Abstract
HIV/AIDS has become a global scourge affecting mainly young people. Sexual behavior change remains the most effective way of preventing further spread. The aim of this study is to assess the knowledge, perception and practice of safe lifestyles towards prevention of HIV infection among students of a tertiary educational institution in Abakaliki, south eastern, Nigeria. A cross sectional descriptive study was carried out, and participants were selected using multistage sampling technique. Data was collected using a pretested, self administered questionnaire and analyzed using SPSS software, version 20. Three hundred and eighty seven participants were recruited for the study, including 199 (51.4%) males and 188 (48.6%) females. Mean age of participants was 23.6 ±2years. All (100%) of the participants were aware of the existence of HIV/AIDS, with the commonest source of information being electronic media (81.1%). Their knowledge of the routes of transmission and modes of prevention of HIV infection was high, though few of them have some misconceptions. Poor practice of safe lifestyles towards prevention of HIV infection as well as low perception of self-vulnerability to the risk of HIV infection was also found. There was poor practice of preventive lifestyles among the participants despite high knowledge of HIV transmission and preventive measures probably due to low perception of self-vulnerability to the risk of HIV infection. Health education should be intensified to impact sufficient comprehensive knowledge to change low perception of self-vulnerability among the students.
Author Contributions
Academic Editor: Christophe Marchand, Staff Scientist Laboratory of Molecular Pharmacology Center for Cancer Research National Cancer Institute Bethesda, US.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 Ngozi Immaculata UGWU, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
HIV/AIDS is a major public health problem. Globally, almost 75 million people have been infected with the HIV virus and about 36 million people have died of HIV since it was first recognized in 1981, making it one of the most destructive pandemics in recorded history.1 An estimated 0.8% of adults aged 15 – 49 years worldwide are living with HIV, although the burden of the epidemic continues to vary considerably between countries and regions. Sub-Saharan Africa remains most severely affected, with nearly 1 in every 20 adults living with HIV and accounting for 71% of the people living with HIV worldwide.1
In 1981, the first set of cases of AIDS was discovered among homosexual men in the United States.2 The men had an unusual type of pneumonia called Pneumocystis carinii pneumonia and rare skin tumors called Kaposi’s sarcoma. Shortly thereafter, the disease was recognized in Western Europe and Africa.2Today it has become a global pandemic.
Since its emergence, HIV/AIDS has become a devastating challenge to human dignity and generalized threat to socioeconomic growth,3, 4 It has hindered the achievement of Millennium Development Goals,5 reduced life expectancy,6 lessened labour productivity and increased poverty levels particularly in developing countries.7
HIV is transmitted by three main routes, which are: unprotected sexual intercourse (anal or vaginal), transfusion of contaminated blood or blood products and vertical (mother-to-child) transmission during pregnancy, childbirth and breastfeeding. HIV transmission in Nigeria is largely through unprotected heterosexual sex contributing 80% of transmission.8 Factors that encourage transmission include lack of information about sexual health and HIV, multiple sexual partners, prostitution, low levels of condom use and high levels of sexually transmitted diseases.9 Preventing HIV transmission and its attendant socio-economic sequel is an essential part of addressing the global HIV/AIDS pandemic. It has been documented that sexual behavior change and practice of safe lifestyles is the most effective way of preventing further HIV transmission.8
Although several studies have documented high level of knowledge of, perception and practices towards HIV/AIDS,10, 11 more information is needed about the knowledge of and practice of lifestyle preventive measures and its linkage with perception of vulnerability, especially among students of tertiary institutions. Hence the main objective of this study is to evaluate the level of knowledge of HIV transmission and prevention, perception and practice of safe lifestyles towards prevention of HIV infection among students of a tertiary educational institution. The information obtained may portray the need to refocus education program so as to impact sufficient comprehensive knowledge to change perception of self-vulnerability, and encourage practice of safe lifestyle to prevent further HIV transmission.
Materials and Methods
Study Design
Descriptive cross-sectional study was carried out between June and September 2013 at Ebonyi State University, which is located in Abakaliki, Ebonyi State, south eastern Nigeria.
Sample Size
The sample size for this study was determined using the formula12 for estimation of population prevalence and was based on a 95% confidence level, and a prevalence of knowledge gap about HIV/AIDS among undergraduates, which is 53%, as reported by a previous study,13 and a desirable degree of accuracy set at 0.05 level. Minimum sample size of 383 was calculated. However, 425 questionnaires were given out to account for refusals. Out of this number, 387 were correctly and completely filled. These questionnaires were considered valid and were used for data analysis.
Sampling Method
Multistage sampling technique was used for the study. Simple random sampling by ballot method was used to select three out of the eleven faculties existing in the school. Simple random sampling technique by ballot method was also employed to select three departments, one department each out of the three chosen faculties, as well as to select students from the chosen departments.
Study Instrument and Data Collection
The tool for data collection was a pre-tested, semi-structured self-administered questionnaire. Information sought in the questionnaire included socio-demographic characteristics, knowledge about HIV including modes of transmission and methods of prevention, perception of self-vulnerability to HIV infection and practice of preventive lifestyles. During data collection, three research assistants were employed to administer the questionnaires. They were adequately trained and mobilized for the exercise and they assisted in the administration and retrieval of the questionnaires.
Data Management and Analysis
KnowledgeaboutHIV: Twenty eight variables on the study instrument were used to assess participants’ knowledge about HIV including routes of transmission and ways of prevention. One mark was awarded for every correctly answered question and zero for every wrongly answered or unanswered question. Getting all the twenty eight questions on general knowledge of HIV/AIDS correctly were scored as 100%. Participants who scored 75% and above were categorized as having very good knowledge. Those who scored between 50% and 74.9% were categorized as having good knowledge; those who scored between 25% and 49.9% were categorized as having poor knowledge while those who scored below 25% were categorized as having very poor knowledge.
Practice: Five questions on the study instrument were used to asses participants’ practice of preventive measures towards HIV infection and these practices were represented in proportions.
Data was cleaned for inconsistencies in the responses and was entered into a computer using statistical package for social sciences (SPSS) software, version 20, which was also used for the analysis. Descriptive statistics were used to compute percentages and averages. Chi square test was used to assess the relationship between variables. Results were presented in tables and charts, and expressed as percentages/proportions, means and standard deviation.
Ethical Issues
The study procedure was approved by joint Ethics Committee of Federal Teaching Hospital Abakaliki and the Management of Ebonyi State University, Abakaliki. Questionnaires were administered only to students who gave their consent.
Results
A total of 387 participants were surveyed and were made up of 199 (51.4%) males and 188 (48.6%) females with male to female ratio of 1.1:1 The ages of the participants ranged between 19 and 35years with mean age of 23.6±2years. All (100%) the participants were Christians, with most, 374 (96.6%) of them single while 13 (3.4%) were married (Table 1).
Table 1. Socio-demographic characteristics of the participants| Characteristics | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Males | 199 | 51.4 |
| Females | 188 | 48.6 |
| Total | 387 | 100 |
| Age | ||
| 19 - 24 | 265 | 68 |
| 25 - 30 | 116 | 30 |
| 31 - 35 | 6 | 2 |
| Total | 387 | 100 |
| Marital status | ||
| Married | 13 | 3.4 |
| Single | 374 | 96.6 |
| Total | 387 | 100 |
| Religion | ||
| Christianity | 387 | 100 |
| Islam | 0 | 0 |
| Traditional | 0 | 0 |
| Others | 0 | 0 |
| Total | 387 | 100 |
Knowledge about HIV
All the participants (100%) had knowledge of the existence of HIV/AIDS. Electronic media (radio/television) was the most frequent source of information about HIV/AIDS among the participants as indicated by 314(81.1%). Other sources of information include health workers 180(46.5%), friends and colleagues 156(40.3%), Lectures 126(32.6%), Posters and pamphlets 124(32%), Newspapers 119(30.7%), internet 111(28.7%), family members 106(27.4%), and libraries 45(11.6%) (Figure 1).
Figure 1. Sources of information/ awareness of HIV/AIDS
Table 2 shows the participants’ knowledge of the routes of transmission of HIV. Three hundred and eighty three (99%) of the participants know that HIV can be transmitted by having sexual intercourse with an infected person. Other routes of HIV transmission known by the participants include transfusion of infected blood 378(97.7%), transmission of mother to baby during pregnancy 250(64.6%) or breast-feeding 269(69.5%) and sharing of unsterilized sharp objects 358(92.5%). However, there were misconceptions about routes of transmission such as sharing toilet with infected person 26(6.7%), sharing the same bed with an infected person 6(1.6%), mosquito bite 5(1.3%), hand shake 4(1%) and eating with infected person 1(0.3%).
Table 2. participants’ knowledge of routes of HIV transmission| Route of transmission | Yes (%) | No (%) |
|---|---|---|
| Sexual intercourse with infected person | 383 (99.0) | 4 (1) |
| Transfusion of infected blood | 378 (97.7) | 9 (2.3) |
| Sharing of unsterilized sharp objects | 358 (92.5%) | 29 (7.5) |
| Mother to child during breastfeeding | 269 (69.5) | 118 (30.5) |
| Mother to child during pregnancy | 250 (64.6) | 137 (35.4) |
| Sharing toilet with infected person | 26 (6.7) | 361 (93.3) |
| Sharing the same bed with infected person | 6 (1.6) | 381 (98.4) |
| Mosquito and other insect bite | 5 (1.3) | 382 (98.7) |
| Hand shake | 4 (1) | 383 (99) |
| Eating with infected person | 1 (0.3) | 386 (99.7) |
Table 3 shows participants’ knowledge of preventive measures against HIV/AIDS. Abstinence from sex 377(97.4%), sticking to one uninfected partner 355(86.6%), not sharing sharp objects 374(96.6%) and use of condoms 366(94.6%) were the commonly known preventive measures. There was, however, misconceptions among some of the participants that isolation of infected persons from others 95(24.6%) and use of insecticide 9(2.3%) are preventive measures.
Table 3. participants’ knowledge of preventive measures towards HIV infection| Preventive measures against HIV infection | Yes (%) | No (%) |
|---|---|---|
| Abstaining from sex | 377 (97.4) | 10 (2.6) |
| Not sharing sharp objects | 374 (96.6) | 13 (3.4) |
| Use of condom | 366 (94.6) | 21 (5.4%) |
| Sticking to one uninfected partner | 335 (86.6) | 52 (13.4) |
| Isolation of infected person from others | 95 (24.5) | 292 (75.5) |
| Use of insecticides | 9 (2.3) | 378 (97.7) |
Eighty nine percent (345) believed that they cannot tell whether a person has HIV by mere looking at him or her while 10.9% (42) believed otherwise.
Ninety one percent (353) believed that a person can be infected without even knowing it while 8.8% (34) had contrary belief.
Seventy seven percent (298) of the participants believe that HIV/AIDS is not curable, 18.3% (71) believe that it is curable while 4.7% (18) did not know whether it is curable or not.
Most of the participants 379 (97.9%) reported that HIV is preventable while eight (2.1%) reported that HIV is not preventable.
Many of the participants 218(56.3%) perceived that they are not vulnerable to HIV infection, 156(40.3%) believe that they are vulnerable and 13(3.4%) did not know whether they are vulnerable or not (Figure 2).
Figure 2. distribution of participants according to perceived self-vulnerability to HIV infection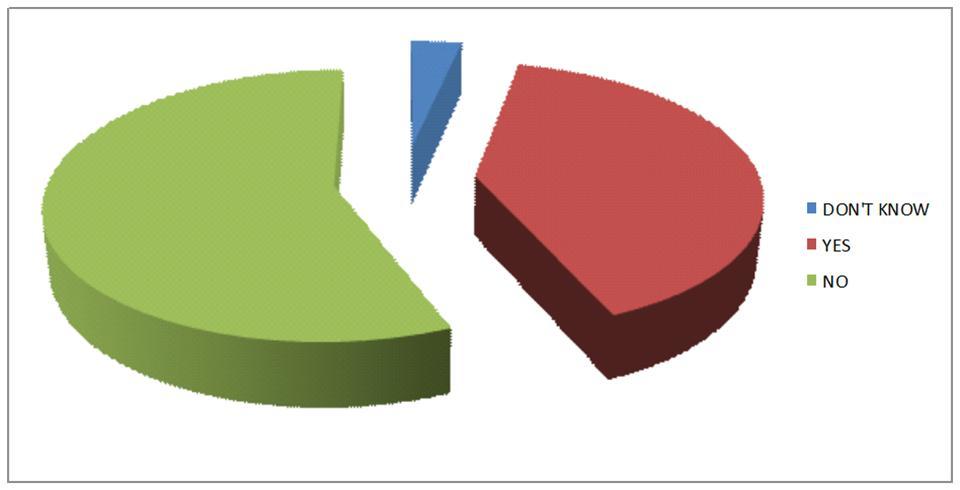
Practice of Safe Lifestyles Towards HIV Prevention.
Preventive lifestyles practiced by the participants include abstinence from sex 211(54.5%), having only one partner 166(42.9%), always using condom during sexual intercourse 116(30%), not sharing sharp objects with people 212(54.7%). Out of the thirteen students that were married, 9(69.2%) reported not engaging in extra marital sex (Table 4).
Table 4. preventive life styles practiced by the participants| Preventive lifestyles | Frequency | Percentage |
|---|---|---|
| Abstain from pre-marital sex | 211 | 54.5 |
| Do not share sharp objects | 212 | 54.7 |
| Have only one partner | 166 | 42.9 |
| Always use condom | 116 | 30.0 |
| Do not engage in extramarital sex | 9 | 69.2 |
Knowledge and Gender
This study found that both males and females have adequate knowledge about routes of HIV transmission. One hundred and ninety three (97%) males and 184 (97.9%) females have very good knowledge about HIV transmission. Association between knowledge of HIV transmission and gender was not statistically significant (X2 = 0.30, p = 0.58).
Males and females were also found to have adequate knowledge about ways of preventing HIV infection. One hundred and eighty nine (95%) males and 184 (97.9%) females have very good knowledge of preventive measures towards HIV infection. Association between knowledge of HIV preventive measures and gender was not statistically significant (X2 = 2.32; p = 0.13).
Practice of Safe Lifestyle and Gender
This study showed that 104 (55.3%) females and 107 (53.8%) males practice abstinence. More females practice abstinence than males though not statistically significant (X2 = 0.094; p = 0.760).
More males, 91 (45.7%) have only one sexual partner than females, 75 (39.9%), though not statistically significant (X2 = 1.334; p = 0.246).
Seventy (35.2%) males and 46 (24.5%) females use condom during sexual intercourse. Association between gender and condom use during sexual intercourse was statistically significant (X2 = 5.281; p = 0.02).
Practice of Safe Lifestyle and Perception of Self-Vulnerability
Table 5 revealed that perception of self-vulnerability generally has significant statistical relationship with safe sex practices, (p < 0.05). Out of the 231 participants who had low perception of their vulnerability to HIV infection, 141 (61%) still engage in pre-marital sex; 144 (62.3%) have multiple sexual partners while 162 (70%) do not use condom during sexual intercourse. Conversely, 86 (55.1%) out of 156 participants who had high perception of self-vulnerability to HIV infection abstain from pre-marital sex. Seventy nine (50.6%) of them had only one sexual partner and majority (61.5%), use condom during sexual intercourse.
Table 5. Relationship between safe sex practices and perception of self-vulnerability| Perception of self-vulnerability | d.f | |||
| Safe sex practices | Low N (%) | High N (%) | X 2 (p-value) | |
| Abstinence from pre-marital sex | ||||
| Yes | 90 (39.0) | 86 (55.1) | 1 | 9.8 (0.002) |
| No | 141 (61.0) | 70 (44.9) | ||
| Total | 231 (100) | 156 (100) | ||
| Only one sex partners | ||||
| Yes | 87 (37.7) | 79 (50.6) | 1 | 6.7 (0.012) |
| No | 144 (62.3) | 77 (49.4) | ||
| Total | 231 (100) | 156 (100) | ||
| Condom use | ||||
| Yes | 69 (30.0) | 96 (61.5) | 1 | 8.9 (0.003) |
| No | 162 (70.0) | 60 (38.5) | ||
| Total | 231 (100) | 156 (100) | ||
Knowledge about HIV/AIDS and Perception of Self-Vulnerability
Table 6 shows that despite the low perception of self-vulnerability to the risk of HIV infection among the 231 participants, they were all very knowledgeable on issues concerning HIV. Similarly, 154 (98.7%) out of 156 participants who high perception of self-vulnerability also had very good knowledge of HIV.
Table 6. Relationship between perception of self-vulnerability and knowledge of HIV/AIDS| Knowledge of HIV/AIDS prevention | |||||
| Perception of self-vulnerability | Good knowledge | Very good knowledge | Total | d.f | X 2 (p-value) |
| Low N (%) | 0 (0) | 231 (100) | 231 (100) | 1 | 2.97 (0.08) |
| High N (%) | 2 (1.3) | 154 (98.7) | 156 (100) | ||
Knowledge about HIV/AIDS and Practice of Safe Lifestyle
Table 7 shows that majority of the participants engage in risky sexual behaviors despite high knowledge about HIV.
Table 7. Relationship between general knowledge of HIV/AIDS and safe sex practices| General knowledge of HIV/AIDS | |||||
| Safe sex practices | Good N (%) | Very good N (%) | Total (100) | d.f | X 2 (p-value) Fishers exact test |
| Abstinence from pre-marital sex | |||||
| No | 2 (1.1) | 174 (98.9) | 179 | 1 | 2.4 (0.21) |
| Yes | 0 (0) | 211 (100) | 211 | ||
| Only one sex partners | |||||
| No | 2 (0.9) | 219 (99.1) | 221 | 1 | 1.5 (0.33) |
| Yes | 0 (0) | 155 (100) | 166 | ||
| Condom use | |||||
| No | 2 (0.7) | 269 (99.3) | 271 | 1 | 0.86 (0.49) |
| Yes | 0 (0) | 116 (100) | |||
| Sharing of sharp objects | |||||
| No | 0 (0) | 176 (100) | 176 | 1 | 1.67 (0.29.) |
| Yes | 2 (0.5) | 209 (100) | 211 | ||
Discussion
This study revealed that the students were between the ages of 19 to 35 years with equal sex distribution. The age of the students were within the most vulnerable age group for HIV epidemic, with most of them unmarried, making them ideal for the study of knowledge on issues regarding HIV/AIDS. This age group, the most economically productive age group in the society, has been most implicated in other studies within and outside Nigeria.13, 14
The study also revealed that all the students had heard about HIV/AIDS. This is similar to the findings of the studies conducted by Unadike et al15 and Onah et al16 who also reported awareness of HIV/AIDS among all the university students studied. Radio and television were found to rank highest as the source of information on HIV/AIDS. This corroborates with previous study conducted by Makwe et al,17 who also reported radio and television as the main source of awareness and other information about HIV/AIDS. This is important in view of the fact that mass media can reach most people in Nigeria, and so there is need for more media-driven health education campaigns.
Most of the participants were found to have very high level of knowledge about the various routes of HIV transmission, however, few of the participants had some misconceptions. They reported that sharing toilet with an infected person, mosquito and other insect bite, sharing the same bed with an infected person, handshake and eating with an infected person are also routes of transmitting HIV. Similar misconceptions have been reported by previous study.18 Furthermore, participants exhibited very high level of knowledge about ways of prevention of HIV infection and general knowledge about HIV/AIDS. Few participants also had some misconceptions about preventive measures. Such misconceptions include isolation of infected person from others, use of insecticides among others. These knowledge gaps were consistent with findings of similar study carried out on HIV/AIDS.11 The high level of knowledge about HIV transmission and preventive measures among Nigerian university students as shown in this study may be connected with the aggressive campaigns that have over the years been championed by relevant health and community based institutions. In addition, the efforts of relevant organs of the United Nations, several non-governmental organizations and relevant government institutions have been aimed at educating the students on the causation, routes of transmission and preventive measures. This trend of findings has a very bright future for the prevention and control of HIV/AIDS pandemic among the youths.
Another finding of this study is that both male and female students have very good knowledge about HIV/AIDS. There was no significant difference in the knowledge about HIV/AIDS between male and female students. The finding is probably as a result of the readily accessible sources of HIV/AIDS information, which are made equally available to both sexes. The finding is in contrast to those of Aluede et al19 and Chang et al20 who reported a higher knowledge among male students and female students respectively.
The study showed a high level of risky sexual behavior among the participants. Over half of the participants practice pre-marital sex, have multiple sexual partners and do not use condom consistently during sexual intercourse. In addition, about half of the participants share sharp objects with people and about a third of the few married ones among them practice extramarital sex. The practice of these high risk behaviours is not compatible with high knowledge of HIV transmission and prevention exhibited by all the participants. This shows that the participants’ practice of preventive measures is still poor despite very high knowledge about HIV transmission and prevention. Although knowledge about a disease is a prerequisite for change, it has however been demonstrated that high knowledge about AIDS is not a predictor for behavioural change21, 22
Since there is no cure for HIV/AIDS at present, most activities are aimed at reducing HIV transmission. Apart from abstinence, the next most effective preventive measure against HIV/AIDS is use of condom during sexual intercourse. Thus the proportion of sexually active students who do not use condom during sexual intercourse suggest that current strategies are inadequate. Among the students that use condom, a significantly higher percentage of males use condom during sexual intercourse compared to females. This may be because some people especially females are not assertive enough to negotiate condom use with their sexual partners.23
Low risk perception of self-vulnerability was observed among the participants as over half of them think they are not at risk of contracting HIV infection. The acceptance of preventive measures depend largely on the degree to which the target population actually feels that HIV/AIDS is a real threat to them. Majority of those who have low risk perception of self-vulnerability practice risky sexual behaviours such as having multiple sexual partners, not practicing abstinence, not using condom during sexual intercourse than those who have high risk perception of self-vulnerability. Similar findings have been reported by other studies.14, 17, 24 This low risk perception of self-vulnerability to HIV infection is important as it may likely influence the attitude of the participants towards risky sexual behavior and practice of preventive measures.
Conclusions
Awareness and knowledge on certain aspects of HIV/AIDS is very high among the students of Ebonyi state University, south eastern Nigeria. However, despite high knowledge about HIV transmission and prevention, students still engage in high risk sexual behavior such as practicing pre-marital sex, having multiple sexual partners, non use or inconsistent use of condom during sexual intercourse and sharing unsterilized sharp objects. This is probably due to low perception of self-vulnerability to HIV infection among the students.
Failure to perceive HIV infection as a personal risk has prevented majority of the students from making commitment to sexual behavior change. Health education should therefore be refocused in such a way as to fortify the very high knowledge about HIV transmission and prevention, as well as to change the low perception of self-vulnerability to HIV infection observed among the students. This will help to improve their practice of safe lifestyles and reduce the incidence of HIV infection and death recorded among the youth.
Acknowledgements
The authors wish to thank the management of Ebonyi State University for permission to carry out the study. We are grateful to the concerned Deans and Heads of Departments for their support and assistance in mobilizing the students, and to the students who participated in the study.