
High Prevalence of Obesity in a Saudi Community K.Aljabri, MD, FRCPC, S. Bokhari, MD. A Cross Section, Single Centre Study
Abstract
Objective:
Obesity is a major public health problem worldwide. We designed this study to determine the prevalence of obesity among Saudis in the department of primary care at King Fahad Armed Forces Hospital.
Methods:
Cross section study of Saudis of both sexes, aged more than or equal to 12 years at the department of primary care at King Fahad Armed Forces Hospital between January 2008 and June 2009.
Results:
A total of 5968 were attending the department of primary care were included in this study. There were 2269 (38.0%) male and 3699 (62.0%) female. With age, a gradual increase was seen in the Body mass index (BMI) in both males and females, up to the age of 59 years, with a decrease occurring thereafter. In the females below 20 years of age, the BMI was lower than in the male group. Above 30 years, the BMI in females was higher than in the males of corresponding ages. The prevalence of BMI≥25 was 70.0%.The prevalence of BMI≥25 was non significantly higher in the male compared to the female,71% and 69.3% respectively, p=0.2.The prevalence of overweight ( BMI=25-29.9) was higher in the males compared to the females, while the reverse was true for obesity(≥30),where 62.0% of the total female population was obese compared to 49.7% of the total male population. The magnitude of the difference in prevalence of obesity in the males and females was significantly high ( p<0.0001).
Conclusion:
The prevalence of obesity is high among Saudi population at the primary care setting and represents a major clinical and might represent a public health problem. A national prevention program at community level should be implemented.
Article Information
- Received
- Accepted
- Published
Academic Editor: M. Javed Ashraf, Truman Medical Center/UMKC School of Medicine
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Khalid S. Aljabri, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: Khalid S.J. Aljabri, MD, Department of Endocrinology, King Fahad Armed Forces Hospital, Jeddah, Kingdom of Saudi Arabia —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
We are grateful to secretaries of the department of primary care at King Fahad Armed Forces Hospital for their valuable contributions in data collection and organizational help.
Citation:
Introduction
Obesity, and overweight are both defined as excessive accumulation of fat in the body.1, 2 Recent publications have shown that obesity has progressively higher morbidity and mortality and it is a major medical and public health problem world-wide and ultimately may cause several health conditions like type 2 diabetes mellitus, insulin resistance, cardiovascular and cerebrovascular diseases, certain types of cancers, hypertension, gallbladder disease, nonalcoholic steatohepatitis, and obesity hypoventilation syndrome.3, 4, 5, 6 Obesity is an epidemic all around the world. Recent reviews have reported significant increases in the prevalence of overweight and obese individuals in developing countries and in Saudi Arabia. 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17 A variety of factors influence the rate of obesity in any particular region, including age patterns, socioeconomic factors and a lack of physical activity. 18, 19 Our understanding of such issues will help us to plan for excellent health care and improving our abilities to manage such cases. Our study is a cross-sectional study designed to estimate the prevalence of overweight and obesity in an adult population in Jeddah, west province of Saudi Arabia.
Methods
We conducted a cross section study during the month of June 2009. Randomly interviewed participants and demographic data were collected. Weight (kg) and height (cm) were measured by physician and nurse interviewers and recorded. Patients were the population at the department of primary care at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia between January 2008 and June 2009. Overweight and obesity were defined as Body Mass Index (BMI) 25-29.9 and ≥ 30.0 kg/m2 respectively.20 The study was approved by the ethical board of King Fahad Armed Forces Hospital.
Statistical Analysis
Continuous variables were described using means and Standard Deviations. Univariate analysis of baseline demography both between and within groups, were accomplished using unpaired t-test and Chi square test were used for categorical data comparison. Pearson correlation was used for correlation between variables and linear regression analysis used as appropriate. P value <0.05 indicates significance. The statistical analysis was conducted with SPSS version 17.0 for Windows.
Results
A total of 5968 were attending the department of primary care were included in the study. There were 2269 ( 38.0 % ) male and 3699 ( 62.0 %) female. The males and females were categorized according to age into different groups and the mean and standard deviation of BMI were calculated. The results are presented in Table 1. With age, a gradual increase was seen in the BMI in both males and females, up to the age of 59 years, with a decrease occurring thereafter. In the females below 20 years of age, the BMI was lower than in the male group. Above 30 years, the BMI in females was higher than in the males of corresponding ages. Clearly the age curves separated after the age of 30 and persisted thereafter, Figure 1. The correlation between age and BMI is statistically significant (r=0.3, P<0.0001).
Table 1. Body mass index ( mean ± Standard Deviation) of patients stratified by age and gender| Age groups | Male | Female | Total | |||
|---|---|---|---|---|---|---|
| (years) | Number | BMI | Number | BMI | Number | BMI |
| 19-Dec | 209 | 21.6 ± 6.5 | 268 | 21.0 ± 5.8 | 477 | 21.3 ± 6.2 |
| 20-29 | 422 | 26.4 ± 6.5 | 978 | 26.4 ± 6.9 | 1400 | 26.4 ± 6.8 |
| 30-39 | 463 | 28.8 ± 5.7 | 768 | 29.4 ± 7.0 | 1231 | 29.2 ± 6.5 |
| 40-49 | 361 | 29.1 ± 5.0 | 643 | 31.8 ± 7.2 | 1004 | 30.8 ± 6.6 |
| 50-59 | 304 | 30.1 ± 4.9 | 618 | 32.4 ± 6.9 | 922 | 31.7 ± 6.4 |
| ≥60 | 510 | 28.8 ± 5.3 | 424 | 31.2 ± 6.9 | 934 | 29.9 ± 6.0 |
| Total | 2269 | 27.9 ± 6.0 | 3699 | 29.1 ± 7.6 | 5968 | 28.7 ± 7.1 |
Figure 1. Mean body mass index and different age groups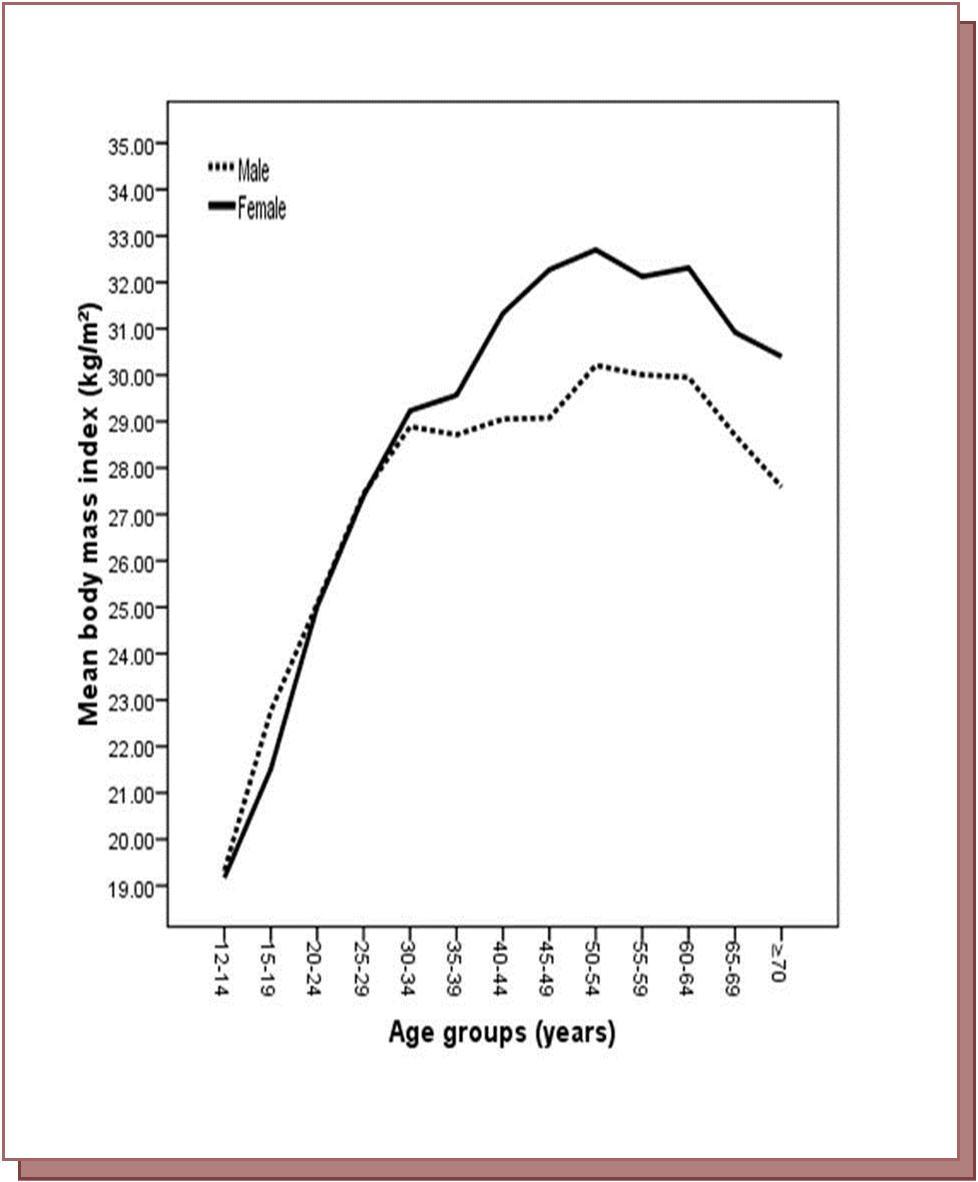
Download figure
Further division of the data was made according to each age groups with each BMI categories. The prevalence was calculated and the results are presented in Table 2. There were several differences in the prevalence of obesity and overweight in the different age groups. In most of the areas overweight was more common in the males compared to females, while the reverse was true for obesity.
Table 2. Prevalence of patients (%) stratified by body mass index categories to age and gender| Age groups (years) | Gender | ||||||||
| Body mass index groups | 19-Dec | 20-29 | 30-39 | 40-49 | 50-59 | ≥60 | Male | Female | Total |
| <18.5 | 47.5 | 35.9 | 7.8 | 4 | 1.5 | 3.3 | 6.5 | 6.8 | 6.7 |
| 18.5-24.9 | 11.9 | 36.3 | 28 | 10.3 | 7.5 | 13.3 | 22.5 | 23.9 | 23.4 |
| 25-29.9 | 3.9 | 21.8 | 24.1 | 18.3 | 14.7 | 17.2 | 35.8 | 26 | 29.7 |
| 30-34.9 | 2.8 | 15.3 | 19.4 | 21.3 | 22 | 19.2 | 24.9 | 23.9 | 24.3 |
| 35-39.9 | 1.3 | 14.2 | 21.5 | 22 | 23.5 | 17.5 | 8.1 | 12.1 | 10.6 |
| ≥40 | 0.6 | 16.2 | 20.6 | 22.8 | 25.9 | 13.8 | 2.2 | 7.3 | 5.4 |
| Total | 477 | 1400 | 1231 | 1004 | 922 | 934 | 2269 | 3699 | 5968 |
The prevalence of BMI ≥ 25 was 70.0%. The prevalence of BMI ≥ 25 was higher in the male compared to the female, 71% and 69.3% respectively, p=0.2. The prevalence of obesity and overweight was calculated in the total males and females and the results are presented in Figure 2, Figure 3. The prevalence of overweight ( BMI = 25-29.9 ) was higher in the males compared to the females, while the reverse was true for obesity (≥30), where 62.0% of the total female population was obese compared to 49.7% of the total male population. The magnitude of the difference in prevalence of obesity in the males and females was significantly high ( p<0.0001).
Figure 2. Prevalence of overweight and obesity to gender
Download figure
Figure 3. Prevalence of overweight and obesity to gender in different age groups
Download figure
Discussion
Our study shows that overweight and obesity is prevalent among Saudi population. There is apparently gradual weight gain with age, which tends to decrease gradually after the age of 60. The decline in mean BMI in the oldest age group was consistent with other studies.21, 22, 23, 24 The increase in obesity levels with age is of concern, as it has been shown that obese elderly are more likely to present with major chronic health conditions and poor general health.25
Our study showed that obesity were more prevalent among females than males and the difference was evidently more in the age groups older than 30. The Asia Pacific Cohort Studies Collaboration reports prevalence rates ranging from less than1% to higher than 20% for countries in the Asia-Pacific region.26 According to National Health and Nutrition Examination Survey of the United States, the prevalence of obesity in individuals aged 20–74 years was 34% in females and 31.7% in males.27 The corresponding figures in Australia were 19% and 17%, respectively.28 In the United Kingdom, the prevalence of obesity was estimated to be 24.2% in females and 23.7% in males.29 The results from most of our neighboring countries, including Oman, 23.8% in females and 16.7% in males.30 Lebanon, 18.8%in females and 14.3% in males,31 Turkey as well, the prevalence of obesity is higher in females 24.6% vs. 14.4% in males32 and Iran, the prevalence of obesity to be 22.3% among Iranian adults (30.6% in females and 14.2% in males.33 In Saudi Arabia, the National Epidemiological Household survey among Saudi subjects over the age of 15 years in different regions of Saudi Arabia showed the prevalence of overweight among male subjects was significantly higher than for female subjects (29% vs. 27%), and the prevalence of obesity among female subjects was significantly higher than for male subjects (24% vs. 16%).16 A community-based national epidemiological health survey, conducted by examining Saudi subjects in the age group of 30-70 years of selected households over a 5-year period between 1995 and 2000 showed that the prevalence of obesity was 35.6% and females are significantly more obese with a prevalence of 44% than males 26.4%.17
BMI has been proved as useful index for large scale epidemiological work.34 The West of Scotland Coronary Prevention Study prospectively followed 5,947 men for 4.9years to predict incident of diabetes. In a multivariate regression model, BMI is significant independent predictors for diabetes.35 A series of cohort studies have shown the association between BMI and the risk of diabetes.36, 37, 38 About half of all new diagnoses of diabetes were made in persons with a BMI >30 kg/m2, and almost 20% have a BMI >35 kg/m2 at the time the diagnosis is made . A recently published study found 13 persons with diabetes for every 100 overweight or obese persons in the US, 99/100 in India, 25/100 in the Philippines, 37/100 in Taiwan, 34/100 in Hong Kong, 19/100 in China, 28/100 in Singapore, 25/100 in Korea, and 34/100 in Thailand.39 In Saudis studies, it was shown that the prevalence of obesity was significantly higher in diabetic and hypertensive Saudis compared to the non-diabetic and non-hypertensive controls. 11, 40, 41 Control of obesity is essential in order to prevent the development of other chronic diseases such as diabetes mellitus, hypertension and cardiovascular disease.. Weight reduction, which is a possibility in most cases, is associated with significant reduction in the frequency of some of the major complications related directly to obesity.42
The results of this study have three important implications for national obesity prevention and management programs. First, it appears that obesity prevalence rates will almost certainly continue to rise in the Saudi population over the next decade. The rapid aging of the currently very young Saudi population into high-risk older age-groups will maintain the spread between incidence and morbidity into the foreseeable future. Even if incidence rates were flat or declining due to a breakthrough in obesity prevention, prevalence rates would continue to rise. As a result, the health burden due to all types of obesity complications will likely continue. This means that the health care and social service systems should start preparing now to provide the prevention and support services and systems, a large number of adults with obesity are going to require to maintain quality of life. These include healthy life programs which is currently implemented in our institution, dietary counseling services, and enhanced infrastructure at the community level to facilitate independent living by adults with limited mobility and eyesight. Second, "upstream" population-based primary prevention programs need to be aggressively implemented to ensure that obesity incidence begins to decrease in the future. The dramatically higher rates of obesity in the Saudi population highlight the urgency of this activity. Because obesity appears to be closely related to the adoption by people of many aspects of the modern lifestyle including diet and low levels of physical activity, prevention programs that draw upon Aboriginal traditions and ways of life and that focus on the lifestyle habits of Aboriginal youth need to be implemented. A number of very promising primary prevention programs that draw upon Aboriginal traditions and ways of life have been implemented in our institution. Third, the reason for the higher prevalence of obesity in Saudi women observed in this study also needs to be better understood.
In conclusion, this study has demonstrated an epidemiological information on the extent of obesity as a health problem and the value of having accurate population-based information on the epidemiology of obesity in our population in the future. By providing information on the trajectory and the geography of the obesity in our centre, it provides important clues as to the magnitude and structure of the primary and secondary intervention programs that will be required to effectively manage this disease.
References
- 2. (1988) World Health Organization. Measuring obesity: Classification and Description of nthropometric Data Report on a WHO Consultation on the Epidemiology of Obesity. Copenhagen: WHO Regional Office for Europe, Nutrition Unit:.
- 3.Adams K F, Leitzmann M F, Ballard-Barbash R, Albanes D, Harris T B et al. (2014) Body Mass and Weight Change in Adults in Relation to Mortality Risk. , Am J Epidemiol; 179(2), 135-44.
- 4.Jee S H, Sull J W, Park J, Lee S Y, Ohrr H et al. (2006) Body-mass index and mortality in Korean men and women. , N Engl J Med; 355, 779-787.
- 5.Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi M G. (2005) The INTERHEART Study Investigators. Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case control study. , Lancet; 366, 1640-1649.
- 6.Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A. (2004) The INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. , Lancet; 364, 937-952.
- 7.Chopra M, Galbraith S, Danton-hill I. (2002) A Global re-sponse to a global problem: the epidemic of over-nutrition. Bulletin of the world Health Organization. 80(12), 952-958.
- 8.Lafta R, Kadhim M. (2005) Childhood Obesity in Iraq: Prevalence and possible risk factors. , Ann Saudi Med; 25(5), 389-393.
- 9.Al Shammari S, Khoja T, Al Maatouq M. (1996) Prevalence of Obesity among Saudi male in the Riyadh region. , Ann Saudi Med; 16(3), 269-273.
- 10.Al Shammari S, Khoja T, Al Maatouq M, Al Nuaim L. (1194) High prevalence of clinical obesity among Saudi females: a prospective, crosssectional study in the Riyadh region. , Journal of Tropical Medicine and Hygiene; 97, 183-188.
- 11.Warsy A, M El Hazmi. (1999) Diabetes mellitus, hypertension and Obesity- common multifactorial dis-orders in Saudis. , Eastern Mediterranean Health Journal; 5(6), 1236-1242.
- 12.Abolfotouh M, Daffallah A, Khan M, Khattab M, Abdulmoneim I. (2001) Central Obesity in elderly individu-als in south-western Saudi Arabia: Prevalence and associated morbidity. , Eastern Mediterranean Health Journal;7(4-5): 716-724.
- 13.Al Qahtani D, Imtiaz M, Shareef M. (2005) Obesity and Cardiovascular risk factors in Saudi adult soldiers. , Saudi Med J; 26(8), 1260-1268.
- 14.Al Qahtani D, Imtiaz M, Shareef M. (2005) Prevalence of metabolic syndrome in Saudi adult soldiers. , Saudi Med J; 26(9), 1360-1366.
- 15.Bartali B, Benvenuti E, Corsi A M, Bandinelli S, Russo C R et al. (2002) Changes in anthropometric measures in men and women across the life-span: findings from the InCHIANTI study. , Soz Praventivmed; 47, 336-348.
- 16.Al Nuaim A, Al Rubeaan K, Al Mazrou Y, Al Attas O, Al Daghari N et al. (1996) High Prevalence of Overweight and Obesity in Saudi Arabia. , International Journal of Obesity; 20, 547-552.
- 17.Al-Nozha M M, Al-Mazrou Y Y, Al-Maatouq M A, Arafah M R, M Z Khalil.. (May3005) Obesity in Saudi Arabia. Saudi Med J; 26(5), 824-9.
- 18.Heitmann B L. (1999) [Occurrence and development of overweight and obesity among adult Danes aged 30-60 years]. Ugeskr Laeger;. 161, 4380-4384.
- 19.Lindstrom M, Isacsson S O, Merlo J. (2003) Increasing prevalence of overweight, obesity and physical inactivity: two population based studies1986and1994. , Eur J Public Health; 13, 306-312.
- 20. (1999) World Health Organization: Obesity: preventing and managing the global epidemic: report of a WHO consultation. , Geneva, Switzerland
- 21.Reeder B A, Chen Y, Macdonald S M, Angel A, Sweet L. (1997) Regional and rural-urban differences in obesity in Canada. Canadian Heart Health Surveys Research Group. Can Med Ass J;157(Suppl1):. 10-16.
- 22. (1983) Fitness and lifestyle in Canada. A report by Canada Fitness Survey. Ottawa ( CA): Fitness and Amateur Sport Canada;.
- 23. (1987) Health and Welfare Canada. The active Health Report: perspectives on Canada health Promotion Survey1985.Ottawa(CA):Minister of Supply and Services.
- 24.Asya A, Al-Riyami Mustafa M Afifi. (2003) Prevalence and correlates of obesity and central obesity among Omani adults. , Saudi Medical Journal 24(6), 641-646.
- 25.Andreyeva T, Michaud P C, A van Soest. (2007) Obesity and health in Europeans aged 50 years and older. Public Health;. 121, 497-509.
- 26. (2007) Asia Pacific Cohort Studies Collaboration: The burden of overweight and obesity in the Asia-Pacific region. Obes Rev;. 8(3), 191-196.
- 27.Ogden C L, Yanovski S Z, Carroll M D, Flegal K M. (2007) The epidemiology of obesity. , Gastroenterology; 132(6), 2087-2102.
- 28.Australian Instituteof Health and Welfare: Australia’s Health 2006: the tenth biennial health report of Australian Institute of Health and Welfare .
- 30.Al-Lawati J A, Jousilahti P J. (2004) Prevalence and 10-year secular trend of obesity in Oman. Saudi Med J. 25(3), 346-351.
- 31.Sibai A M, Hwalla N, Adra N, Rahal B. (2003) Prevalence and covariates of obesity in Lebanon: findings from the first epidemiological study. Obes Res. 11(11), 1353-1361.
- 33.Esteghamati A, Meysamie A, Khalilzadeh O, Rashidi A, Haghazali M. (2009) Third national surveillance of risk factors of non-communicable diseases (SuRFNCD-2007) in Iran: methods and results on prevalence of diabetes, hypertension, obesity, central obesity, and dyslipidemia. BMC Public Health. 9-167.
- 34.Wells J C K. (2000) A Hattori chart analysis of body mass index in infants and children. , International Journal of Obesity; 24, 325-329.
- 35.Sattar N, Gaw A, Scherbakova O, Ford I, O’Reilly D S et al. (2003) Metabolic syndrome with and without C-reactive protein as a predictor of coronary heart disease and diabetes in the West of Scotland Coronary Prevention Study. , Circulation; 108, 414-419.
- 36.Ford E S, Williamson D F, Liu S. (1997) Weight change and diabetes incidence: findings from a national cohort of US adults. , Am J Epidemiol; 146, 214-22.
- 37.Leibson C L, Williamson D F, Melton L J. (2001) Temporal trends in BMI among adults with diabetes. Diabetes Care. 24, 1584-9.
- 38.Burke J P, Williams K, Narayan K M, Leibson C, Haffner S M et al. (2003) A population perspective on diabetes prevention: whom should we target for preventing weight gain? Diabetes Care;. 26, 1999-2004.
- 39.Yoon K H, Lee J H, Kim J W. (2006) Epidemic obesity and type 2 diabetes in Asia. , Lancet; 368, 1681-8.
- 40.Al-Turki Y. (2000) The prevalence of overweight and obesity amongst hypertensive and diabetic adult patients in primary health care. , Saudi Medical Journal 21(4), 340-343.
Cited by (10)
This article has been cited by 10 scholarly works according to:
Citing Articles:
IOP Conference Series Earth and Environmental Science (2021) OpenAlex
E. P. Rini, F. Rachman, D. Wirnas, Trikoesoemaningtyas, D. Sopandie - IOP Conference Series: Earth and Environment (2020) Semantic Scholar
M. Rafieazad, A. Chatterjee, A. Nasiri - JOM (2019) Semantic Scholar
JOM (2019) OpenAlex
IOP Conference Series Earth and Environmental Science (2019) OpenAlex Semantic Scholar
M. Pratiwi, H. Sinaga, E. Julianti - IOP Conference Series: Earth and Environment (2019) Semantic Scholar
K. Aljabri, S. Bokhari, Muneera A. Al Shareef, Patan Murthuza Khan - Annals of Saudi Medicine (2018) Semantic Scholar
Journal Of Obesity Management (2017) OpenAlex
Deleted Journal (2016) OpenAlex Semantic Scholar