft tissue destruction had a comparatively poor outcome.
Kuo and his co-workers 11 carried out a retrospective study among ninety-two adults treated for foot injury, forty-eight patients with forty-eight injuries were followed for an average of fifty-two months. The patients at the end of the follow-up period had mild pain, decreased recreational function, and needed orthoses. They observed poorer outcomes despite anatomical reduction and screw fixation. Similarly, the patients who had osseous involvement in the open foot injury, in our study, had a poorer outcome.
Conclusion
Open injuries to the foot are a significant cause of long term disability in Ghana and mostly involve males (67.9%), aged between 19 and 49 (66.7%) occur on the road (76.5%). Pedestrians are the most afflicted (61.7%). Soft tissue disruption, particularly plantar skin involvement, is a significant predictor of poor outcome. The outcome, after treatment, of Gustillo-Anderson grade IIIB open metatarsal fractures with associated plantar skin degloving is poor with residual pain on weight bearing, bigger foot, inability to wear previous shoes and inability to tiptoe on the affected foot.
Recommendations
Further studies on open fractures of the foot are recommended to generate more evidence on treatment methods that offer the best functional outcomes.
A study with a longer follow-up time is recommended to gather data on long term outcomes of open foot injuries.
Low- and middle-income countries should provide pedestrian walkways along roads and enforce their use by pedestrians in order to minimize the high pedestrian-related car injuries to the foot.
The outcomes of open foot injuries could be improved with
References
- 1.E K Naddumba.A cross-sectional retrospective study of boda boda injuries at mulago hospital in kampala-uganda.
- 2.Jeffers R F, Tan H B, Kamath R NicolopoulosC, GiannoudisPV. (2004) Prevalence and patterns of foot injuries following motorcycle trauma. , J Orthop Trauma 18(2), 87-91.
- 3.Probst C,Richter M,LeferingR,Frink M,Gaulke R,KrettekC,Hildebrand F. (2009).Epub Nov 3 Incidence and significance of injuries to the foot and ankle in polytrauma patients--an analyss of the Trauma Registry of DGU.Injury.2010 Feb;41(2):. 210-5.
- 5.Berry G K, Stevens D G, Kreder H J, Schemitsch E, Stephen D J. (2013) 14, The Spectrum of Open Fractures of the Foot in Adults. Foot And Ankle International.
- 7.Afukaar F K, Antwi P, Ofosu-Amaah S. (2003) . Mar-Jun;1 Pattern of road traffic injuries in Ghana: implications for control.InjControlSafPromot.12: 69-76.
- 8.Tadros A M, Eid H O, Abu-Zidan F M. (2010) Epidemiology of foot injury in a high-income developing country. Injury. 41(2), 137-40.
- 9.TurchinDC SchemitschEH, McKee M D, Waddell J P. (1999) Do foot injuries significantly affect the functional outcome of multiply injured. 13(1), 1-4.
- 10.Annappa R, Jhamaria N L, Dinesh K V, Ramesh RH Devkant, Suresh P K. (2015) Functional and radiological outcomes of operative management of displaced talar neck fractures. Foot (Edinb). 25(3), 127-30.
- 11.Kuo R S, Tejwani N C, Digiovanni C W, Holt S K, Benirschke S K et al. (2000) Sangeorzan BJ: Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. , Nov;82-A 11, 1609-18.
- 12.Dietmar O, Tim P. (2001) Analysis and load assessment of secondary impact to adult pedestrians after car collisions on roads. IRCOBI conference 143-157.
- 13. (2005) American Orthopaedic Foot and Ankle Society (AOFAS). Evaluation of the foot function index. 21stAnnual Summer Meeting. , Boston, MA, USA