Abstract
Background
Adolescents is the transition from childhood to adulthood .Which is a time of opportunity, but also one of risk. In Ethiopia, sexual and reproductive health problems of adolescents are increasing from time to time related to many parents not feeling happy to discuss sexual matters in addition to early sexual commencement among adolescents.
Objective
This study was intended to assess parent-adolescent communication on sexual and reproductive health matters and associated factors among secondary and preparatory school students in Robe Town, Bale Zone, South East Ethiopia, 2017.
Methods
Institution based cross sectional study was conducted among 394 secondary and preparatory school students in Robe town from April 10-25, 2017. Simple random sampling technique was used. Data was obtained through the use of a self administered questionnaire and supplemented by focus group discussion with parents. Data was entered using Epi Data 3.1 and analyzed by SPSS 20. Descriptive statistics and logistic regression analyses were done. Data quality was assured through careful questionnaire design, pretest and training.
Results
One hundred eighty six (47%) of the study participants had discussed at least two SRH issues with their parents. Grade eleven students were about nearly five times more likely discussed on sexual and reproductive matters with their parent compared with grade nine students (AOR: 4.88, 95% CI: 1.76, 13.54). Those living with relatives were 3.13 times less likely discussed as compared to those students are living with both parents (AOR: 0.32, 95%CI: (0.12, 0.80) and the odds of discussion on SRH matters is 2 times higher among females compared with their counterpart (AOR=2.02, 95% CI: 1.25, 3.26).
Conclusions
Communication on sexual and reproductive health matters between adolescent and parent was low. Majority of student preferred to discuss with their peers than parent. Being ashamed, parents lack of communication skill and parent knowledge on SRH issues were the major reasons mentioned by the students for not discussing about SRH matters with their parents. Therefore; comprehensive family life education needs to be initiated for the students and parents. Sexual information exchange between peers needs to be strengthened.
Author Contributions
Academic Editor: Lucio Mango, S. Camillo-Forlanini General Hospital, Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Niguse Mengesha Habte, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Adolescents are defined by the United Nations as those between the ages of 10 and 19 1. Today there are 1.2 billion adolescents worldwide. Nearly 90 percent of them live in developing countries. An estimated 2.2 million adolescents, around 60 percent of whom are girls, are living with HIV, and many of them do not know they are infected. Every year, 1.4 million adolescents die from road traffic injuries, complications of child birth, suicide, violence, AIDS and other causes. Cause of adolescent death varies by region, and mortality patterns are associated with sex. In Latin America, injuries including homicide are the leading cause of death among adolescent boys; in Africa complications of pregnancy and child birth are the leading cause among adolescent girls aged 15-19 2.
Adolescents experience intense physical, psychological, emotional and economic changes as they make the transition from childhood to adulthood. Risk-taking is part of adolescence, and it is the duty of society to prevent risk and to mitigate consequences such risk-taking behavior 2. The communication helps to transmit values, beliefs and expectations about SRH matters to their adolescents 3.
In Ethiopia, a lot of adolescents often lack strong and stable relationships with their parents or other adults which are necessary to openly discuss reproductive health concerns. Therefore, many teenagers do not have access to reliable information regarding their RH needs. In most cultures, parents and family members are an influential source of knowledge, beliefs, attitudes, and values for children and young people. Parents often have the power to guide children’s development in sexual health matters, encouraging them to practice reasonable sexual behavior and develop good personal decision making skills 4.
Communication within the family appears to be particularly important during the adolescent years especially concerning reproductive health issues. Family communication affects adolescent identity formation and role–taking ability 5.
The majority of people become sexually active during adolescence. The use of contraceptives and condoms among young people, however, is low and unprotected sex is the second largest contributor to health risk in terms of the burden of disease in young people. As a consequence, each year, there are at least 100 million cases of sexually transmitted infections among young people, as well as more than 2.5 million unsafe abortions recorded for adolescents 1.
Specifically in Ethiopia, 13 percent of women age 15-19 have begun childbearing with 10 percent having had a live birth and two percent pregnant with their first child. Teenage mothers are more likely to experience adverse pregnancy outcomes and are more constrained in their ability to pursue educational opportunities than young women who delay childbearing. There has not been a study done related to this subject in our area, so it is important to know the prevalence of parent adolescent discussion on sexual and reproductive health issues in our area 6. Therefore, this study was conducted to assess parent adolescent communication on sexual and reproductive health matters and associated factors.
Methodology
Study Area and Period
The study conducted in Robe town, Oromia National Regional state, from April 10-25, 2017. Robe is capital town of Bale Zone located 430 Km south east of Addis Ababa. In the town there are two secondary schools and one preparatory school which are government schools. The total number of students attending in the academic year 2016-2017 in all secondary schools and preparatory school in Robe town were 4,200. From this 2031(48.36%) were males and 2169(51.64%) were females. The town has an estimated area of 8,024 hectares. According to the information obtained from the town statistics office report, the total population of the town was 80,501 with sex distribution of 40,843 were males and 39,658 were females. There is one hospital and one health center in the town.
Study Design
Institution based cross sectional quantitative study supplemented with qualitative method was employed. The source populations were all secondary and preparatory students attending grade 9-12, in Robe town were the source population. And those students from grade 9-12 who were selected for this study population for this study. Students aged 19 years old or less who are unmarried and attending secondary and preparatory school at the time of the study were included. And students who were married were excluded since they may have different characteristics as compared to the unmarried.
Sample Size
Sample size was calculated by using a single population proportion formula with the following assumption. The proportion of parent adolescent communication in previous study done in Debremarkos town of p=36.9% 9, 95% CI, 5% marginal error and 10% non-response rate and the final Sample size was 394. List of frame of students was obtained from each grade’s student roster in collaboration with instructors of respective classes. Students within the age range of 13-19 years old from the existing sampling frame (students ‘roster) were drawn. Calculated sample size was proportionally allocated for each grade according to their number of students. Simple random sampling technique was used to select the study participant.
Sample size for qualitative studies purposive sampling was employed. Parents who have adolescent students of age 13-19 years were selected for FGDs. Thirty two parents, out of whom 16 females and 16 males were involved in four focus group discussions separately where the researcher obtained saturated information. FGD participants were expected to be parents of adolescent student’s age 13-19 years. The participants were selected based on the criteria to meet the objective and research question of the study. Participants of the focus group discussions were selected after communicating with kebele administrators. The four group discussion was conducted separately for males and females parents. The discussion conducted in kebele office in different time and days.
Operational Definition
In order to have common understanding in this study the following terms and phrases are defined.
Parents
Parents in this study mean biological parents, step parents or foster parents but it does not include elder siblings
Adolescents
In this study the adolescent implies a segment of the people who are unmarried and whose age fall in the age range of between thirteen and nineteen.
Communication
Communication in this particular study refers to the exchange and sharing of knowledge, ideas, and other information concerning SRH issues among adolescents and their parents.
Communication Between Parents and AdolesCents on SRH Issues
In this particular study context parents and adolescents communication regarding SRH components is a simple discussion or talking which is interactive between parents and adolescents on the following issues: STIs/HIV/AIDS, sexual intercourse, premarital sex, condom, pubertal stage, unwanted pregnancy, contraception and menstrual cycle.
Communication on SRH Issues
Students who discussed at least two SRH issues (STIs/ HIV/AIDS, condom, sexual intercourse, premarital sex, puberty, menstrual cycle, unwanted pregnancy and contraception) with their parents in the last 12 months 7.
Study Variables
The dependent variable was parent-adolescent communication and independent variables were demographic and Socio economic variables related to parent and adolescents such as age, sex, family size, education status of mother, occupation of father, occupation of mother, living arrangement of the student, family income, educational status of father and grade level of student. Socio-cultural factors such as general communication, parent Adolescent disclosure, parent acceptance on the importance of discussion and parent time giving for discussion. Adolescent’s SRH information school and media.
Data Collection Tools and Techniques
A pre-tested, self-administered questionnaire comprised of 56 items was developed for the study. The questionnaire was initially developed in English and then translated into Afan Oromo. It was translated back to English by another person to check consistency. Most of the items were adapted from existing surveys and modified based on local context. The questionnaire incorporates 14 items on socio-demographic characteristics and 42 on communication about SRH.
Self-administered anonymous questionnaires were preferred for this kind of survey to minimize social desirability bias and interviewer distortion that often limits the use of face to face interview. Four individuals, who had completed grade twelve, were selected for data collection that has experience of data collection. Data collectors were supervised by two diploma Nurses and problems faced during data collection were solved on time. The investigator was checking filled questionnaires and solution given by discussing with the supervisors and data collectors if problems arise. Finally, filled questionnaire were signed by supervisors after checking for its completeness.
For qualitative study a series of four group discussions were carried out among purposefully selected parents who have adolescent students of age 13-19 years. Participants of the focus group discussions were selected after communicating with kebele administrators. The kebele administrators was informed on the objective of the study and then assisted in selecting those parents who have adolescents age 13-19 and who were expected to be active participants in the discussion. The investigator was the moderator, and is accompanied by BSC Nurse female assistant. The assistant is note taker and recorder as well as facilitate the female parents to increase the quality of information. There were eight participants in each group. A semi-structured questionnaire guideline was used to lead the discussion. FGD study components were present using quotes and explanations.
Data Quality Control
The quality of the data was controlled by translating the questionnaire translated by an individual fluent in both English and Afan Oromo in order to identify the clarity and consistency of the questionnaire. The questionnaire was pre-tested on 5% of the sample in a similar population in Goba town. Based on the findings necessary modifications such clarity and consistency of questions and evidence based time allocation for each respondent were made accordingly. In addition, data collectors were trained for one day on the general objective of the study and on the administration of the questionnaire. Supervision was carried out throughout the data collection period by an investigator.
The focus group discussion for mothers and fathers were conducted separately to increase the quality of information that can be generated and the confidence of the respective parents. To understand their opinion fully, a tape recorder was used after they have been told the objective of the study and verbal consent obtained.
Data Processing and Analysis
Data entering, coding and clearing were performed using Epi Data version 3.1 and the analysis was done using SPSS version 20.0. Descriptive statistics was used to describe the study population in relation to relevant variables. Binary logistic regression analysis was used to ascertain the association between explanatory and outcome variables. All variables having P value < 0.25 had significant association from binary logistic regression was entered to multiple logistic regression analysis to determine independent associated factor of adolescent parent communication on sexual and reproductive health issues by controlling the effect of possible confounder, significant statistical association was determined by using adjusted odd ratio at 95% confidence interval and P value < 0.05.
Qualitative data from FGD was transcribed by arranging the record according to forwarded questions and translated to English version. Then thematic data analysis method was used after listening audio records. Then comparison was done on the responses of different parents to identify similarities and differences. Finally, information was linked to its congruence with data obtained from quantitative findings.
Ethical Consideration
Letter of permission was obtained from Madda Walabu University Goba Referral Hospital Department of Public Health. Educational bureau and school officials were also express their willingness after they were informed of the purpose of the research. Written assent was obtained from each study participants. For those study participants who were under the age of 18 years, written consent was obtained from their parents. Participants were told the objective of the study and their right to refuse completion of the questionnaires and this would not affect any support that they will get from the schools. Questionnaires were coded instead of using names as identification and hence, confidentiality was assured throughout the study. Verbal assent was obtained from the discussants of FGD to participate and for voice recording.
Results
Socioeconomic and Demographic Characteristics of Respondents
In this study a total of 394 students were included with response rate of 100%. The mean age of respondents’ was 16.71 with standard deviation of 1.44 years. From the study participants, 212 (53.8%) were female. Majority of the respondents were 309 (78.4%) Oromo ethnic group and 178 (45.2%) were Muslims. 286 (72.5%) were living with both parents (Table 1, Table 2).
Table 1. Socio-demographic characteristics of study participants, Bale zone, Robe town June, 2017| Variables | Frequency | Percent | |
|---|---|---|---|
| Age | 13-16 years | 182 | 46.2 |
| 17-19 years | 212 | 53.8 | |
| Sex | Male | 182 | 46.2 |
| Female | 212 | 53.8 | |
| Religion | Orthodox | 174 | 44.1 |
| Muslim | 178 | 45.2 | |
| Protestant | 33 | 8.4 | |
| Others | 9 | 2.3 | |
| Ethnicity | Amhara | 64 | 16.2 |
| Oromo | 309 | 78.4 | |
| Gurage | 10 | 2.6 | |
| Tigrie | 5 | 1.3 | |
| Other | 6 | 1.5 | |
| Marital status of parents | Together | 328 | 83.2 |
| Separated | 22 | 5.6 | |
| Divorced | 28 | 7.1 | |
| Widowed | 16 | 4.1 | |
| With whom are you living | With father and mother | 286 | 72.5 |
| With mother | 45 | 11.4 | |
| With father | 11 | 2.8 | |
| Friends | 14 | 3.6 | |
| Alone | 22 | 5.6 | |
| Relatives | 16 | 4.1 | |
| Mother educational status | Illiterate | 34 | 8.6 |
| Read and write only | 87 | 22.1 | |
| Primary school | 136 | 34.5 | |
| Secondary school | 76 | 19.3 | |
| Diploma | 25 | 6.3 | |
| Degree | 31 | 7.9 | |
| No mother | 5 | 1.3 |
| Variables | Frequency | Percent | |
|---|---|---|---|
| Father educational status | Illiterate | 23 | 5.8 |
| Read and write only | 64 | 16.2 | |
| Primary school | 34 | 8.6 | |
| Secondary school | 136 | 34.5 | |
| Diploma | 24 | 6.1 | |
| Degree | 97 | 24.6 | |
| No Father | 16 | 4.1 | |
| Occupation of mother | House wife | 221 | 56.1 |
| Employed (private) | 28 | 7.1 | |
| Employed (government) | 39 | 9.9 | |
| Merchant | 77 | 19.5 | |
| Farmer | 24 | 6.1 | |
| No Mother | 5 | 1.3 | |
| Occupation of Father | Employed (private) | 28 | 7.1 |
| Employed (government) | 142 | 3.6 | |
| Merchants | 47 | 11.9 | |
| Farmer | 138 | 35 | |
| No Father | 19 | 4.8 | |
| Other | 20 | 5.1 | |
| Family size | < 5 | 243 | 61.7 |
| >=5 | 151 | 38.3 |
Source of Information on Sexual and Reproductive Health Issues
Three hundred eight (78.2%) of the respondents mentioned that they have got sexual and reproductive health information. Among thistwo hundred eighty six (92.8%) of the respondents heard information on sexual and reproductive health issues from school which is followed by mass media 91 (29.5%) (Figure 1).
Figure 1. Students’ source of information about sexual and reproductive matters, Bale zone, Robe town June, 2017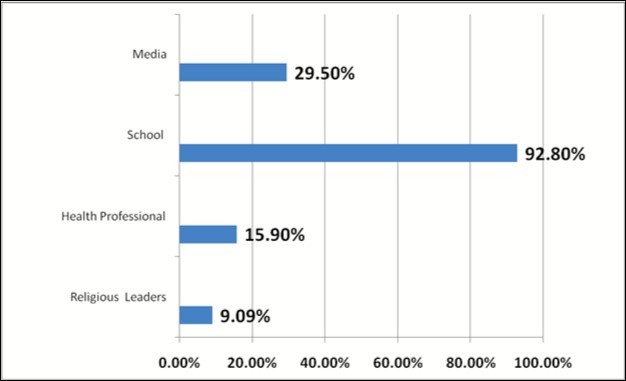
Communication on Sexual and Reproductive Health Issues
Three hundred seventy four (94.9%) of the students had agreed on the importance of discussion on sexual and reproductive health matters with their family. It was also supported by majority of participants who involved in focus group discussion as communication between parent and adolescent on sexual and reproductive health matters since parents needs to play vital role in shaping their children behavior during adolescent age particularly regarding premarital sex and unwanted pregnancy but they have a gap of knowledge regarding sexual health.
This is evident from the response, “We are supposed to tell our adolescents everything that has to do so with reproductive health. But I do not feel that we know all information they need,” (a 38-year-old female discussant).
However, 186(47.2%) of students had ever discussed on at least two sexual and reproductive health topics with their parents. Large number of the study participants 228(57.9%) had reported as they have discussed on condom from which 223(56.6%) of them undertaken the discussion with their friends/peers. Majority of them 89% discussed some times.
The majority of the students discussed on different sexual and reproductive health matters with their peers/friends followed by with sisters. From the total female participants, majority of them has seen their first menses at the age of fourteen years which account for 17.8% followed by fifteen years of age (15.7%). About 20(9.4%) of study participants had discussion before they have seen their first menses. Nearly 65% of them had a discussion with their sisters about menses before they have seen it followed by with peers (45%) (Table 3).
Communication on Contraceptive
One hundred nine (27.7%) of the students haddiscussed about contraceptive (Table 3). On the other hand 285 (72.3%) did not discuss contraceptive with their parents were shameful and parent’s lack of communication skill 254 (64.5%) and 237 (60.2%) respectively (Table 4). However, these respondents had discussed with their mothers 64 (16.2%) and 61 (15.5%) with friends (Table 3). Majority, 80.7% discussed sometimes. Lack of knowledge regarding sexual and reproductive health matters as well as social norms attached to dealing with such kind of issues were mentioned by majority of focus group discussion participants as a reason for not discussing sexuality with children.
Table 3. Study participants’ level of discussion and with whom they had discussed in different sexual and reproductive health issues, Robe town, June 2017.| Topic of discussion | With whom they had discussed | ||||||
| Discussed | *Father | *Mother | *Peers | *Sisters | *Brothers | *Other | |
| Contraceptive | 109(27.7) | 30(7.6) | 64(16.2) | 61(15.5) | 48(12.2) | 30(7.6) | 2(0.5) |
| STI/HIV/AIDS | 131(33.2) | 24(6.1) | 38(9.6) | 109(27.7) | 47(11.9) | 34(8.6) | 16(4.2) |
| Sexual intercourse | 103(26.1) | 21(5.3) | 38(9.6) | 81(20.6) | 42(10.7) | 26(6.6) | 1(0.3) |
| Unwanted pregnancy | 119(30.2) | 6(1.5) | 36(9.1) | 96(24.4) | 62(15.7) | 9(2.3) | 2(0.6) |
| Premarital sex | 113(28.7) | 13(3.3) | 41(10.4) | 91(23.1) | 42(10.7) | 14(3.6) | 1(0.3) |
| Condom | 228(57.9) | 2(0.5) | 4(1.0) | 223(56.6) | 41(10.4) | 27(6.9) | 14(3.6) |
| Pubertal stage | 112(28.4) | 9(2.3) | 17(4.3) | 85(21.6) | 60(15.2) | 12(3.0) | 7(1.8) |
| Menstrual cycle | 115(29.2) | 3(0.8%) | 48(12.2) | 74(18.8) | 52(13.2) | 2(0.5) | 0(0) |
| Topic of discussion | Reasons for not discussing about SRH | ||||||
| Not discussed | *Culturally unacceptable | *Shame | *Parent’s lack of knowledge on SRH | *Parent’s lack of communication skill | *Parents are not a good listener | *Difficult and embarrassing | |
| Contraceptive | 285(72.3) | 182(46.2) | 254(64.5) | 198(50.3) | 237(60.2) | 136(34.5) | 169(42.9) |
| STI/HIV/AIDS | 263(66.8) | 166(42.1) | 233(59.1) | 187(47.5) | 227(57.6) | 137(34.8) | 171(43.4) |
| Sexual intercourse | 291(73.9) | 181(45.9) | 261(66.2) | 213(54.1) | 252(64.0) | 143(36.3) | 188(47.7) |
| Unwanted pregnancy | 275(69.8) | 174(44.2) | 245(62.2) | 202(51.3) | 222(56.3) | 145(36.8) | 176(44.7) |
| Premarital sex | 281(71.3) | 169(42.9) | 250(63.5) | 192(48.7) | 239(60.7) | 138(35.0) | 172(43.7) |
| Condom | 166(42.1) | 126(32.0) | 136(34.5) | 124(31.5) | 109(27.7) | 96(24.4) | 123(31.2) |
| Pubertal stage | 282(71.6) | 175(44.4) | 241(61.2) | 197(50.0) | 223(56.6) | 140(35.5) | 180(45.7) |
| Menstrual cycle | 97(24.6) | 78(19.8) | 97(24.6) | 80(20.3) | 96(24.4) | 60(15.2) | 65(16.5) |
Communication on STI/HIV/AIDs
One hundred thirty one (33.2%) of the students haddiscussed about STI/HIV/AIDs. From those had a discussion, 109 (27.7%) and 47 (11.9%) discussed with their peers and sisters respectively (Table 3). Majority, 77.9% discussed sometimes. On the other hand 263 (66.8%) did not discussed with their parents due to shame and parent’s lack of communication skills which account 233 (59.1%) and 227 (57.6%) respectively (Table 4). From qualitative data, nearly half of the focus group discussants mentioned as they do not discuss about STI/HIV/AIDs due to lack of knowledge regarding sexual and reproductive health issues.
Communication on Sexual Intercourse
One hundred three (26.1%) of the students discussed about sexual intercourse (Table 3). Majority, 72.8% discussed sometimes. On the other hand 291 (73.9%) did not discuss sexual intercourse with their parents were shameful and parent’s lack of communication skills 261 (66.2%) and 252 (64.0%) respectively (Table 4). However, these respondents had discussed with their peers 81 (20.6%) and 42 (10.7%) with sisters (Table 4).
From focus group discussion, a female participant said that, “it less likely to discuss about sexuality in the house and in the community as well which basically related with cultural unacceptability and religious matters”a 35 years old female participant.
Communication on Unwanted Pregnancy
One hundred nineteen (30.2%) of the students had discussed about unwanted pregnancy (Table 3). Majority, 75.6 % discussed sometimes. On the other hand 275 (69.8%) did not discuss unwanted pregnancy with their parents were shameful and parent’s lack of communication skill 245 (62.2%) and 222 (56.3%) respectively (Table 4). However, these respondents had discussed with their peers 96 (24.4%) and 62 (15.7%) with sisters (Table 3).
Communication on Premarital Sex
One hundred thirteen (28.7%) of the students had discussed about premarital sex (Table 3). Majority, 61.1% discussed sometimes. On the other hand 281 (71.3%) did not discuss premarital sex with their parents were shameful and parent’s lack of communication skill 250 (63.5%) and 239 (60.7%) respectively (Table 4). However, these respondents had discussed with their peers 91 (23.1%) and 42 (10.7%) with sisters (Table 3).
One 50 years old male parent said “keep their virginity until marriage almost all of the discussants agreed on a virgin girl in our community is respected ” (50 years old male FGD participant).
Communication on Condom
Two hundred twenty eight (57.9%) of the students had discussed about condom (Table 3). Majority, 89 % discussed sometimes. On the other hand 166 (42.1%) did not discuss with their parents were shameful and culturally unacceptable 136 (34.5%) and 126 (32.0%) respectively (Table 4). However, these respondents had discussed with their peers 223 (56.6%) and 41 (10.4%) with sisters (Table 4).None of parents discussed about condom use.
One mother said that “discussing about condom is opening the way or initiating our children to have sex” (32 years old female FGD participant).
Communication on Puberty
One hundred twelve (28.4%) of the students had discussed about puberty (Table 3). Majority, 67.9 % discussed sometimes. On the other hand 282 (71.6%) did not discuss with their parents were shameful and parent’s lack of communication skill 241 (61.2%) and 223 (56.6%) respectively (Table 4). However, these respondents had discussed with their peers 85 (21.6%) and 60 (15.2%) with sisters (Table 3).
Communication on Menstrual Cycle
One hundred fifteen (29.2%) of the students had discussed about menstrual cycle (Table 3). Majority, 53% discussed sometimes. On the other hand 97 (24.6%) did not discuss with their parents were shameful and parent’s lack of communication skill 97 (24.6%) and 96(24.4%) respectively (Table 4). However, these respondents had discussed with their peers 74 (18.8%) and 52 (13.2%) with sisters (Table 4).
In this case one female participants of focus group discussion mention “I frequently discuss with my child regarding menses with the purpose of developing her confidence since the issue is naturally occurs on human being” 34 years female FGD participants. But majority of participants did not discussed on menses as a result of discomfort and shame of dealing with children.
With regard to adolescents major reasons for not discussing sexual and reproductive matters with their family, about 261 (66.2%) of students reported as shameful hindered them for discussing about sexual intercourse followed by parent’s lack of communication skill which account for 252 (64.0%). In general, being ashamed, parent’s lack of communication skill and lack of parents’ knowledge about sexual and reproductive health issues were the major reasons mentioned by the students for not discussing about sexual and reproductive health matters with their parents. The reason not discussing RH issues is bound by several socio cultural norms and expectations: “In our culture discussing about sexual issues is very rare. Let alone discussing with your child, wife-husband discussion on this issue is not experienced. Everybody is shy about it. These culture, taboo and traditions are passing from generation to generation. We were brought up like this and are doing it today,” (45-year-old female parent).
Bivariate logistic regression analysis was performed to assess association between each independent variable and outcome variable. Results of bivariate analysis showed that grade level, sex of student, mother occupation, mother education status, father education status, living arrangement and family size become significantly associated with parent adolescent communication.
Multivariate analysis was performed to identify factors independently associated with parent adolescent communication. In the multivariate analysis those variables with a p value <0.25 in the bivariate analysis were included and backward stepwise model was used. In the multivariate analysis, and the Hosmer- Lemeshow test indicates a p > 0.05 which signifies that the overall model fit is good. From 11 variable entered in to the multivariate analysis four of the variable including sex of student being female, being student grade 11, student from father education status diploma and above and students living with relative/friend or living alone were significantly associated with parent adolescent communication after controlling for confounders (Table 5).
Table 5. Factors associated with student-parent communication about sexual and reproductive matters, Bale zone, Robe town, June 2017.| Variables | Communication on SRH | Crude OR (95%CI) | AOR(95%CI) | ||
| Yes | No | ||||
| Sex | MaleFemale | 63123 | 11989 | 12.61(1.73, 3.93)** | 12.02 (1.25, 3.26)* |
| Grade | 9th10th11th12th | 65872113 | 10280917 | 11.71 (1.10, 2.64)3.66 (1.58, 8.49) **1.20 (0.55, 2.63) | 11.16 (0.70, 1.92)4.88 (1.76, 3.54)*0.65 (0.28, 1.50 |
| Living arrangement | With both parentsWith single parentWith friends/ relatives or alone | 1581810 | 1314037 | 10.37 (0.20, 0.68) 0.22 (0.11, 0.47)** | 10.84 (0.35. 2.01)0.32 (0.12, 0.80* |
| Mother education | IlliteratePrimary schoolDiploma and aboveNo mother | 3968772 | 8759593 | 12.57 (1.54, 4.29) **2.91 (1.75, 4.84)1.49 (0.24, 9.26) | |
| Fathers education | IlliteratePrimary schoolDiploma and aboveNo father | 219151 5 | 702110611 | 11.13 (0.46, 2.80)4.48 (2.58, 7.76)**1.43 (0.44, 4.58) | 10.74 (0.26, 2.01)3.35 (1.73, 6.47)**2.47 (0.44,13.72) |
| Mother occupation | HousewifeEmployed (Gov`t or private)MerchantOther1 | 11034384 | 120293920 | 11.28 (0.73, 2.240)1.06 (0.63, 1.78)0.22 (0.072, 0.66)** | |
| Family size | <5>=5 | 85101 | 15850 | 13.75 (2.44, 5.77)* | |
Accordingly, students whose father education diploma and above were 3.35 times more likely to have parent adolescent communication than students whose father were illiterate (AOR, 3.35 95% CI (1.73, 6.47)). It was also found that, grade 11th students were 4.88 times more likely discussed on sexual and reproductive health matters with their parent compared with grade 9th students (AOR: 4.88 95%CI: (1.76, 13.54)).
In this study, female study participants were nearly 2 times more likely to discussed about sexual and reproductive health matters with their parents when compared with their counterparts (AOR: 2.02 95%CI: (1.25, 3.26)). Again the odd of parent adolescent communication Study participants whose living arrangement were with relatives were less likely discussed on sexual and reproductive matters when compared with those students living with both parents ((AOR: 0.32 95%CI: (0.12, 0.80)).
However, factors that were statistically significantly in the bivariate analysis like mother education, mother occupation and family size were not showed statistically significant association in the multivariate analysis after controlling for confounders
Discussion
Parents play an essential role in the betterment of adolescents' lives through communicating various issues particularly sexual and reproductive health matters. They have a unique role in influencing the decisions and behaviors of their adolescent children related to sexual and reproductive health issues based on their willingness to communicate on such topics.
This study has tried to assess level of parent-adolescent communication on sexual and reproductive health issues and factors associated with it. Accordingly, about 186 (47.2%) of the students has discussed on two and more sexual and reproductive topic with their parents.
The result is lower when seen with the finding of the research conducted on barriers of parent-adolescent communication on sexual and reproductive health issues among school students in Yirgalem town which showed 59% parent-adolescent discussion on sexual and reproductive health issues 8. This could be due to socioeconomic and demographic difference among the two study areas.
It is higher when compared with a longitudinal study in Tanzania that showed 27% of parent-adolescent communication about sexual and reproductive health 9 and a study done in Rwanda which revealed, only 19% of the study participants had discussed on sexual and reproductive health matters 10. The result also higher than studies done in Ethiopia in Nekemte town which showed that, about a third of young people (32.4% of females and 32.7% males) engaged in conversation about sexual and reproductive health topics with their parents/parent during the last six months 11 and it is also higher when compared with a study conducted Debremarkos town 7 and Dire Dawa town 12 which showed that 36.9% and 36.8% of students discussed in at least two topics of SRH respectively. The result of this study was also slightly higher when compared to a recent study done in Boditi town Southern Ethiopia where 40.70% of students had discussed at least two topics of RH issues with either of their parents 13. The possible reason for the difference could be time gaps between the studies and the current better expansion of sexual and reproductive health service for adolescents.
With regard to with whom the student had discussed sexual and reproductive health matters, majority of study participants had undertaken the discussion with peers followed by with sisters. It is in line with the study done on barriers of parent-adolescent communication on sexual and reproductive health issues among school students in Yirgalem town which showed that, students more likely preferred to communicate sister and peers 8 and a study conducted in Benishangul Gumz region which indicated, a high proportion of both male (78%) and female (72%) students preferred to discuss sexual and reproductive health issues with peers compared with parents 14. The possible explanation might be peers are the most preferred to discuss on reproductive health issues by students. As to reported reason for not discussing about sexual and reproductive health issues, being ashamed, parent’s lack of communication skill and lack of parental knowledge on SRH were the major perceived reasons mentioned by the students.
In multivariate analysis, level of father education showed strong statistical association with communication about sexual and reproductive health. Adolescents whose father’s education diploma and above were 3.35 times more likely to have parent adolescent communication than students whose fathers were illiterate. This is congruent with previous finding from study done in Rwanda 10. This is congruent with previous finding in Dire Dawa town, Western Ethiopia, in Alamata, Tigray Region and Yirgalem town 8, 12, 14, 15. The possible explanations might be educated fathers have better access to health service information, improved perceptions of SRH issue.
It was also found that, grade level of students to be statistically linked with parent-adolescents communication. Grade 11th students were 4.88 times more likely discussed on sexual and reproductive matters with their parent compared with grade 9th students. This finding was similar with the study done in Western Ethiopia and Debremarkos 7, 11. This could be attributed to maturity which comes when their education level increases. In contrary to evidence from a study done in Mekelle town and in Alamata High school, northern Ethiopia 15, 16 which showed that students whose grade 11th and 12th were less likely to discuss sexual and reproductive matter when compared to grade nine students. The difference might be in the study area parents give emphasis to discuss sexual and reproductive issues when they are at lower grade level.
Sex of the study participants was found to be statistically associated with parent- adolescent communication on sexual and reproductive health matters. Female study participants were nearly 2 times more likely to discussed about sexual and reproductive health matters with their parents when compared with their counterparts. The result of this study was comparable when compared with the study done in Rwanda where males did not discuss sexual matters compared to the female students 10, 17, 18. This finding was also in line with the study done in Ethiopia Dire Dawa town where Male were by 40% less likely to discuss on sexual issues with their parent than female 12.
In contrary to this study done Benishangul Gumuz revealed that male were more likely to communicate on parent adolescent communication 12. In addition to this a study conducted on aim to determine young people’s parental discussion about SRH issues in Awabel woreda, Northwest Ethiopia where parental discussion SRH issues were significantly associated and higher among young males 19. This difference might be due to differences in the study population, study settings, data collection method and the study design itself both of the above mentioned studies were conducted among rural residents.
In this study, with whom student live was found to be significantly associated with parent-adolescents communication on sexual and reproductive matters. Study participants whose living arrangement were with relatives or friend or students who live alone were less likely discussed on sexual and reproductive matters when compared with those students living with both parents. The finding is in line with a research done on parent-adolescent communication about sexual and reproductive health in Mekele town where students living with both parents were two times to communicate on SRH issue when compared with students living with others 15. This might be due to students who are living with both parents could have a probability of discussion with father or mother.
However, this finding was not supported by a study done in Awabel woreda, Northwest Ethiopia as young people who were living with their fathers were more likely to discuss on SRH topics 19. The difference might be due to the educational status difference between the two communities and study setting as well as the study population difference since this study conducted among young people and at community level.
However, factors that were statistically significantly in another study like age of student, mother education and family size were not showed statistically significant association in the present study. The reason might be there is no difference on parent adolescent communication with respect to age of student, mother education status and family size in the present study area.
Strength and Limitation Of The Study
Strength of the Study
The study used mixed method of quantitative and qualitative method which allowed triangulation of the findings of the study.
Limitations of the Study
As this is a cross-sectional study does not show cause and effect relationship. There might be also be a recall bias in remembering issue of discussion between parents and adolescent in 12 months.
Conclusion
The study revealed that low level of parent-adolescent communication on sexual and reproductive health matters. From sexual and reproductive health topics discussed, discussion on condom was the leading one. Among those students had a discussion on sexual and reproductive health matters with their parents, majority of them had the discussion with peers followed by sisters
Being ashamed, parent’s lack of communication skill and Lack of parental knowledge about sexual and reproductive health, were the major reasons mentioned by the students for not discussing about sexual and reproductive health matters with their parents. Sex, educational level of students, living arrangement of students and father educational level were identified as significantly associated with parent-adolescent communication on sexual and reproductive health matters. Hence provision of information, education and communication targeting adolescents and their parents to increase their awareness and practice regarding sexual and reproductive health matters is recommended.
Authors’ Contribution
TF have conceived and designed the study, performed the data analysis and write up of the final result. AT participated in designing the study, performed the statistical analysis, writhing the results and discussion and prepared the manuscript. MT has assisted in designing the study writing the results and discussion.
Acknowledgements
We would like to present my heartfelt thanks to Robe Town Administration, Health Office, Educational Office, and Robe Town Secondary and Preparatory Schools. We would like to thank the study participants and data collectors for their time and information they provided.
Last but not least, I would also like to extend my thanks to Madda Walabu University, Goba Referral Hospital, and Department of Public Health for providing me the opportunity to carry out the research.