Abstract
Pericentric inversions in chromosome 10 are regarded as both common and rare conditions, based on breakage and rearrangement within each specific segment.
We present phenotypic and cytogenetic characterizations of a rare recombinant chromosome 10, namely inv(10)(p11q26), in a 13-month-old flabby girl associated with a maternal pericentric inversion.
A review of the literature on the different aspects of this condition is also provided.
Author Contributions
Academic Editor: Huseyin Bekir, Professor Doctor in Department of Materials Science and Nanotechnology Engineering, KTO Karatay University, Konya, Turkey, Email: [email protected]
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Maryam Sotoudeh Anvari, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Inversions as a subclass of chromosome mutations constitute structural chromosome anomalies with arrangements in normal genetic material. A minimum of 2 breaks in 1 chromosome is required for the occurrence of inversion, 1, 3 in which the intercalated fragment rotates 180° and reinserts into the chromosome and the breaks reintegrate. If the inverted segment includes the centromere (with the involvement of both arms), the inversion is classified as pericentric and if the 2 breaks appear on the same side of the centromere (in the same arm), the inversion is categorized as paracentric. 2
Most inversions are usually balanced rearrangements and do not cause an abnormal phenotype in carriers. However, if the breakage occurs within a functional gene, there is an increased risk of meiotic errors, which can lead to infertility or early spontaneous fetal loss. 1 On the basis of a study on 33 families, Collinson et al 4 revealed that a small pericentric inversion in chromosome 10, namely inv(10)(p11.2q21.2), is a common chromosomal variant rather than an aberration.
Drawing upon comparative genomic hybridization array, Ciuladaite et al 5reported a large pericentric inversion in chromosome 10, namely inv(10)(p15.1q26.12), in 2 relatives in 1 family with idiopathic intellectual disability as a rare chromosomal abnormality.
The present report describes a patient with a pericentric inversion in chromosome 10 with hypotonia and convulsion, in association with a maternal pericentric inversion.
We employed various online data bases specifically Google Scholar, Scopus, and PubMed—on English articles in September 2017. We tested various keywords such as “pericentric inversion in chromosome 10”, “chromosome 10 inversion”, and “inv(10)(p xx q xx)” in nontumoral subjects in these databases.
Case Report
A 13-month-old girl was referred to our center for chromosome evaluation via the observation of facial dysmorphism, hypotonia, convulsion, and developmental delay by a neurologist.
The only child of healthy-looking unrelated parents, the patient was a full-term baby with 3500 g birth weight. She had a prenatal history of oligohydramnios, with no evidence of abortion in the mother. Moreover, she had major clinical malformations—comprising dolichocephaly, hypertelorism, micrognathia, low-set ears, frontal bossing, moderate mental retardation, convulsion, bilateral hip dislocation, pectus excavatum, muscular hypotonia, walking difficulty, and umbilical hernia. Laboratory tests were within normal limits. Family history and karyotype analysis demonstrated that a phenotypically normal maternal uncle was a carrier for this chromosomal anomaly. Additionally, she had twin maternal aunts with a phenotype similar to hers who had died at 6 months and 19 years old, respectively, without genetic study.
After blood sampling, lymphocyte culture on Na-heparin peripheral blood was performed using conventional methods in an RPMI (Roswell Park Memorial Institute) 1640 medium supplemented with phytohemagglutinin and fetal bovine serum at 37˚C for 72 hours. Thereafter, the cells were harvested by adding colcemid before they were treated with a hypotonic solution (0.075 M KCl) and fixed using 3:1 methanol/glacial acetic acid. The metaphases were stained with a trypsin–Giemsa procedure (Giemsa-banding). The constitutive heterochromatin at the centromeres was evaluated via C-banding stain, with the chromosomes exposed to a saturated alkaline solution of barium hydroxide, before Giemsa staining.
Twenty metaphases were analyzed using Cyto Vision software. Chromosome analysis revealed that all the cells had a pericentric inversion in 46,XX,inv(10)(p11q26) in Giemsa-banding. This finding was rechecked in C-banding, which resulted in the extension from the pericentromeric region to almost the near telomere in the short arm of chromosome 10 (Figure 2 and Figure 3).
Cytogenetic study was also performed in the patient’s parents. The mother was a carrier with an identical pattern, whereas the father had a normal karyotype. Chromosome analysis also showed a large pericentric inversion in chromosome 10, involving the region between bands p15 and q26, in 1 maternal uncle. The phenotype of the mother and uncle was normal. Figure 1 is a simplified pedigree of the patient’s maternal family.
Figure 1. Maternal family pedigree.
Figure 2. Karyotype of 46, XX, inv (10)(p11, q26) in the girl. (G banding)
Figure 3. Karyotype of 46,XX, inv (10)(p11, q26) in the mother. (C banding)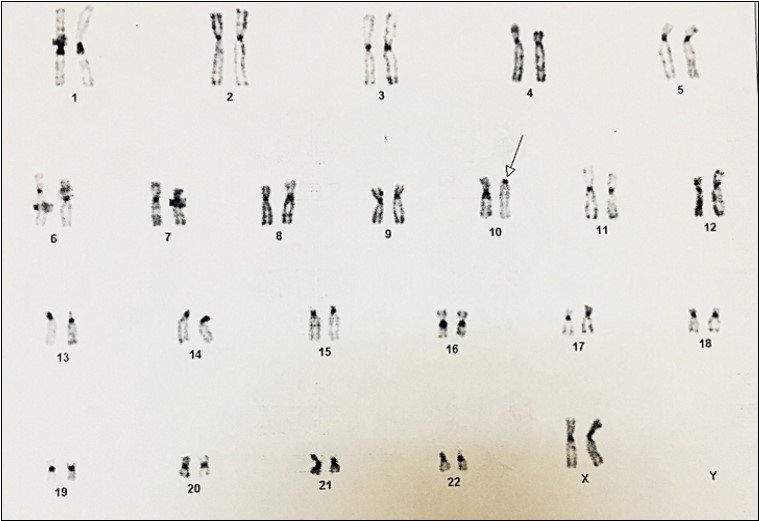
Discussion
The most common pericentric inversion reported in humans is in chromosome 9, with an incidence of 1.98%, especially in African Americans. 7 Demirhan et al 6 suggested that the 10p-q critical regions are involved in the pathogenesis of aggressive behaviors and hyperactivity as genetic neurodevelopmental disorders.
Table 1. Details of 59 cases of pericentric inversions in chromosome 10| Researcher(s) | Karyotype theme | Clinical Impression | Ref. Number |
| Bedeschi et al. (2006) | duplication of chromosome 10p was present in one case, inherited from a pericentric chromosome 10 inversion | Agenesis of the corpus callosum | 10 |
| Chen et al (2016) | rec(10) dup(10p)inv(10)(p11.2q26.3) in a fetus associated with paternal pericentric inversion | A 35-year-old woman underwent amniocentesis at 18 weeks of gestation because of an advanced maternal age | 11 |
| Gilling et la. (2006) | pericentric inv(10)(p11.2q21.2) in 20 unrelated families | phenotypically silent | 8 |
| Ciuladaite et al . (2014) | Relatives with opposite chromosome constitutions, rec (10) dup (10p) inv (10) (p15.1q26. 12) and rec (10) dup (10q) inv (10) (p15. 1q26. 12), due to a familial | idiopathic intellectual disability | 5 |
|---|---|---|---|
| Ravel et al. (2006) | 46, XY, inv(10) (p12q23) 46, XY, inv (10(p15.3q21.1) 46,XY,inv(10) (p12q21.1) survey of over 10 000 sperm donor karyotypes | Not Applicable(N/A) | 12 |
| Collinson et al. (1997) | Pericentric inv (10) (p11.2q21.2) In 33 families | A normal phenotype in 21/33 families. | 4 |
| de la Chapelle et al. (1974) | -46, XY inv(10) (p1q21) -46, XX inv(10)(pllqll) | -Childless at age 34. Hypogonadotrophic hypogonadism. Delayed neuromuscular development Hypertelorism, broad forehead. Agenesis of the corpus callosum. Ambiguous genitalia. | 13 |
| Axelsson et al. (1984) | an inversion on chromosome 10 | 1/134 patients with paranoid psychosis | 14 |
| Cozaru et al. (2012) | 1 case with inversion on chromosome 10 | 1/229 couples with reproductive disorders | 15 |
| Helszer et al. (2003) | 46, XY, inv (10) (p15.2q11.22). ish inv(10)(p15.2q21.3)(p15×3)(q21×3)(p15conq21×2) | In a patient with hypogonadotropic hypogonadism | 9 |
| Morin et al. 2017) | inv(10)(p11.2q21.2) | reproductive pathology | 16 |
| Thomas et al. ( 2008) | inv(10) (p11.2q21.2) | N/A | 17 |
| Deloukas et al. (1973) | Pericentric inversion, inv (10), in a mother and aneusomy by recombination, inv (10), rec (10) (p15, q24), in her son | 18 | |
| Kosztolányi et al. (1995) | a pericentric inversion of chromosome 10 | Craniofacial anomalies, arachnodactyly, and severe developmental failure protruding eyes, feeding difficulties, and mental retardation. | 19 |
| Lorda -Sanchez et al. (1999) | pericentric inversion of chromosome 10 46, XX (p13;q22) pat | Encephalomyopathy with MELAS and Kearn-Sayre syndrome features. | 20 |
| Lin et al. (1998) | pericentric inversion of chromosome 10, inv (10) (p11.2q21.2) | In 2/8, affected persons with familial eosinophilia | 21 |
| Teyssier et al. (1983) | Inv (10) (p15q11) and inv (10)(p11q21) | in two infertile men | 22 |
| Lansky et al. (1981) | Infant: 46, XY, rec (10), dup p, inv (10) (p11q26) mat. The mother: (46, XX, inv (10) (p11q26). | Ambigous genitalia and Trisomy 10p phenotype ( Dolichocephaly, Frontal bossing Long narrow face, Protruding occiput, Hairlip, Cleft palate Palpebral fissures, long and horizontal, Arched eyebrows Hypertelorism, Broad nasal bridge Turtle's beak, Large, low set, posteriorly rotated ears, Narrow thorax and pelvis, Mottled skin Scoliosis, Limbs Hyperflexed upper limbs, Camptodactyly Clinodactyly, Lower limbs abducted, flexed, Clubfoot, Hypotonia, Hypoplastic male genitalia) | 23 |
| Yunis et al. (1981) | 46, XY, der (10) (10pter→10q25: 10p12→ 10pter) mat. | Developmental delay, malrotated right kidney, Bifid spina, face dysmorphism | 24 |
Table 1 lists a number of related studies in diverse areas for our topic.
Inversions are found across the spectrum of anifestations, from phenotypically silent to neurologic and reproductive consequences. With respect to the absence and presence of phenotypical changes, Gilling et al 8 were first to reveal that pericentric inv(10)(p11.2q21.2) is common in cytogenetic laboratories without association with phenotypical abnormalities among northern Europeans. Subsequently, Helszer et al 9 reported a case of idiopathic hypogonadotropic hypogonadism with 46,XY,inv(10)(p15.2q11.22).ish inv(10) and muscular weakness in the left lower limb.
We found only 1 article with a similar breakpoint (p11q26) in a child who had an additional trisomy 10p phenotype due to the duplication of chromosome 10 p arm with a phenotypically normal mother. 24 Trisomy 10p phenotype was pointed out by Lansky et al 24 and Bedeschi et al. 11
Given that our symptomatic patient had asymptomatic mother and uncle in the presence of identical cytogenetic abnormalities, it seems that her phenotypic changes cannot be completely explained with her karyotype findings.
Array-based comparative genomic hybridization is able to explore loss or gain of chromosome material much more precisely than conventional chromosome analyses; it can, therefore, help us explain dimorphism and specific rearrangements in patients.
The salient limitation of the present case report is that we had no access to the results of the patient’s blood analysis.
Conclusions
In summary, we described a flabby girl with developmental delay and convulsion and cytogenetic characterization of inv(10)(p11q26) associated with a pericentric inversion in first and second-degree relatives.
Acknowledgements
We thank Mrs Samira Ahamadpour and Mrs Hedyeh Vasei for their assistance in our cytogenetic study.