Abstract
We report a twin gestation with one fetus afflicted by a left sided Extra-Lobar Sequestration (ELS) in a morbidly obese mother. The ELS was complicated by a left pleural effusion in the second trimester unresponsive to maternal steroid administration. We discuss the need for repeat shunt placement, in the setting of maternal morbid obesity and twin gestation. Shunt replacement was necessary secondary to dislodgement. Delivery at 34 weeks gestation was followed by successful surgical removal of the ELS. At one year follow up the infant has complete expansion of the left lung with no morbidity.
Author Contributions
Academic Editor: Ramesh Bhat Y, Department of Pediatrics, Kasturba Medical College, Manipal University, Manipal, Udupi District, Karnataka, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Sathyaprasad Burjonrappa, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction:
Congenital lung malformations are being identified earlier during pregnancy and with greater accuracy owing to improvements in imaging technology. Such malformations include pulmonary sequestration (PS), congenital cystic adenomatoid malformation (CCAM /CPAM), bronchial atresia (BA), and bronchopulmonary sequestration (BPS) 1. Pulmonary sequestration can be subdivided into intra lobar (ILS) and extra lobar (ELS) variants 1. While most sequestrations have a benign outcome with regression during the third trimester, complications such as hydrops and maternal mirror syndrome can develop and contribute to fetal mortality and maternal morbidity2. Prenatal steroid administration and fetal surgery with thoraco-amniotic shunt placement or cyst aspiration have been described with varying success in the management of fetal pleural effusion and hydrops 3. We report the successful management of a fetus with a large lung malformation complicated by pleural effusion in the setting of maternal morbid obesity and twin gestation by thoraco-amniotic shunt placement.
Case Report:
A 37 year old G3P2 female was referred to the pediatric surgical clinic for a twin pregnancy with one of the twins having a large left sided lung mass. The mother had a BMI of 48 and had undergone lap band surgery in the past. The lung mass was detected at 22nd week of gestation and was noted to be homogenous and solid on ultrasound and had a Cyst Volume Ratio (CVR) of 1.4. The twins were dichorionic diamniotic. Twin A had a posterior placenta and twin B (twin with the lung mass) had an anterior placenta. The lesion was located in the left hemi thorax and did not have any associated pleural effusion at first. The differential diagnosis for this lesion included a Stoker Type3 CPAM, a mediastinal teratoma, and a diaphragmatic hernia6. The Twin B was superior in the uterus in a breech position to the right side with a vertical pocket of amniotic fluid measurement of 6.8cm. The Bio Physical Profile score was 10/10. While the middle cerebral artery and ductus venosus dopplers were normal, there was some drop off in the end diastolic flow in the umbilical artery Dopplers. The mother was placed on weekly hi-definition ultrasound follow ups. Echocardiogram showed no structural cardiac defect. Steroids (betamethasone 12mg IM, two doses, 24hours apart) were administered after the development of pleural effusion was noted at the repeat ultrasound performed at 24 weeks and at this point CVR had increased to 1.6. As there was an inadequate response to steroid administration, with the development of a mediastinal shift from the mass effect of the lesion and significant pleural effusion, aspiration of the pleural fluid was performed twice (at weekly intervals during the 26th and 27th week of gestation) with recurrence of the effusion. The pleural fluid analysis showed that it was transudate on both occasions. The volume aspirated on each occasion was about 20 ml. Ascites was also detected and 10 ml of abdominal fluid was aspirated during the second aspiration. It appeared that the fetus was developing hydrops. During the 30th week ultrasound showed a significant mediastinal shift to the right, a large liver with ascites, and increased fetal skin thickness. A thoraco-amniotic shunt was placed at the 30th week of gestation and another course of steroids administered Figure 1 and Figure 2. The significant maternal subcutaneous fat would allow only a direct lateral access into the pleural cavity. The twin and mother were doing well with no symptoms. However, three weeks later, the fetus was able to dislodge the 'double-J' catheter and a second thoraco-amniotic shunt was placed because of recurrence of pleural effusion. While this was successful initially, the combination of the twin pregnancy and interventions led to premature delivery of the twins at 34 weeks gestation. MRI was not considered in the evaluation because of the large BMI.
Twin B underwent surgical intervention on day of life3. A large ELS was removed by thoracotomy after ligation of the systemic vascular supply Figure 3. Twin A had an uneventful neonatal intensive care unit (NICU) stay. Twin B made a uneventful recovery and was discharged from the NICU after a two week stay. At one year the infant is doing well and has almost caught up with his twin in terms of body weight and milestones.
Figure 1. Antenatal Ultrasound demonstrating the guide wire and shunt in position. The thickness of the amniotic fluid is being measured by the markers.
Figure 2. Deployed shunt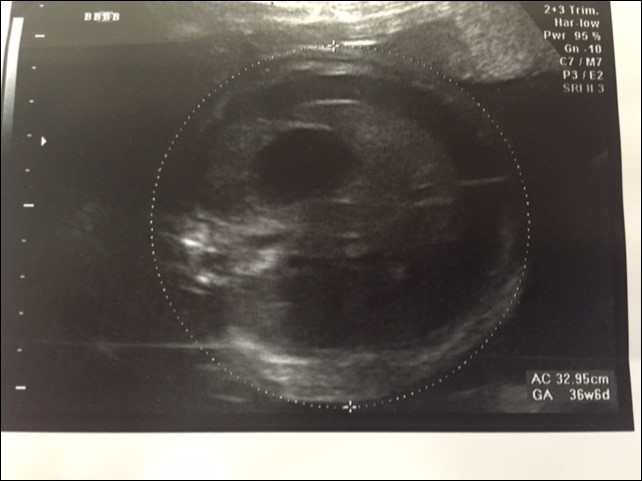
Figure 3. Post natal thoracotomy showing the CLM with a systemic blood supply being removed sucessfully.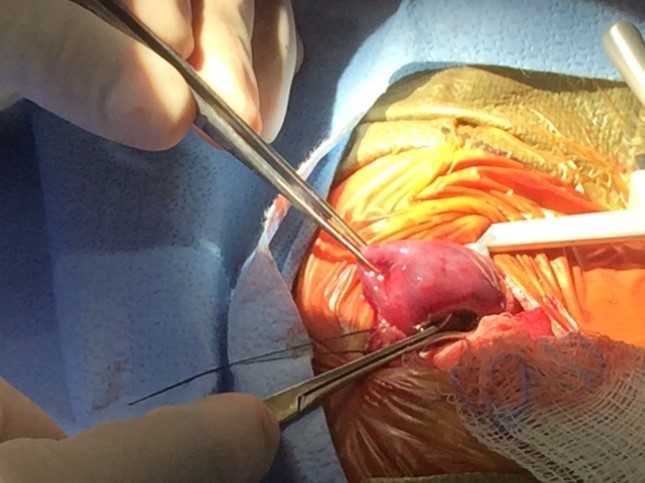
Discussion:
A majority of lung malformations have an excellent prognosis. While it may not be possible to differentiate between the different pulmonary cystic malformations based on imaging findings in the prenatal period it is possible to have a common strategy in the management of different kinds of lesions which may have cross over in terms of both pathological features and clinical presentations. Large lesions with a CVR>1.6 however are more prone to developing complications4. In such cases, cardiac compression from the mass and impairment of venous return may result in the development of hydrops. Hydrops is defined as the presence of fluid in more than one fetal body cavity and its reported incidence in lung masses varies from 5-30%2, 3. In our patient the etiology of the hydrops was likely a combination of mass effect and cardiac shunting associated with systemic arterial supply and venous drainage in extra lobar sequestration. Surveillance by biweekly ultrasound after detection of lung malformation is necessary to detect development of these complications. MRI is an excellent imaging technology to distinguish between the different types of pulmonary malformations7. In ELS associated anomalies include diaphragmatic hernia, congenital heart disease, and pulmonary hypoplasia5. In many instances regression of the lung malformation is noted in the third trimester. Regression, prior to birth, has been noted in nearly 67% of pulmonary sequestration and only 15% of CPAM1. However even after complete sonographic resolution, postnatal CT scans reveal the radiological abnormality in 95-100% of cases6.
Once the lung malformation is complicated by the development of a pleural effusion steroid administration can be considered. Steroids act by decreasing the fluid secretion from the malformation and also by facilitating its re-absorption8. While steroids can be tried in all types of lung malformation, they are generally most effective in the microcystic variant of CPAM, where they have made the need for fetal surgical intervention obsolete 8. We tried betamethasone on two different occasions, two weeks apart. Studies have shown that fetuses have a reduction in lesion size between 62-73% and hydrops resolution in 54-80% with a single course of bteamethasone in the case of CPAM.8 The same authors trialed multiple courses of steroids in both CPAM and non-CPAM congenital lung lesions with reasonable clinical response9 They noted in their study a higher rate of fetal intervention (including fetal surgery), an earlier age at post natal surgery, and a prolonged mechanical ventilator support requirement in the neonates born after multiple steroid doses. We have resorted to the use of steroids in the late second trimester in cases of CLM complicated by pleural effusion and have repeated the regimen if necessary. As Parenteau and colleagues have suggested, this also helps prepare the fetus (by increasing pulmonary surfactant levels) for preterm delivery if fetal intervention is complicated by labor and subsequent delivery.
In fetuses over 30 weeks gestation one could consider aspiration or shunt placement. In our experience, aspiration is usually quickly followed by fluid reaccumulation in the pleural space. In our patient, the presence of twin gestation complicated shunt placement. The twins were dichorionic diamniotic. It was necessary to pin the infant by external pressure to facilitate ultrasound guided catheter placement. The fact that the mother had a BMI of 48 did not help matters. Having a long access needle is important and patient positioning is critical in obtaining an adequate window to accurately place the shunt. Shunt placement is very effective in relieving the mediastinal shift and cardiac compression. However dislodgement and inadequate shunt function is a problem as we noted in our patient. A direct approach through the mid-clavicular line in the chest wall has a higher dislodgement rate as compared to a more superior and lateral approach. The fetus was noted 'live' displacing the shunt that we had placed needing immediate replacement10 Complications mentioned of TA shunts are the development of constriction bands if the amniotic end of the shunt causes a constriction band around an extremity and rib malformations10. Presence of maternal mirror syndrome should lead to consideration of preterm delivery. Large maternal BMI and twin gestation should not contraindicate consideration for TA shunt placement. Need for a second shunt placement should be determined by fetal maturity and gestational age. With the twin gestation, the extra time spent in utero helped in the excellent outcomes seen in both twins, with twin A needing a short NICU stay prior to discharge. In our patient, shunt placement facilitated delivery in the third trimester which contributed to the excellent outcome.
We proceeded with resection of the lesion by thoracotomy at 4 days of age as the neonate was symptomatic. The early resection has theoretical benefits as it decreases the risk of infection, potential for pneumothorax, and allows for better growth of the remaining lung tissue. It further reduces the diagnostic dilemma of the lesion actually being a pleuropulmonary blastoma (PPB) and facilitates reestablishment of normal lung capacity 1.
Thoraco amniotic shunt should be considered in fetus with symptomatic pleural effusion and hydrops. Maternal morbid obesity and twin gestation should not preclude its use as illustrated in this case report. One should not hesitate to replace displaced shunts, in case of recurrence of effusion, as it may buy valuable in-utero time and facilitate pulmonary development and maturation and prevent post natal complications.