
Post Mastectomy Pain is No Longer Nightmare
Abstract
Background
PMPS nowadays is common due to advances in both; diagnosis and treatment of cancer breast. Choosing proper treatments can improve the patients’ quality of life. Cancer breast is common and quite important disease and female in our family must be aware of it. Improvement of the diagnosis and treatment PMPS lead to increased patient’s satisfaction and decrease fear of cancer breast.
Objective
Discuss different methods for management of PMPS with less side effects, adequate analgesia, improvement of quality of life, and better patient satisfaction in the future.
Methods
Treatment approaches include both pharmacological interventions and non-pharmacological strategies. However, current treatments of the PMPS are near-optimal and prevention much better than treatment.
Conclusion
Continuous perioperative thoracic epidural Fentanyl–bupivacaine infusion was much better in pain relief, less sedating effect and shorter duration of hospital and ICU stay than continuous perioperative entanyl intravenous infusion in patients undergoing major upper gastrointestinal cancer surgery.
Author Contributions
Academic Editor: Angela Pıa Cazolla, Professor for the Master degree of Dentistry and for the in Pediat Vocational Masters Degree ric Dentistry and Dental Traumatology at University of Foggia, Italy
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Alaa Ali M. Elzohry, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cancer breast is the most common cancer in women and second most common cancer overall. It is the fifth most common cause of death from cancer in women according to International Agency Of Research On Cancer and WHO. There are more than 1.7 million new cases diagnosed worldwide. This represents about 12% of all new cancer cases and 25% of all cancers in women 1.
The risk of breast cancer doubles each decade until menopause, after menopause the risk increase slows. Survival rates for breast cancer vary worldwide, but in general rates have improved. In most countries, the five-year survival rate of early stage breast cancers is 80–90 per cent, falling to 24 per cent for breast cancers diagnosed at a more advanced stage 2.
There are several factors which increase a woman's risk for the breast cancer; such as hyperprolactinemia due to neuroleptics and other dopamine antagonists. Breast cancer subtypes mostly are hormone-related. The natural history of the disease differs between those diagnosed before and after the menopause, which may be due to different kinds of tumors and possibly different effects of nutritional factors on hormones depending on menopausal status. Also, patients with Parkinson's disease have lower rates of malignancies specially breast cancer 3.
Variations observed in rates of incidence and mortality because to breast cancer, are due to a number of factors like age, race, socio-economic status, life style, reproductive history and finally family history 4.
As a consequence of advancements in both diagnosis and treatments, the survival rate patients have increased. So, population susceptible to develop pain as a complication is expected to increase 5. It has been estimated that about 70 percent of new breast cancer cases would be seen by 2020 in developing nations 6.
But although adequate treatment, many patients experience severe pain either from disease progression or from treatment related side effects (like surgery or radiotherapy). And this under managed pain affects negatively physical and psychosocial patients’ lives 6.
Pain arising in advanced stage of breast cancer can cause emotional suffering and affects quality of life of patients 6. As per the estimates of the International Association for the Study of Pain (IASP) the prevalence of pain in breast cancer ranges from 40-89 percent 7.
Breast cancer causes pain due to multiple causes. It may be due to cancer itself, release of inflammatory mediators, and distant spread to other tissues like bones or neuronal tissue or due to different modalities of treatment as chemotherapy which causes degeneration of sensory neurons and lead to neuropathic pain 8. And radiotherapy induce pain as a result of changes which occur at microvascular level and nerve compression The main causes for surgery induced pain are neuroma formation and intercostobrachial nerves damage 9. Finally Estrogen deficiency caused by aromatase inhibitors leads to arthralgias 10.
When we mention different modalities of treatment, we must know that surgery is the keystone in the treatment of solid neoplastic tumors in general including breast cancer. Paradoxically, there is high risk of metastatic spread the perioperative period represents in cancer patients 11. This is due to depression of antitumoral cellular immunity and depression occur in the postoperative period is linked to the metabolic and hormonal changes caused by the “stress reaction” to surgery 12.
‘By any reasonable code, freedom from pain should be a basic human right, limited only by our knowledge to achieve it’ Ronald Melzack13. It is the basic duty of all healthcare professionals to relieve pain, and the most important indication for treating pain after surgery is humanitarian 13. As pain is a nightmare for most patients and influences their overall experience 14.
Usually adequate analgesia is achieved by following the WHO’s step analgesic ladder. As the cancer progresses, the pain experienced by the patient increases. This necessitates the administration adjuvant analgesics with opioids to control this severe pain. Unfortunately, analgesics affect immunity and tumor development by direct interfering with cellular mechanisms (e.g., cell apoptosis) or indirect interacting with the sympatho-adrenal systems 15 .
Persistent pain after mastectomy is common and about 20-50 percent women are complaining of persistent neuropathic pain after mastectomy 16. More common among young patients, those undergoing radiotherapy and axillary lymph node dissection 17.
There is a strong evidence that; suppression of the immune system in the perioperative period increase postoperative complications which includes bad wound healing infections leading to sepsis, multiple organ failure and death 18. Also the development of residual malignant cells and the formation of new metastases are accelerated by immune suppression 19.
Other concerns of the anesthesiologists are prevention of post operative pain and suppression of the surgical stress response. Stress responses to surgical trauma and postoperative pain elicit diffuse changes in the hormonal secretion of cortisol and prolactin 20.
So this review aimed to summarize the different perioperative methods to prevent post mastectomy pain because Aggressive perioperative pain prevention can yield both short-term and long-term benefits as unrelieved pain affects patient recovery, prolongs hospital stays, increases hospital morbidity, and adds to the burden of growing health-care costs 21.
Post Mastectomy Pain Syndrome (PMPS)
PMPS first by reported by Wood in late 1970, and then Folly et al described PMPS as pain and sensory disorders following mastectomy. Post-mastectomy pain syndrome is described as a chronic neuropathic pain which caused by damage of the multiple nerves, and occurred after all types of breast cancer surgery (radical mastectomy, modified radical mastectomy, and lumpectomy associated with axillary lymph node dissection) 22. It represents about 25%-60% of patients suffer from chronic pain after breast cancer-related surgery 23.
Damage to the intercostobracial nerve is the most common cause of PMPS. Unfortunately, the risk of damage to the intercostobrachial nerve during breast conserving surgery is equivalent to that which occurs during complete mastectomy. This is due to a wide variation in the size, location and branching of the intercostobrachial 24.
Pain features (neuropathic) are burning like sensation, paroxysmal lancinating pain, shock-like, and pinprick pain 25.
The pain decreases everyday activities, social function and causes heavy economic burden for the healthcare system 26. Several factors make PMPS persistent, like adjuvant therapy, psychosocial status, preoperative breast pain, type of surgery and type of analgesia. Being a problem of such important, should increase attention to PMPS 27.
The pain is perceived mainly in the axilla, medial upper arm, breast, and chest wall after more than three months of surgery to eliminate all other causes of pain such as infection (Figure 1)28, 29.
Figure 1.location of PMPS 29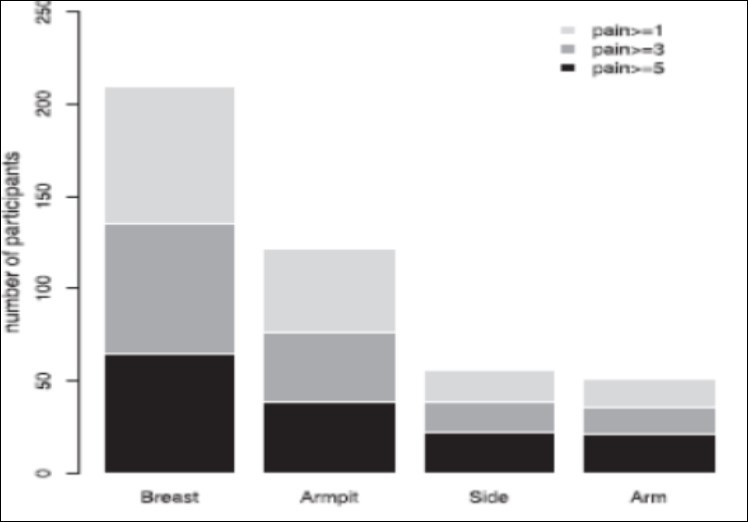
Many mechanisms explain PMPS such as; tissue injury, nerve damage related to surgery, and neuroma pain. Different types of sensory disturbances (e.g., numbness) are sequelae to surgical intervention and an important part of the pain characteristics 30.
PMPS can be related to the patient or the surgery itself. Among patient-related factors, the younger age was proved to be a high risk for the development of PMPS, and these findings are consistent with previous literature 31.
Many explanations have been proposed, including (1) these age group were subjected to more aggressive use of adjuvant therapies; (2) pain perception decrease with age; (3) negative estrogen receptor status; (4) greater surgical invasion in axillary dissection. For axillary clearance is more difficult because of plenty fatty tissue, the researchers consider high BMI as a risk factor for PMPS, but no evidence prove this finding 32.
Consequences of Undermanaged PMPS
PMPS is a form of neuropathic pain caused by surgical trauma and is associated with an inflammatory reaction that has many consequences involving multiple organ systems, including local and systemic effects 33.
Sympatho-Adrenal and Metabolic Stress Responses
Surgical trauma leads to a cascade of endocrine and metabolic effects and release of inflammatory mediators and pro-inflammatory cytokines including interleukin 1 (IL-1), IL-6, and tumor necrosis factor (TNF). It also decreases in anti-inflammatory cytokines such as IL-10 33.
The clinical consequences of these changes include immune suppression, hypothermia, and thromboembolic complications among others. In addition to an inflammatory response, acute postoperative pain can also induce endocrine metabolic changes. These changes induce a catabolic response with clinical consequences including loss of muscle mass, impaired wound healing and ileus 34.
Cardiovascular System
Post mastectomy pain causes a global sympathetic response capable of increasing heart rate, peripheral vascular resistance, blood pressure, and subsequently cardiac output. This sympathetic cascade can increase the oxygen demand of the myocardium and potentiate myocardial ischemia, especially in patients with preexisting coronary artery disease 35.
Respiratory System
Pain from surgery to the chest or abdomen often results in splinting of the muscles of the diaphragm and chest wall 35. This leads to decreased lung vital capacity, forced expiratory volume and functional residual capacity.
Musculoskeletal System
Immobility due to PMPS causes venous stasis and increases the risk of deep vein thrombosis. Also, vasoconstriction because of pain can lead to muscle wasting which can be debilitating. This leads to prolonged stay in the hospital and rehabilitation facilities. 35
Psychological Effects
Anxiety, depression, fear, sleeplessness, and fatigue are increased due to poor pain control. In turn, sleep deprivation can decrease the effectiveness of pain therapy. Strong evidence suggests that depression and anxiety modulate activity in the dorsal horn, through the descending pathways and change pain perception 36.
Chronic Pain
Untreated acute post mastectomy pain can be changed to chronic pain and this was proved by multiple studies. 36 Up regulation of peripheral nociception and increased nerve excitability due to prolonged exposure to noxious stimuli are the possible mechanisms. Noxious stimuli sensitize the nervous system response to subsequent stimuli. This is known as “windup” or “central sensitization” and is further illustrated in (Figure 2)37.
Figure 2.Noxious stimuli can sensitize the nervous system response to subsequent stimuli 37
Discussion
According to a previous review, the literature was inconsistent in defining chronic pain after mastectomy 38. To improve comparability between studies in the future, Jung et al suggested a time frame definition of chronic neuropathic syndrome classification based on the etiology.
The authors suggested that neuropathic pain syndromes due to breast surgery are considered chronic after 3 months and that shorter time frames should raise a consideration of pain associated with tumour recurrence. In Jung et al’s review, there were approximatly 21 studies with follow-up periods from 1-96 months which revealed the following:
Phantom breast pain prevalence is (3-44) per cent;
Intercostobrachial neuralgia (ICN) 16-39 percent for all breast cancer surgery;
Neuroma pain prevalence is (23-49) percent. 38
There were many trials (randomized, doubled-blinded, placebo-controlled) done to investigate the best neuropathic pain treatment algorithm. Many trials were included studying a lot of neuropathic conditions. The most studied oral medications were; anti-depressants, anticonvulsants, opioids, NMDA antagonists, mexilitine, topical lidocaine, cannabinoids, topical capsaicin, and glycine antagonist.
We here mention the most effective methods for controlling PMPS that were published in last few years:
One prospective randomized controlled clinical study was done in South Egypt Cancer Institute, titled (Analgesic efficacy of pregabalin in acute postmastectomy pain: placebo controlled dose ranging study) that published in Journal of Clinical Anesthesia, 2016. The conclusions was a single preoperative oral dose of pregabalin 150 mg is an optimal dose for reducing postoperative pain and morphine consumption in patients undergoing MRM 40.
Another important method is paravertebral block, as proved by study by Brian M. et.al. That published in 2015 and concluded that "Adding a multiple-day, continuous Ropivacaine infusion to a single-injection ropivacaine paravertebral nerve block may result in a decreased incidence of pain and pain-related physical and emotional dysfunction for 1 year after mastectomy 41.
Also, Pecs block (pectoral nerves block) which is an easy and reliable block inspired by the infra clavicular block approach and the intercostal abdominis plane blocks. Its technique as following, the pectoralis muscles are located under the clavicle then the space between the two muscles is dissected to reach the lateral pectoral and the medial pectoral nerves. The main indications are breast expanders and subpectoral prosthesis because the distension of these muscles is very painful 42.
A second version of the Pecs block was described, called ‘‘modified Pecs block’’ or Pecs block type II. This novel approach aims to block at least the pectoral nerves, the intercostobrachial, intercostals III-IV-V-VI and the long thoracic nerve. These nerves must be blocked to provide complete analgesia during breast surgery (Figure 3) 43.
Figure 3.anatomy of pectoral muscle
In a study published 2012 in Elsevier Doyma ‘‘modified Pecs’s block’’ or Pecs block type II was described. Using Ultrasound images that was very conclusive as the contrast was taken up by the axilla and reaches the thoracodorsal nerve area, passing above the serratus muscle and hence, the long thoracic nerve, was anesthetized with the clinical usefulness. This approach aims to block the axilla that is vital for axillary evacuation and the intercostal nerves, necessary for wide local excisions of the tumor. Two needle approaches used to perform the Pecs II block or ‘‘modified Pecs’s block’’ instead of one 44.
We must know that, Thoracic epidural and paravertebralblocks became the gold standard techniques to achieve this goal, but not every anesthesiologist is comfortable performing these procedures (Figure 4) 45.
Figure 4.U/S guided Thoracic epidural and paravertebral blocks 43
Other interventional method "interscalene brachial plexus block" which was proved by Kaya M et al, 2013 who evaluated the effects of interscalene brachial plexus block on postoperative pain relief and morphine consumption after modified radical mastectomy (MRM). Sixty ASA I–III patients scheduled for elective unilateral MRM under general anesthesia were included. Pain intensity was assessed with the visual analogue scale (VAS). Other parameters as morphine consumption, side effects of opioid, antiemetic requirement, and complications associated with interscalene block were recorded.VAS scores were significantly lower in interventional group, except in the first postoperative 24 h (p < 0.007). The patients without block consumed more morphine (group 1, 5 (0–40) mg; group 2, 22 (6–48) mg; p = 0.001) 46.
Until now paravertebral blocks and thoracic epidurals are the most effective and the gold standard pain treatment for breast cancer surgery. However, we questioned the effectiveness based on the fact that the brachial plexus nerves are the main component of this painful surgery and we described for the first time the use of pectoral nerve blocks with this indication 47.
We cannot ignore role of non-pharmacological methods of pain relief as preoperative explanation, education and Physical therapy techniques. As one of the best review that illustrated in detail effectiveness of postoperative physical therapy for upper-limb impairments after breast cancer treatment published in 2015 with the following recommendations 48:
1) First week post-op: low-intensity program involving elbow/wrist
2) 7-10 days post-op: gradually increase intensity passive mobilization (manual stretching, active exercises and increase muscle strength)
3) No recommendations can be made on length of time, content, intensity
4) Multifactorial therapy consisting of manual stretching and active exercises effectively treated impaired shoulder ROM 48.
2-Relaxation therapy
3-Hypnosis
4-Cold or heat
5-Splinting of wounds
6-Transcutaneous electrical nerve stimulation (TENS).
And sure the pharmacological methods of pain relief according to the ‘analgesic ladder’ introduced for treatment of cancer pain by the World Health Organization (WHO). It is formed of three steps according to intensity of pain. The first step involves the use of non-opioid +/- adjuncts (e.g. paracetamol, aspirin or non-steroidal anti-inflammatory drugs (NSAIDs). If pain is still uncontrolled, in addition to step 1 medication weak opioids (e.g. codeine, tramadol) can be added 49.
In moderate to severe pain or pain increasing in spite of step 2 treatment, stronger opioids are considered in addition. All these involve the concept known as multimodal analgesia. It is important to include the analgesic ladder in individual patient analgesic plan along with the adjunctive therapies. The analgesics act at different sites. Drugs that act at the site of injury and decrease pain associated with inflammatory reaction (e.g. NSAIDs), other drugs may alter nerve conduction (e.g. local anesthetics), some may modify transmission in the dorsal horn (e.g. opioids and antidepressants) while group of drugs may affect the central component and the emotional aspects of pain (e.g. opioids and antidepressants) 49.
Fourth step was added to WHO analgesic ladder which was interventional pain management such as stellate ganglion block (radiofrequency thermal neuro modulation) or local anesthetic injection of stellate ganglion block). Intervention pain management was advised to be done early before tumor spread or patient became deteriorated 51.
Opioid use could be associated with an increased incidence of opioid-related adverse drug events, including over sedation and respiratory depression 50. Further study are needed because opioid-related adverse drug events have been associated with an increase in overall cost, length of stay, and even decreased survival during in-hospital resuscitation 51.
It is frequently not possible to administer sufficient opioids alone, due to coexisting medical conditions, patient tolerance, allergies, or efforts to reduce total opioid use. In such cases, a multimodal approach to intravenous pain management must be employed. This may include the use of opioids, NSAIDS, and other adjuvant as needed to optimize patient pain control in the immediate postoperative period as a bridge until the patient can be transitioned to less potent oral medications 52.
And finally Minimizing damage to nerves during surgery Improved screening methods detect breast cancer at earlier stages. Earlier detection means smaller tumour sizes, which has made breast-conserving surgical treatments possible and widely used. These currently account for up to 40 per cent of breast cancer surgery 53.
Breast conserving techniques include lumpectomy, conservative breast surgery, wide local excision, partial mastectomy, segmentectomy, or tylectomy. Such approaches include reducing the number of axillary dissections required. Combining reduced surgical trauma with nerve preservation techniques may reduce the risk of sensory deficits and the occurrence of ICN 54, 55.
In this regard, the increased use of less invasive staging techniques such as sentinel lymph node biopsy has helped to reduce the number of patients undergoing axillary dissection and the resulting trauma to intercostobrachial nerves 56.
Conclusion
PMPS nowadays is frequency due to advances in diagnosis and treatment of breast cancer. Choosing proper treatments can improve the patients’ quality of life. Cancer breast is common and important disease to female in our family and all female must be aware of it, Improvement of the diagnosis and treatment of patients with breast cancer lead to increased incidence rate of PMPS. Treatment approaches include both pharmacological interventions and non-pharmacological strategies.
However, current treatments of the PMPS are near-optimal and prevention much better than treatment. Further investigations are required to achieve the appropriate developments in diagnosis and screening of breast cancer, and evaluation and treatment of PMPS that will provide less side effects, adequate analgesia, and finally, improved quality of life, and patient satisfaction in the future.
Ethical Issues
Not applicable.
Financial Support
None.
Acknowledgment
Praise to ALLAH who has guided us to this, never could it be done without the help of ALLAH.
I would like to express my deep thanks to all my colleagues, members of anesthesia, intensive care and pain management department in south Egypt cancer institute who kindly helped me in achieving this work.
I would like to immense gratitude and appreciation to my friend Rachel (Special Issue Manager) and all Editorial Office for great help in this work.
References
- 1.World cancer research -http://www.wcrf.org/int/cancer-facts-figures/ data-specific-cancers/breast-cancer-statistics Tel: +44-20-73434200 Fax: +44-20-73434220 The GLOBOCAN estimates are presented for 2012 estimates of the incidence of, mortality and prevalence of breast cancer.2012.
- 2.Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S et al. (2012) International Agency for Research on Cancer;. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet] , Lyon, France: .
- 3.Handy C R, Krudy C, Boulis N. (2011) Gene therapy: a potential approach forcancer pain. Pain Res Treat.;2011:. 987597.
- 4.GLOBOCAN 2008,Cancer Fact Sheet. Breast Cancer Incidence and Mortality Worldwide in2008.[accessed onJuly20,2011].
- 5.Jung B F, Ahrendt G M, Oaklander A L, Dworkin R H. (2003) Neuropathic pain following breast cancer surgery: proposed classification and research update. Pain.;104: 1–13
- 6.International Associationfor the Study of Pain, Psychosocial Interventions for Cancer Pain. [accessed onJuly20,2011].
- 7.Miaskowski C, Dibble S L. (1995) The problem of pain in outpatients with breast cancer. Oncol Nurs Forum.;22:. 791-7.
- 8.International Associationfor the Study of Pain, Mechanisms of Cancer Pain. [accessed on:July20,2011]
- 9.Jung B F, Ahrendt G M, Oaklander A L, Dworkin R H. (2003) Neuropathic pain following breast cancer surgery: proposed classification and research update. Pain.;104: 1-13.
- 10.Mao J J, Stricker C, Bruner D, Xie S, Bowman M A et al. (2009) Patterns and risk factors associated with aromatase inhibitor-related arthralgia among breast cancer survivors. Cancer.;115:. 3631-9.
- 11.Shakhar G, Ben-Eliyahu S. (2003) Potential prophylactic measures against postoperative immunosuppression: could they reduce recurrence rates in oncological patients? Ann Surg Oncol;10:. 972-92.
- 12.Wrona D. (2006) Neural-immune interactions: an integrative view of the bidirectional relationship between the brain and immune systems. , J Neuroimmunol; 172, 38-58.
- 13.Macintyre P E, Schug S A, Scott D A. (2010) APM: SE Working Group of the Australian and New Zealand College of Anesthetists and Faculty of Pain Medicine. Acute Pain Management. Scientific Evidence (3rd edition), ANZCA & FPM. , Melbourne;
- 14.Niraj G, Rowbotham J. (2011) Persistent post-operative pain: where are we now?. , Br J Anaesth; 107, 25-29.
- 15.Forget P, Machiels J-P, Coulie P G. (2013) Neutrophil:lymphocyte ratio and intraoperative use of ketorolac or diclofenac are prognostic factors in different cohorts of patients undergoing breast, lung and kidney cancer surgery. Ann Surg Oncol.
- 16.Gärtner R, Jensen M B, Nielsen J, Ewertz M, Kroman N et al. (2009) Prevalence of and factors associated with persistent pain following breast cancer surgery. , JAMA.; 302, 1985-92.
- 17.Bokhari F, Sawatzky J A. (2009) Chronic neuropathic pain in women after breast cancer treatment. , Pain Manag Nurs 10, 197-205.
- 18.Kurosawa S, Kato M Anesthetics. (2008) immune cells, and immune responses. , Anesth J; 22, 263-277.
- 19.Kumar S, Gupta R, Kaleem A M.(Jan18,2014) Mitigation of pain and anaesthetic drugs. , OA Anaesthetics 2(1), 2.
- 20.Solak M, Ulusoy H, Sarihan H. (2000) Effects of caudal block on cortisol and prolactin responses to postoperative pain in children. , Eur J Pediatr Surg; 10, 219-223.
- 21.Miaskowski C, Crews J, Ready L B. (1999) Anesthesia-based pain services improve quality of postoperative pain management. , Pain; 80, 23-9.
- 22.Mejdahl M K, Andersen K G, Gärtner R, Kroman N, Kehlet H. (2013) Persistent pain and sensory disturbances after treatment for breast cancer: six year nationwide follow-up study. doi: 10.1136/bmj.f1865. , BMJ: 346, 1865.
- 23.Abdel Dayem OT, Saeid M M, Ismail O M, El Badrawy AM, Abdel Ghaffar NA. (2014) Ultrasound guided stellate ganglion block in postmastectomy pain syndrome: a comparison of ketamine versus morphine as adjuvant to bupivacaine. , Journal of Anesthesiology.;2014: 792569.
- 24.Pekka M, Kairaluoma. (2006) Revista espanola de anestesiologia y reanimacion 58(5):. , Anesth Analg 103, 290-294.
- 25.Vecht C, Brand H Van de, Wajer O. (1989) Post-axillary dissection pain in breast cancer due to a lesion of the intercostobrachial nerve.Pain. 38, 171-6.
- 26.Couceiro T C D M, Menezes T C De, Valˆenc¸a M M. (2009) Post mastectomy pain syndrome. The magnitude of the problem,”Revista Brasileira de Anestesiologia 59(3), 358-365.
- 27.Peuckmann V, Ekholm O, N K Rasmussen. (2009) Chronic pain and other sequelae in long-term breast cancer survivors: nationwide survey in Denmark. , European Journal of Pain 13(5), 478-485.
- 28.Bokhari F, Sawatzky J A. (2009) Chronic neuropathic pain in women after breast cancer treatment. , Pain Manag Nurs 10, 197-205.
- 30.Mejdahl M K, Andersen K G, Gartner R, Kroman N, Kehlet H. (2013) Persistent pain and sensory disturbances after treatment for breast cancer: six year nationwide follow-up study. British Medical Journal.Article Idf1865 346.
- 31.K G Andersen, Kehlet H. (2011) Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. , Journal of Pain 12, 725-746.
- 32.Kehlet T S Jensen H, C J Woolf. (2006) Persistent postsurgical pain: risk factors and prevention. , The Lancet 367(522), 1618-1625.
- 33.Cousins M, Power I. (1999) Acute postoperative pain. Textbook of pain. 4th ed. Edinburgh: Churchill Livingstone; In Wall PD, Melzack R, editors 447-91.
- 34.Kehlet H, Dahl J B. (2003) Anaesthesia, surgery, and challenges in postoperative recovery. , Lancet; 362, 1921-8.
- 35.Macintyre P E, Schug S A, Scott D A. (2010) APM: SE Working Group of the Australian and New Zealand College of Anesthetists and Faculty of Pain Medicine. Acute Pain Management. Scientific Evidence (3rd edition), ANZCA & FPM. , Melbourne;
- 36.Apfelbaum J L, Chen C, Mehta S S. (2003) Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. , J Anesth Analg; 97(2), 534-540.
- 37.Gottschalk A, Smith D S. (2001) New concepts in acute pain therapy: preemptive analgesia. , Am Fam Physician; 63(10), 1979-85.
- 38.Jung B. (2003) Neuropathic pain following breast cancer surgery: proposed classification and research update.Pain,104:p.1-13.Hetta et al Analgesic efficacy of pregabalin in acute postmastectomy pain: placebo controlled dose ranging study. , Journal of Clinical Anesthesia2016 34, 303-309.
- 39.Brian. (2015) Persistent Postmastectomy Pain and Pain-Related Physical and Emotional Functioning With and Without a Continuous Paravertebral Nerve Block: A Prospective 1-Year Follow-Up Assessment of a Randomized, Triple-Masked. , Placebo-Controlled Study Ann Surg Oncol 22, 2017-2025.
- 40.Blanco R. (2011) Bloqueo pectoral (Pecs Block). Manual de anesthesia regional y econoanatomía avanzada. Capítulo 4.Madrid:Editorial Ene. isbn: 978-84.
- 41.Klein S M, Bergh A, Steele S M, Georgiade G S, Greengrass R A. (2000) Thoracic paravertebral block for breast surgery. Anesth Analg;90:. 1402-5.
- 42.Kehlet H, T S Jensen, C J Woolf. (2006) Persistent postsurgical pain: risk factors and prevention. 367(9522), 1618-1625.
- 43.Norum H M, Breivik H. (2011) Thoracic paravertebral blockade and thoracic epi- dural analgesia: two extremes of a continuum. , Anesth Analg 112, 990.
- 44.Kaya M. (2013) Postoperative analgesia after modified radical mastectomy: the efficacy of interscalene brachial plexus block. , Journal of anesthesia December 27(6), 862-867.
- 45.Smith H S, Wu S-X. (2013) Persistent pain after breast cancer treatment. , Ann Palliat 1(3), 182-194.
- 46.DeGroef A. (2015) Effectiveness of Postoperative Physical Therapy for Upper-Limb Impairments After Breast Cancer Treatment: A Systematic Review Archives of Physical Medicine and Rehabilitation;. 96, 1140-53.
- 48.Manchikanti L, Fellows B, Ailinani H. (2010) Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. , Pain Physician; 13, 401-435.
- 50.Fecho K, Jackson F, Smith F. (2009) In-hospital resuscitation: opioids and other factors influencing survival. , Ther Clin Risk Manag; 5, 961-968.
- 51.Barton J, Stuart G A. (2012) Outcome studies and infection control in regional anesthesia. Essentials Regional Anesth:. 741-777.
- 52.Rietman J. (2006) Long term treatment related upper limb morbidity and quality of life after sentinel lymph node biopsy for stag I or II breast cancer.European Journal of surgical oncology. 32, 148-52.
- 53.Mansel R. (2006) Standard Axillary Treatment in Operable Breast Cancer:. The ALMANAC trial.Journal of National Cancer Institute 98(9), 599-609.
- 54.Peintinger F. (2003) Comparison of quality of life and arm complaints after axillary lymph node dissection vs sentinel lymph node biopsy in breast cancer patients.British. , Journal of Cancer 89, 648-52.
Cited by (16)
This article has been cited by 16 scholarly works according to:
Citing Articles:
Hanane Barakat, Rony Al Nawwar, Linda Gholmieh, Caroline Chahine, Mariam Karake et al. - Saudi Journal of Anaesthesia (2025) Semantic Scholar
Journal of Cellular and Molecular Anesthesia (2025) Crossref
Deleted Journal (2025) OpenAlex
Aesthetic Surgery Journal (2023) Crossref
Aesthetic Surgery Journal (2023) OpenAlex
Krzysztof Nosek, W. Leppert, Łukasz Puchała, Krzysztof Łoń - Pharmaceutics (2022) Semantic Scholar
S. Otto, R. Schleip, V. Fink, A. Bayat - 64. Kongress der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe e. V. (2022) Semantic Scholar
Geburtshilfe und Frauenheilkunde (2022) Crossref
Geburtshilfe und Frauenheilkunde (2022) OpenAlex
A. Chappell, Selcen S. Yuksel, D. Sasson, Annie B. Wescott, Lauren M. Connor et al. - JPRAS Open (2021) Semantic Scholar
JPRAS Open (2021) Crossref
JPRAS Open (2021) OpenAlex
L. C. Martínez - (2020) Semantic Scholar
Revista de la Sociedad Española del Dolor (2020) OpenAlex
Irwan Setiadi, M. A. Prihartono, Erwin Pradian - (2020) Semantic Scholar
A. Chappell, J. Bai, Selcen S. Yuksel, M. Ellis - World journal of plastic surgery (2020) Semantic Scholar
WORLD JOURNAL OF PLASTIC SURGERY (2020) OpenAlex