Abstract
Objectives:
To evaluate the efficacy of a weight loss programme and the factors that predict successful adherence of the treatment.
Methodology:
A retrospective chart review of 500 overweight outpatients (427 women, 73 men), mean age 41.7 years (range: 18–81) and mean BMI of 31.44 kg/m2 (range: 25.09–51.33), treated at an obesity specific clinic. A programme involving a hypocaloric Mediterranean diet was prescribed, along with suggestions for leisure exercise and daily activity. The weekly follow-up continued until the weight loss goal was reached (‘completion’ group) or the patient discontinued the programme (‘dropout’ group).
Key Results:
Those that completed the programme achieved a mean weight loss of 10.6 kg (12.9% percentage loss of initial body weight) and a mean body fat mass loss of 26.8%. Factors predictive of completion were: gender (males higher completion), previous dietary programmes (predictive of dropout), initial percentage of fat mass (higher percentage, lower completion), age (younger age, lower completion) and hypothyroid disease (predictive of dropout).
Conclusions:
A hypocaloric Mediterranean diet and moderate exercise could help to reduce body weight and body fat in overweight patients. Treatment completion of self-selected and self-paying patients is low, and appear to be more effective for men, persons with a low percentage of fat mass, older age groups and those who have not made other previous diets.
Author Contributions
Academic Editor: Chung-Yi Chen, Fooyin University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Casanas-Quintana LT, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Because obesity seriously threatens the health of men and women, it must be considered a global epidemic 1. There are multiple causes of obesity, and the aetiology is not well known. It is partially attributable to physical inactivity and the overconsumption of calorie-dense foods 2, 3, 4.
In 2014, the reports of overweight individuals exceeded 1.9 billion. Of these, over 600 million were categorised as obese. Overall, about 13% of the world’s adult population (11% of men and 15% of women) were obese and 39% overweight (38% of men and 40% of women). Obesity more than doubled worldwide between 1980 and 2014 5.
The prevalence of general obesity in the adult population of Spain was 22.9% (24.4% of men and 21.4% of women); the overweight prevalence was about 39.4% (46.4% of men and 32.5% of women) according to the ENRICA study, carried out between June 2008 and October 2010 6. The Canary Islands and in southern Spain had a very high prevalence of obesity. With respect to the population of the Canary Islands, it appears to be an autonomous community with one of the highest prevalence of obesity, particularly among women, as determined by the National Health Survey 7.
Obesity treatment is difficult and results over time are very poor, and the vast majority of patients regain the lost weight. However, there is no doubt, as most experts indicate, that obesity must always be treated after an extensive study of the patient and the pathogenetic factors involved in fat accumulation. As a crucial aspect of all weight management programmes, dietary and lifestyle interventions help decrease energy consumption and increase its expenditure by implementing a balanced diet and exercise programme 8. The treatment or prevention of obesity could find solution through the Mediterranean diet, which has significant backing with evidence. Buckland and colleagues, in 2008, systematically reviewed and analysed epidemiological evidence on the Mediterranean diet and overweight/obesity. Albeit inconsistent, the results indicate a potential of the Mediterranean diet in preventing overweight/obesity, and physiological mechanisms can explain this protective effect 9.
Most often, obese patients fail in long term diet and exercise treatments. Identification of dropout predictors could be important for increasing recruitment in susceptible groups and developing guidelines to prevent those at high risk from dropout 10. Baseline factors that are associated with dropout, including sex, age, marital status and race, and so on, have reported in previous single study investigations 11.
The investigation to determine the efficacy of a hypocaloric Mediterranean diet (HMD) plus physical activity recommendations is the primary objective. This study also attempts to identify baseline characteristics of individuals that could predict successful completion of a weight loss programme.
Material and Methods
Study Design
A single-centre, retrospective chart review. Data were collected for a five year period.
Subjects
All procedures were in accordance with good clinical practices and were within the guidelines of the Helsinki Declaration for studies conducted using human subjects 12. The Ethical Committee of Las Palmas de Gran Canaria University accepted the study principles. Patients' data were codified to guaranty anonymity.
Between February 2009 and January 2013, 500 subjects agreed to a weight loss programme. The data was collected in consecutively enrolled participants attending our clinic specialising in obesity. The patients had a BMI >25 kg/m2 and were attending the clinic for the first time. The age range was between 18 and 81 y (mean= 41.7; standard deviation s.d.= 11.47) and the BMI was between 25.09 and 51.33 kg/m2 (mean=31.44; s.d.=4.41). The study finished in January 2014, when the last of the 500 subjects concluded the intervention.
Structure of the Programme
The patients agreed to a self-paying programme for weight loss through modification of diet and physical exercise recommendations. A complete clinical history was obtained and a complete physical examination was carried out in the first outpatient clinic visit, lasting 30–45 min. The blood chemistry data were solicited, when available, and nature of the programme was explained. Initially, through weekly follow up, evaluations were performed and solutions were suggested for problems that the patient might have been experiencing in adhering to treatment. When the patient discontinued treatment or, alternatively, the weight loss goal was reached, the treatment phase was considered to have ended. From there, the patient went on to the stage of weight maintenance, which focused on normalising caloric intake and physical exercise throughout a five-period week. The patient proceeded on to the follow-up stage of treatment, consisting of regular visits to the outpatient clinic every 15 days. Depending on the patient's needs and/or choice, the time-lapse between visits progressively lengthened to two or three months, with the objective to establish, and keep up, good lifestyle habits 13.
Characteristics of the Diet
In designing hypocaloric diets, body requirements and individual taste preferences were considered. The energy requirements, derived via the Harris–Benedict formula, were decreased by about 2.6 MJ/day according to the type of physical activity in order to induce an estimated loss ranging from 0.5 to 1 kg/week.
The general intake ranged from 3.8 to 5.8 MJ for male and 2.9 to 4.1 MJ for female subjects. For more obese individuals, this ran higher. The Mediterranean diet was used, which follows distributions of the principal components recommended by the Spanish Society of Community Nutrition (14]. The diet was comprised of 35% fat (<10% saturated and 20% of monounsaturated), 50% carbohydrates and 15% protein.
Physical Exercise
Regular moderate aerobic exercise at least three times a week for a minimum of half an hour/day was implemented in accordance with the US Expert Panel’s ‘Guide for the Identification, Evaluation and Treatment of the Overweight Adult’ 15. Adjustments were, of course, made given the patient’s capabilities. The increase of physical activity in daily habits were among other recommendations.
Determination of the Effectiveness of Treatment
'Completion' of the programme was defined as the patient reaching the previously agreed upon weight loss goal and the viability to proceed from weight maintenance to the follow-up stage of the programme. For statistical purposes, individuals unable to fulfil the treatment or maintenance requirements but had achieved a substantial weight loss were not considered in the 'completion' group.
The treatment duration varied as the individual goals and profile of each patient are different. The goal was agreed upon with the patient before intiating treatment and at an established minimum weight loss of 5% was set relative to baseline. When the desired weight loss goal was attained, the patient transitioned to the weight maintenance stage, which focused on normalising caloric intake and physical exercise throughout a five-period week. This was the point when the patient moved from ‘dieting’ to ‘not dieting’.
Variables Collected in the Study
The Following Variables were Collected:
Body mass index (kg/m2) was calculated by body mass in kilograms divided by body height in meters squared (m²). Weight was measured on a Tanita BF-350 Body Composition Analyser with a limit of 200 kg in 100 g increments. The patients wore light clothing without shoes. Height was measured subsequently using the Leicester metred scale with a range of 6–210 cm in divisions of 1 mm. The patients were segregated, for statistical purposes into groupings according to the 'Guidelines of the American Clinics for the Identification, Evaluation and Treatment of Obesity and Overweight in Adults' from the US Expert Committee on Obesity 15. These were: 1 – overweight: BMI between 25 and 29.9 kg/m2; 2 – obesity grade I: BMI between 30 and 34.9 kg/m2; 3 – obesity grade II: BMI between 35 and 39.9 kg/m2; and 4 – obesity grade III: BMI  40 kg/m2.
40 kg/m2.
Body Composition
Fat mass, lean body mass and body water were measured on a Tanita BF-350 Body Composition Analyser (Tetrapolar bio-electrical impedance analysis); measurement frequency 50kHz, measurement range 150–900 Ω. The patients were separated into groups based on the ‘Healthy Percentage Body Fat Ranges for Standard Adults Reported by Gallagher in 2000’ 16. These were: 1 – Healthy; 2 – Overfat; 3 – Obese.
Gender
Age is a continuous variable and in this study, it was separated into three groups: Group 1 – <35 y, Group 2 – between 35 and 45 y, Group 3 – >45 y.
Physical activity at the patient’s leisure was defined according to regular moderate physical aerobic exercise for a minimum of half an hour/day, as recommended by the US Department of Health and Human Services in their 'Dietary Guidelines for Americans 2005' 17.
Smoking habit was categorised as a function of the standard criteria, according to the recodification of the WHO guidelines, defined as: 1 – never smoked, those persons who have never smoked or who had smoked less than six months total during their lifetime; 2 – ex-smoker, those persons who are non-smokers at the time of visiting the obesity clinic but who previous smoked for a period of six months or more; 3 – smoker using one to four cigarettes/day or occasionally at the time of the study; 4 – smoker using 4–20 cigarettes/day or on occasion at the time of the study; 5 – smoker using >20 cigarettes/day at the time of the study. For simplicity sake in this study, the variable was as follows: 1 – smoker (comprised of groups 3, 4, and 5, above) and 2 – non-smoker (comprised of groups 1 and 2, above).
Alcohol in an amount of >40 g/day is defined as excessive by the Spanish Society for Community Nutrition 18 (Sociedad Española de NutriciónComunitaria; SENC), which corresponds to more than two to three alcoholic beverages, such as 330 ml bottles of beer, 80 ml glasses of wine, or the standard measurements for distilled alcohol (cognac, whisky, anis, etc.) 18, 19.
Hypothyroidism was defined as participants that were under medical treatment with thyroid hormones.
Previous experience of diets for weight loss.
Childhood obesity was defined ascommencement of obesity during infancy or adolescence.
Duration of treatment was defined as the length of time the patient complied with the programme, that is, successfully completed the weight maintenance or, alternatively, stage up to the time the patient abandoned the treatment.
'Completion' of the programme, as defined above.
Statistical Analyses
The SPSS statistical package (version 15.0. for Windows) was used throughout the data analysis. The qualitative variables and measurements of central tendency (mean or median) and measures of dispersion (standard deviation; s.d.) for quantitative variables were tested by the descriptive analyses of the variables. Using the ϰ2 test, bivariate analyses for the proportionality of distribution of categorical variables were calculated. We used the Kolmogorov–Smirnov test to verify that the variables were distributed in a normal fashion for continuous variables. P>0.05 was considered normal. In comparing variables, durations in which the distributions were not normal, like BMI, age, weight loss, percentage weight loss and treatment, the comparisons of absolute means among groups were measured using Wilcoxon test, a nonparametric, for the sum of the ranges.
The evaluation of the impact of the differing variables linked with obesity (age, gender, BMI, etc.) across the time of treatment (from start to finish of the programme, whether due to having lost the desired weight, in other words, 'completion' of the programme, or having discontinued the programme, in other words, 'dropout'), we used the survival analysis of the Cox step-by-step towards regression with the Z statistic of Wald. Whether categorical or continuous, this permitted the impact of multiple covariables in the same model to be assessed. The measures taken were: to select the variable 'duration' of time of survival, as indicated by the amount of time it took the patient to follow the programme in order to lose the desired weight, or the follow-up period until the patient discontinued the programme without having last the desired weight. The status variable was defined as an 'event' with the option of 'yes' for the 'completion' variable. Covariables were body fat percentage, age (continuous), BMI (continuous), alcohol, smoking habit, gender, hypothyroidism, previous diets, physical exercise, and age of commencement of obesity. The statistic values standard error of B, generated were coefficient (B), levels of significance, Wald statistic, the 95% confidence interval (95% CI) of the value exp(B) and reason of the estimated advantages (exp(B)). Significance was set at P<0.05 (13).
Results
The mean age of the participants was 42 ± 12 y (range: 18–81 y), BMI was 32 ± 5 kg/m2 (range: 25–51), and the body fat percentage was 39.41 ± 6.03% (range: 20–54). In addition, 85.4% of the participants were women. According to BMI classification, 44% were overweight, 37% were class I obese, 13.6% were class II obese and 5.4% were class III obese. The mean time on programme was 3.75 ± 4.70 months. The participants that reached the weight loss goal (21.4%) had done so in a mean period of adherence to the programme of 6.40 months (Table 1). All the patients in the “completion” group, finished the maintenance stage and were introduced in good lifestyle habits.
Table 1. Characteristics of the patients segregated with respect to weight loss treatment completion| Completion | |||||
| Characteristic | Total (n=500) | Yes (n=108) | No (n=392) | p | |
| Gender | Male (%) | 14.6 | 15.7 | 14.3 | 0.403a |
| Female (%) | 85.4 | 84.3 | 85.7 | ||
| Age (years) | Mean ± s.d. | 41.7 ± 11.47 | 42.94 ± 11.01 | 41.35 ± 11.58 | <0.001b |
| <35 (%) | 29.8 | 23.1 | 31.6 | 0.169a | |
| 35-45 (%) | 34.6 | 40.7 | 32.9 | ||
| >45 (%) | 35.6 | 36.1 | 35.5 | ||
| Baseline BMI(kg/m²) | Mean ± s.d. | 31.44 ± 4.41 | 29.68 ± 3.64 | 31.93 ± 4.49 | <0.001b |
| Baseline Body fat percentage | Mean ± s.d. | 39.41 ± 6.03 | 37.22 ± 5.57 | 40.02 ± 6.02 | <0.001b |
| Time on program | Mean ± s.d. | 3.75 ± 4.70 | 6.40 ± 4.58 | 3.02 ± 4.47 | <0.001b |
| Hypothyroid diseasec | (%) | 9 | 3.7 | 10.5 | 0.018a |
| Smoking habitd | (%) | 14 | 10.2 | 15.1 | 0.127ª |
| Alcohol abusee | (%) | 7.2 | 7.4 | 7.1 | 0.532ª |
| Physical exercisef | (%) | 32.6 | 38 | 31.1 | 0.111ª |
| Childhood obesityg | (%) | 29.8 | 23.1 | 31.6 | 0.054ª |
| Previous diets | (%) | 86 | 16.4 | 69.5 | 0.001ª |
In the patients who reached the weight loss goal, the weight change mean was -10.6 ± 5.8 kg, equivalent to a 12.9% percentage loss of initial body weight. The fat mass change was -8.3 ± 5.2 kg and the percentage loss of initial fat mass was 26.8 ± 10.9%. Within-group, the unadjusted weight change was −4.2 ± 4.2 kg and the fat mass change was 3.1 ± 3.6 (Table 2).
Table 2. Change in weight and body composition with respect to weight loss treatment completion| COMPLETION | VARIABLE | Pre | Post | Absolute change | Percentage change | p |
| YES | Weight (kg) | 79.0 ± 13.2 | 68.4 ± 9.3 | 10.6 ± 5.8 | 12.9 ± 5.2 | <0.001a |
| BMI (kg/m2) | 29.68 ± 3.64 | 25.69 ± 2.14 | 3.98 ± 2.06 | 12.94 ± 5.21 | <0.001a | |
| Fat mass (kg) | 29.6 ± 7.9 | 21.3 ± 4.8 | 8.3 ± 5.2 | 26.8 ± 10.9 | <0.001a | |
| Lean body mass (kg) | 49.4 ± 8.5 | 47.1 ± 8.1 | 2.3 ± 1.7 | 4.6 ± 3.2 | <0.001a | |
| Body water (kg) | 36.2 ± 6.3 | 34.5 ± 5.9 | 1.7 ± 1.2 | 4.6 ± 3.2 | <0.001a | |
| NO | Weight (kg) | 87.0 ± 15.0 | 82.8 ± 13.9 | 4.2 ± 4.2 | 4.7 ± 4.3 | <0.001a |
| BMI (kg/m2) | 31.93 ± 4.49 | 30.38 ± 4.16 | 1.54 ± 1.54 | 4.68 ± 4.28 | <0.001a | |
| Fat mass (kg) | 35.0 ± 9.5 | 31.9 ± 8.9 | 3.1 ± 3.6 | 8.6 ± 8.8 | <0.001a | |
| Lean body mass (kg) | 51.9 ± 9.2 | 50.8 ± 9.0 | 1.0 ± 1.7 | 2.0 ± 3.1 | <0.001a | |
| Body water (kg) | 38.0 ± 6.7 | 37.2 ± 6.5 | 0.7 ± 1.3 | 2.0 ± 3.1 | <0.001a |
The regression analysis, with the outcome variable set at weight loss 'completion' (as previously mentioned), highlighted the variables in the stage of active weight loss in the overall study sample as being the variables that effected an individual's completion of the programme, were gender, age, baseline body fat percentage, hypothyroid disease and prior participation in weight loss programmes (Table 3). A male was 3.7 times more likely to complete the programme than was a female counterpart. For each year of age, the possibility of completion went up by 3.4%. For each unit decrease in initial body fat percentage, the possibility of completion increased by 12.6%. Previous attempts at a dietary programme reduced the possibility of completion by 45%. In those individuals suffering from hypothyroidism, the probability of “completion” was reduced by 77%.
Table 3. Factors associated with overweight and obese patients achieving completion on the weight loss program| COVARIABLES | B | s.e. | Wald value | p-value | Exp (B) | 95% CI |
| Gender | 1.27 | 0.517 | 6.042 | 0.014 | 3.562 | 1.294 - 9.811 |
| Age | 0.034 | 0.01 | 11.042 | 0.001 | 1.034 | 1.014 - 1.055 |
| Fat mass percentage | -0.119 | 0.038 | 9.582 | 0.002 | 0.888 | 0.824 - 0.957 |
| Previous diets | -0.605 | 0.151 | 16.037 | <0.001 | 0.546 | 0.406 - 0.734 |
| Hypothyroid disease | -1.47 | 0.538 | 7.506 | 0.006 | 0.229 | 0.08 - 0.657 |
Figure 1 illustrates the survival analysis of reaching the weight loss goal as a function of group of initial fat mass percentage and dropout rates relative to groups of baseline body fat percentage of the subjects. “Completion” of the treatment was lower in groups with a baseline higher body fat percentage.
Figure 1. Survival analysis: Completion of the treatment as a function of initial fat mass.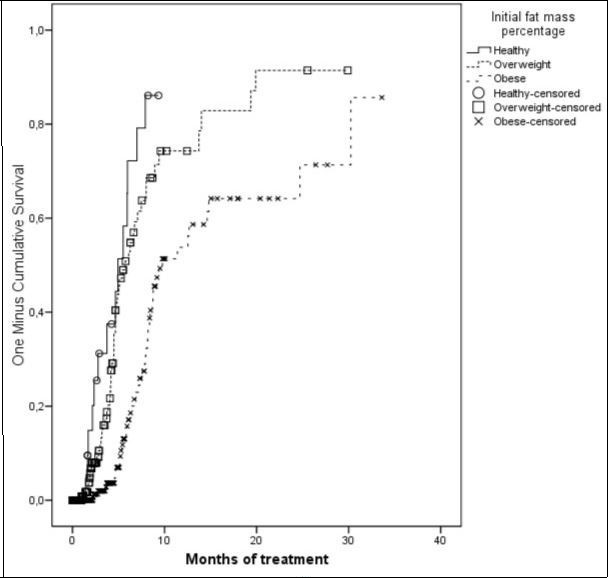
Discussion
Strengths and Limitations of the Study
The present study has several limitations. The selection of subjects was not randomly performed. The data were gathered in consecutively enrolled participants in real-life settings, as opposed to data gathered in controlled research settings, where a more rigorous inclusion criteria has the possibility to limit external validity. However we consider that this kind of studies could also be useful to understand the problem of obesity in real life. We enrolled few men (14.6 %). This must be taken into account in the comparative results between sexes. However this fact is repeatedly observed in other studies on weight reduction treatments (13,20,21] probably because men are less likely to perform this type of treatment.
The strengths of the study include that all data were collected by a single observer, in the same place and with the same measurement instruments which implies a reduced measurement error both intra - observer and between instruments. Also, all data were treated and analyzed by the same investigator. Several studies have indicated that the differences between observers are significantly greater than the intra-observer differences 22. We have not found survival studies that had considered the percentage of fat mass as an adherence predictor to treatment.
Finally, we would highlight that all subjects were part of a real population, taking weight loss treatment voluntary in an obesity clinic.
Efficacy of a Hypocaloric Mediterranean Diet
Our data suggest that both HMD plus the recommendations of physical activity were effective at reducing weight and fat mass of overweight and obese adults, as hypothesised.
Attrition rates in obesity trials range from 10% to 80% 23, 24, 25, 26. This elevated percentage of variability may be due to differing methodologies. Not many published studies report the results found in specialised obesity clinics and, in reviewing, we noted similar difficulty and variability in attempting to define the precise criteria that would outline a sufficient conclusion of a weight loss programme.
In this study, 51.8% of patients experienced more than a 5% reduction of baseline body weight. Numerous reports have concluded that modest weight losses of 5–10% were associated with significant improvements in related comorbidities (hypertension, diabetes, hyperlipidemia, cardiovascular disease, osteoarthritis, sleep apnea, etc.) in obese subjects 27, 28, 29, 30, 31, 32. Moreover, a Mediterranean type diet appears to be more effective in inducing clinically significant long-term improvements in cardiovascular risk factors and inflammatory markers than a low fat diet 33.
Just 21.4% of the patients achieved the weight loss goal previously agreed upon and successfully completed the weight maintenance stage. Despite the high attrition rate, the completers resulted in a mean weight loss of 10.6 kg (12.9%) from the starting weight during the first six months.
In a recent systematic review of randomised clinical trials focused on weight loss, having at least a one-year follow-up, Franz and colleagues 34 reported that a mean weight loss of 5 to 8.5 kg (5% to 9%) was noted during the initial six months due to interventions involving a reduced-energy diet and/or weight loss medications, with weight plateaus occurring at approximately six months. The magnitudes of the loss of weight noted in the present study suggest that a hypocaloric Mediterranean diet plus physical activity could be an effective way to improve weight loss in obesity treatments.
In 2015, Clark and colleagues 35, in a systematic review and meta-analysis, focused on comparing changes from treatment programmes for adults who were overfat. They observed that when exercise and diet is combined you obtained better results than diets alone in reducing body mass and fat mass and at the same time maintaining lean body mass following treatment.
The results of the current study indicate that the combination of a hypocaloric MD and regular moderate physical aerobic exercise may be effective at reducing weight, as well as body fat percentage (-26.8% from baseline), in patients complying with the treatment.
Factors Predictive of Completion
The second objective was to identify baseline characteristics that can help us predict further compliance with the weight loss programme. A number of factors might influence adherence to a diet, for example the length of intervention, disease state, patient support, and restrictiveness 36. It is very difficult to compare from other studies because the strategies involved in the studies are different than that of the present study. In the present study, the results are based on the 'survival analysis'. Which permits a prediction for individuals who initiate and follow through with the programme over different timeframes to be formulated. We can estimate, as well, the importance of the differing variables druing the entire period that the patient stays on the programme and achieves the objectives.
The factors associated with the completion of the treatment were gender (males higher completion), baseline fat mass percentage (higher percentage, lower completion), attending to previous dietary programmes (predictive of less completion), age (worse results in the young) and hypothyroid disease (predictive of dropout). Initially, the survival study was performed excluding the variable fat mass percentage, and here, BMI appeared as predictor of successful completion. By including fat mass percentage in the Cox regression analysis, the influence of BMI was nullified.
In a 2014 systematic review of randomised trials of weight loss interventions using traditional diet and/or exercise interventions, Kaiser and colleagues found that the possibility of dropout was significantly higher for females than for males, as well as in those subjects with a higher BMI 10. In 2015, another study also suggested that a higher level of obesity were more likely to drop-out 37.
Conflicting results have been observed between age and attrition 38. Weight loss programmes conducted in research settings showed no association between relatively young age and treatment discontinuation 39, 40, 41, 10, while the present study and other studies found that relatively young age was an important predictor of dropout 19, 20, 21, 37, 42, 43. Some authors hypothesised that older patients were aware of the health benefits of weight loss 44.
Our findings suggest that having experienced previous diet programmes significantly reduced the probability of completion. Bautista and colleagues 19 also reported similar results. However, previous experience of weight loss predicts attrition only in selected reports. In our review of the literature, we did not find studies related to predicting the role of fat mass percentage on attrition.
Desertion is lower in patients treated with cognitive behavioural therapy 45, 46, 47, and the expected rates outside the controlled studies are even higher 48. In several studies, it was observed that the total stress level differentiates patients who do not continue treatment from those who finish the programme 37, 49, 50. Dietary programme alone is not the sufficient to treat overweight and obese patients who suffer psychological distress because they are unable to control anxiety that nutritional strictness produces 37.
We subscribe to the belief that, in the short term, diet programmes may produce weight loss 51, 52, however the maintenance of this weight loss is often difficult and often requires doing exercise and following a lower-energy diets as a long term habit in a person’s lifestyle 53. A comprehensive programme of lifestyle modification is considered the first option for losing weight and maintaining this weight loss (National Institute, 98) 54. Lifestyle modification, i.e. behavioural weight control, is comprised of three primary components: exercise, diet, and behaviour therapy 55.
There is not enough consistency between the results of different studies regarding predictors of successful treatment for weight reduction. The results of this study may not be suitable for select high-risk groups of patients, but could be useful in understanding compliance probabilities with respect to obesity treatments in outpatient clinics.
Conclusions
In conclusion, a hypocaloric Mediterranean diet and moderate exercise could help to reduce body weight and body fat mass in overweight patients. Treatment completion of self-selected and self-paying patients is low, and appear to be more effective for men, persons with a low percentage of fat mass, older age groups, subjects without hypothyroid disease and those who have not made other previous diets.
This study help to reinforce the efficacy of the hipocaloric Mediterranean Diet in fat mass reduction and the importance of the initial body fat mass in the dropout rate. We have not found other studies regarding this issue.
Further studies of both the factors predisposing one to failure and those that contribute to improving adherence to different treatments are needed.