Abstract
Objective:
This study assessed the baseline knowledge, perceptions, attitudes and behaviors of prediabetes patients in order to tailor a new technology-enhanced primary care-based lifestyle modification intervention.
Methods:
Patients with a diagnosis of prediabetes were enrolled in a randomized, controlled pilot study, Avoiding Diabetes Thru Action Plan Targeting (ADAPT), a technology-based intervention to promote action plan discussions around patient-selected behavior change goals.
Results:
A total of 54 adults (82% female) were enrolled in the pilot study. Most (89%) had comorbid conditions and mean BMI was 36. Participants exhibited significant levels of diabetes risk knowledge and diabetes risk perception, as well as high levels of willingness to make changes to decrease diabetes risk. Number of daily steps was inversely correlated with perceived physical activity (r=-0.35082, p<0.001). Poorer scores on diet quality were inversely correlated with BMI.
Conclusion:
Participants in this sample demonstrated requisite levels of knowledge, self-efficacy, motivation and risk perception for effective behavior change. These data suggest that primary care-based prediabetes interventions can move beyond educational goals and focus on enhancing patients’ ability to select, plan and enact action plans.
Author Contributions
Academic Editor: Wei Wang, Professor, School of Medical Sciences, Edith Cowan University, Australia; Professor/Director, Beijing Municipal Key Laboratory of Clinical Epidemiology and Capital Medical University, Beijing, China.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2014 Jennifer M Kolb, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
In the United States, 25.8 million adults have type 2 diabetes mellitus (T2DM), and another 79 million adults are affected by prediabetes.1 Data from the 2007-2009 National Health Interview Survey and National Patient Information Reporting System reveal a disproportionately higher prevalence of diabetes among African Americans, Hispanics, and Asian Americans.2 The rising incidence of diabetes in the US is a public health concern with serious medical and financial implications. In 2012, the cost of diabetes in the US was estimated at $245 billion.3
Without intervention, individuals with prediabetes are at high risk of developing diabetes and associated comorbid complications. Prediabetes alone has also been associated with increased risk of cardiovascular disease,4, 5, 6, 7 chronic kidney disease,8 retinopathy,9 and neuropathy.10
Lifestyle changes in patients with elevated glucose levels are known to delay or prevent the progression of prediabetes to T2DM.11, 12 Effective interventions include changes in diet alone, exercise alone, diet plus exercise, and weight loss.13, 14 The Diabetes Prevention Program (DPP) demonstrated that a structured, intensive program of dietary and exercise counseling combined with a weight loss regimen effectively reduced the risk of developing T2DM by 58% over three years and was more effective than metformin in reducing risk of diabetes, with protective benefits persisting for at least 10 years.15, 16, 17, 18, 19 The efficacy of diabetes intervention programs has also been demonstrated in primary care settings.
Patient factors such as a lack of willingness to change, low self efficacy, poor disease understanding, and inappropriate perception of risk are often cited as key obstacles to successful execution of behavior change programs in primary care.20, 21 Challenges described include participants’ mixed levels of knowledge regarding whether diabetes can be prevented and little knowledge of risk factors.22 Providers note an absence of patient motivation to change their unhealthy habits as an important barrier for effective lifestyle counseling.23 Since diabetes is largely a self-managed disease, patients’ social support, access to care, financial barriers, and attitudes and beliefs about their illness are crucial components that determine individual health behaviors. Pre-existing physical conditions and social demands can act as impediments to behavior change and necessitate a holistic approach to lifestyle intervention.24
Comprehensive lifestyle interventions like the DPP have the time and resources to intervene on all of these factors: educational, motivational and behavioral. However, primary care provider-led interventions must be more focused and smaller in scope. This creates some confusion as to where emphasis should be placed for behavior change. Do prediabetes patients in primary care have enough knowledge to enact behavior change plans, or do interventions first need to focus on improving knowledge, attitudes and beliefs about their disease and risk for diabetes? Can interventions presume sufficient levels of these factors among patients, and instead focus on tools to enable them to achieve their behavioral goals? This study seeks to answer these questions and evaluate the baseline knowledge, attitudes, beliefs and behaviors of prediabetes patients in a primary care setting in order to guide the focus, development and implementation of a technology-enhanced lifestyle intervention.
Methods
A randomized, controlled pilot study, Avoiding Diabetes Thru Action Plan Targeting (ADAPT), introduced a novel tool to enhance physician counseling for patients with prediabetes in the primary care setting. The full details of the study design have been previously published, but in brief, the ADAPT system uses the electronic medical record, pedometers and the internet to embed prediabetes-specific action planning into primary care encounters.25 Patients were recruited from two urban, academic primary care practices, both affiliated with the Mount Sinai Hospital in New York. Recruitment followed practical trial methods such that patients were recruited from practice databases and all study procedures were situated within the context of previously scheduled clinical visits.26 Patients were eligible if they were age 18 or older, English-speaking, and had prediabetes defined as having a glycosylated hemoglobin (A1C) of 5.7-6.4% (40-48mmol/mol) or a fasting glucose of 100-125. Patients were excluded if they had a diagnosis of diabetes, had ever been prescribed a diabetic medication, were unable to walk, or did not have access to email since part of ADAPT involves email-based communication. Eligible patients from each practice were approached via phone by trained research assistants and invited to participate in the study. Patients who expressed interest in participating over the phone and wanted additional information were subsequently sent a follow-up email with an attached consent form. Patients who were sent an email received an additional follow-up phone call to schedule a meeting to officially enroll in the study by signing the consent form and receiving a pedometer.
All study activities were conducted within the context of real clinical activities and were scheduled around or within upcoming primary care visits. As such, all participants completed a 60-item multiple-choice pre-enrollment survey administered by a research assistant by telephone or in-person prior to their primary care visit. Items included socio-demographics, medical history, and family history. Participants were asked about current physical activity and attempts to change physical activity. Similar questions were asked about individual body weight. In addition to inquiring about confidence/self-efficacy to change eating habits and physical activity, the survey assessed participants’ current stage of change in these behaviors according to the Transtheoretical Model of Stages of Change.27 Pre-diabetes risk knowledge and T2DM risk perception were measured as well using subscales of the Risk Perception Survey-Developing Diabetes (RPS-DD).28, 29 Symptoms of depression and anxiety were assessed using the Patient Health Questionnaire (PHQ-8) and the General Anxiety Disorder (GAD-2) scale, respectively.30, 31 Participants answered questions related to the locus of responsibility for making changes to their lifestyle and the effectiveness of their provider in helping them change behaviors. Finally, self-reported diet behavior was assessed using the short Rapid Eating Assessment for Patients (REAP-S) tool, a 16-item instrument to address dietary intake and behavior.32, 33
Participants were required to wear a pedometer (portable activity monitor, Omron HJ-720ITC) to measure their daily steps for one week prior to their first study visit. To be considered valid, a participant’s pedometer data needed to consist of (1) at least 10 hours of non-zero activity per day and (2) at least 3 days of activity.41 Hours of activity and days worn could be continuous or interrupted. Steps-per-day were then calculated for each patient for each valid day. On average, participants wore the pedometer for 5 weekdays and 1 weekend day for final analyses. At the initial baseline visit, height, A1C, and fasting lipid panels were measured.
This study was approved by the Institutional Review Board of the Mount Sinai Hospital.
Statistical Analysis
Descriptive statistics were performed for all baseline characteristics. Univariate analysis was performed to evaluate the association between number of daily steps, body mass index (BMI, kg/m2), stages of change, level of physical activity, Rapid Eating Assessment for Participants (REAPS) score, diabetes knowledge, and diabetes risk perception. For all tests, a p-value less than 0.05 was used for statistical significance. Data analyses were conducted using SAS (v9.1) software for Windows (SAS Institute, Cary, North Carolina).
Results
Socio-Demographics
A total of 63 patients were enrolled in the study. Five individuals presented with a baseline A1C less than 5.7 or greater than 6.4 and four individuals failed to complete all entry requirements leaving 54 participants for final analyses (Table 1).
Table 1. Baseline socio-demographic and clinical characteristics of participants enrolled in ADAPT (Avoiding Diabetes Thru Action Plan Targeting)| Variable | Overall (N= 54) |
|---|---|
| Mean age (in years) (SD) | 45.7 (10.9) |
| Gender | Female = 44 (81.5%) |
| Race | |
| White | 6 (11.1%) |
| Black | 21 (38.9%) |
| Hispanic | 22 (40.7%) |
| Asian | 4 (7.4%) |
| Insurance | |
| Any Medicaid | 9 (17.6%) |
| Any Commercial | 41 (80.4%) |
| Only Medicare | 4 (7.8%) |
| Education | |
| ≤ HS degree | 10 (18.5%) |
| Some college | 21 (38.9%) |
| College graduate | 22 (40.7%) |
| Mean Weight (kg) (SD) | 96.2 (23.0) |
| range = 59.4 – 153.3 | |
| Mean BMI (kg/m 2 ) ( SD) | 35.7 (8.3) |
| Mean A1C (SD) | 5.9 (0.2) |
| mmol/mol | 40-48 |
| Lipids (mean (SD)) | |
| Total Cholesterol (normal < 200) | 187 (33) |
| LDL (normal < 100) | 110 (27) |
| HDL (normal > 60) | 56 (14) |
| TG (normal < 150) | 111 (77) |
| In general how is your health? N (%) | |
| Excellent/Very Good | |
| Good | 11 (20.8%) |
| Fair/Poor | 28 (52.8%) |
| 13 (26.4%) | |
| Comorbidities | |
| 0 | 6 (11.1%) |
| 2-Jan | 28 (51.9%) |
| 3+ | 20 (37.0%) |
| Family History of Diabetes | |
| Yes | 41 (75.9%) |
| PHQ-8 (mean) | 4 |
| GAD-2 (anxiety) | |
| Not at all | 29 (61.7%) |
| Several days | 14 (29.8%) |
| Nearly every day | 4 (8.5%) |
| GAD-2 (worrying) | |
| Not at all | 33 (67.3%) |
| Several days | 6 (12.2%) |
| Nearly every day | 10 (20.4%) |
Table 1 displays the socio-demographic and clinical characteristics of our sample. Most participants were female (82%) and either Black (39%) or Hispanic (41%), which was representative of the urban primary care practice from which they were recruited. Prediabetes was an isolated condition in only 11% of the sample, while co-morbid hypertension (45%), hyperlipidemia (29%), and arthritis (30%) were common. Most participants reported a family history of diabetes (76%), in addition to numerous friends with diabetes (74%). Eighty-one percent had some college education and 70% reported an annual income over $30,000. Mean BMI was nearly 36 (SD 8.3) and mean A1C was 5.9 (SD 0.2) (40-48mmol/mol).
Knowledge/attitudes
Table 2 displays measures of participant knowledge, attitudes, and perceptions. Participants were knowledgeable about their health and about prediabetes, with 88.9% scoring ‘high’ in risk knowledge (‘low risk’ to ‘slight risk’ being “low risk” and ‘moderate risk’ to high risk’ being “high risk” for both knowledge and perception scores).34 Participants also recognized the hardship diabetes would place on them (88% reporting life with diabetes would be “difficult”). They understood that being overweight, having low levels of physical activity, and having a family history of diabetes increase their chances for developing diabetes. They also recognized that lifestyle changes, including weight loss and exercise, could lower their risk for diabetes. Overall, patients exhibited positive mental health attitudes with no symptoms of depression, and over 60% reported that they are not at all anxious or worried on any given day.
Table 2. Baseline cognitive characteristics of participants enrolled in ADAPT (Avoiding Diabetes Thru Action Plan Targeting)| Stages of change, N (%) | ||||||||
| Pre-contemplation | Contemplation | Preparation | Action | Maintenance | ||||
| Diet | 2 (3.8%) | 11 (21.2%) | 24 (46.2%) | 11 (21.2%) | 4 (7.7%) | |||
| Exercise | 0 (0.0%) | 3 (6.0%) | 20 (40.0%) | 20 (40.0%) | 7 (14.0%) | |||
| Low | Average | High | ||||||
| 5-year risk perception (maximum 28)Compared to other people your age, your risk of getting diabetes over the next 5 years is… | 4 (8.3%) | 18 (37.5%) | 26 (54.2%) | |||||
| Complications (maximum 32)If you had diabetes the chance of having a complication like a heart attack or stroke is… | 31 (67.4%) | 3 (6.5%) | 12 (26.1%) | |||||
| Mean Self-Efficacy | ||||||||
| Diet (0-10 scale)How confident are you that you can successfully change your eating to prevent diabetes? | 7.7 | |||||||
| Exercise (0-10 scale)How confident are you that you can successfully change your physical activity to prevent diabetes? | 7.7 | |||||||
Participants demonstrated appropriate risk perception, with 85.2% recognizing they were at high risk of developing diabetes. The majority (78%) reported being worried about getting diabetes and felt that with diabetes they would be likely to have a complication such as a heart attack or stroke. However, they recognized that they were not invariably destined to have diabetes and overall felt that they could do something to stop the progression to diabetes.
Participants reported dissatisfaction with their current level of physical activity. Over half considered themselves to be somewhat active (59%), though nearly everyone desired to be more active (94%). Similarly, 92% of patients considered themselves to be overweight and wanted to weigh less (96%). Eighty percent said that it was very important to extremely important to become more physically active and lose weight.
Participants felt that they were most responsible for making changes to their diet and exercise. Many participants viewed their providers (94%), family (80%), and friends (64%) as valuable partners in helping them reach their goals for lifestyle modifications. The majority of participants saw their providers as somewhat to very effective in helping them change their diet (94%) and physical activity (96%), and nearly all (96%) viewed their providers as effective at helping them lower their chances of developing diabetes. Of note, participants tended to view their friends and family as less responsible than providers in helping them to make lifestyle changes to lower their risk of developing diabetes.
Behaviors
Participants were moderately active at baseline, with average daily steps of 7,074 (SD=2,716; range 2,437 – 16,406).35 Ninety percent of the group failed to meet recommendations of 10,000 steps per day (Figure 1).36
Figure 1. Steps-per-day at baseline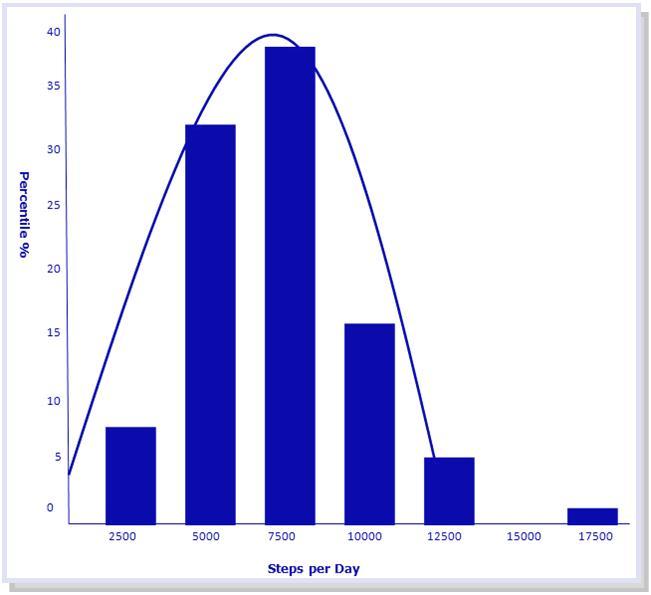
When asked about making lifestyle adjustments with regard to diet and exercise, participants asserted confidence that they could successfully make changes to their diet (mean=7.7 out of 10 point scale) and exercise (7.7 out of 10 point scale) to prevent diabetes. Nearly all respondents were in the preparation or action phases of the Stages of Change model for diet (75%) and exercise (94%). Seventy-six percent reported spending over 4 hours a day sitting down and using electronics. Although 96% of patients have tried to lose weight and become more physically active in the past 12 months, only 10% reported being successful at these attempts. Participants generally demonstrated poor eating habits and unhealthy diets as evidenced by their responses to food specific inquiries (Appendix A). Nearly 75% of patients ate less than 2 servings of fruits or vegetables a day and half of patients reported eating more than 4 meals per week from restaurants. Additionally, 34% reported skipping breakfast regularly. Still, nearly all participants (98%) answered that they were willing to make changes to their eating habits to be healthier.
Univariate Analysis
Participants who reported greater physical activity on the pre-enrollment survey recorded fewer daily steps on pedometer measurement; the negative correlation was moderate in strength (r = -0.35, p < 0.001). On the REAPS assessment, a tool used to assess diet related to U.S. dietary guidelines, participants reported moderately healthy overall intake (mean score 16.4 (SD 5.2) on a 39 point scale where higher scores are associated with poorer nutrition). Poorer scores on the REAPS measure of diet quality was associated with lower BMI; this negative correlation was also moderate in strength (r = -0.42, p = 0.0017). Number of daily steps and BMI were not correlated with other variables of interest, such as stages of change, diabetes knowledge, and diabetes risk perception.
Discussion
Our data suggest that contrary to common assumptions, patients enrolling in primary care-based prediabetes interventions are well-informed about their condition and exhibit high levels of risk perception, self-efficacy and motivation to change. Moreover, participants reported poor eating and physical activity habits despite their well-recognized risk for diabetes and positive attitudes towards diabetes prevention. These observations are particularly relevant considering the diversity of the sample and their high burden of diabetes risk factors including obesity, family history of diabetes, and cardiovascular comorbidities, however, they are not surprising. A 2009 study by Hivert et al. demonstrated that primary care patients with higher perceived risk scores on the RPS-DD questionnaire (“high risk” vs. “low risk”) were truly at increased risk of diabetes development, yet higher perceived risk did not result in adopting healthier behaviors.34 These findings suggests that the sample, recruited using practical trial methods, represents an ideal target for a prediabetes lifestyle intervention and would likely resemble the typical patient seen in urban primary care practices. The data were used to redirect the development of the ADAPT intervention away from enhancing patient knowledge, perceptions and attitudes and instead leverage the participants’ existing positive attitudes to replace less healthy behaviors with more healthy ones.
Barriers often cited for patients being unable to modify behaviors to prevent disease include the absence of health education, poor understanding of risk of disease and complications, and lack of motivation to change.37, 38, 39 Individual cultural beliefs, lack of community connection, and misperceptions about diabetes education programs also pose challenges to lifestyle change.40, 41, 42 However, this group of patients demonstrated adequate knowledge about their disease, appropriate risk perception for developing diabetes and its accompanying complications, and an overall high level of awareness of their unhealthy behaviors. Overall, patients had an accurate perception of the natural progression of prediabetes and diabetes. The fact that despite these factors they have been unsuccessful at making appropriate lifestyle changes emphasizes that cognitive awareness is not necessarily correlated with behavioral changes. ADAPT was therefore targeted to primary care patients presenting with adequate levels of knowledge and motivation, but who need a structured path to enact change.
Interestingly, participants who reported higher levels of physical activity were in fact walking less according to pedometer data. This discrepancy between impressions of versus actual physical activity level illustrates that patients often have inaccurate perceptions of their physical activity throughout the day.43 Additionally, participants who reported healthier eating habits (lower REAPS) had higher BMIs than those who reported poor eating habits. Again, this finding suggests that participants are either not good at judging their diet change efforts or are not accurately reporting their behaviors. These findings suggest a gap between patient intentions or self-perceptions about their behavior and their actual behaviors. The ADAPT tool may be valuable in bridging this gap between intentions to exercise and eat healthfully and taking action to adopt healthy behaviors.
Participants demonstrated high levels of self-efficacy and asserted their confidence in their ability to successfully change their eating habits and physical activity to prevent getting diabetes. Despite that, they have not been successful at making changes in the past. This disconnect between how confident people feel and how successful they have been highlights the need for an intervention such as ADAPT to support people in implementing change. Goal setting, action planning and other simple cognitive behavioral change methods are designed to help link intentions and actions.44 The SMART (specific, measurable, attainable, relevant, time-bound) goals based action planning used in ADAPT can help patients focus their intentions into concrete actions to achieve their goals.45, 46, 47
ADAPT incorporates the self-management support component of the Chronic Care Model, which includes goal setting, action planning, and problem solving,48, 49 and features a patient-centered approach to care that facilitates patient-selected short-term, specific goals coupled with provider feedback, which has been effective for patients at risk for or suffering from chronic diseases.44, 50, 51, 52 ADAPT is valuable to providers and patients because it provides the framework for shared goal setting and implementation during the clinical encounter. Barriers to patient adoption of lifestyle changes are also commonly attributed to the provider side of the patient-provider interaction. Effective counseling is challenging and providers often lack knowledge and successful strategies for helping their patients change behavior; there is much room for improvement of behavioral counseling rates.53, 54, 55, 56, 57 Data from the 2005-2006 National Health and Nutrition Examination Survey showed that only 34.6% of adults with prediabetes receiving health care reported that they had been told by their physician in the past year to control or lose weight; 36.8% reported being told to reduce calories in their diet and 39.4% reported being told to increase physical activity.58 Less than half of adult patients with diabetes are receiving provider advice on how to reduce risk. Clearly, providers could more actively counsel healthy lifestyle changes, especially in a group similar to this study population who are in the preparation/action stages of change. ADAPT presents providers with a workflow embedded simple shared goal setting platform and framework to guide patients who are ready for change through an iterative action planning process.
Study limitations include small sample size, single institution, and urban setting, thus generalizability is limited. Participants were recruited randomly from a clinical database and so there was a significant degree of selection bias; patients who answered their phones, responded to emails, had active insurance and ultimately enrolled in the study were likely more motivated at baseline to change their behaviors to prevent diabetes than the average person. However, this selection process was designed to identify the type of primary care patients who are sufficiently engaged with their healthcare team to benefit from a primary care based behavior change program.
ADAPT promotes action plan discussions between patients and providers for patient-selected behavior change goals during the outpatient visit. This study demonstrated that the recruited sample were already knowledgeable about their health and risk for developing diabetes, demonstrated high levels of self efficacy, placed value on being more active and losing weight, and strongly felt that they could successfully make lifestyle changes to prevent diabetes. This suggests that typical primary care patients are candidates for simple and efficient primary care based action planning interventions. The ADAPT tool was tailored to meet this population’s needs to structure/facilitate behavior change to reduce diabetes risk.
Funding:
This study was supported by a grant from the National Institute for Diabetes, Digestive and Kidney Diseases (5K23DK081665)
Abbreviations:
T2DM: Type II Diabetes Mellitus
ADAPT: Avoiding Diabetes Thru Action Plan Targeting
Appendix A. REAPS (Rapid Eating Assessment for Participants – Shortened) Questions| In an average week how often do you: | Usually | Often | Rarely/Never |
|---|---|---|---|
| Skip breakfast? | |||
| Eat 4 or more meals from sit-down or take out restaurants? | |||
| Eat less than 2 servings of whole grain products or high fiber starches a day? | |||
| Eat less than 2 servings of fruit a day? | |||
| Eat less than 2 servings of vegetables a day? | |||
| Eat or drink less than 2 servings of milk, yogurt, or cheese a day? | |||
| Eat more than 8 ounces of meat, chicken, turkey, or fish per day? | |||
| Use regular processed meats (like bologna, salami, corned beef, hotdogs, sausage or bacon) instead of low fat processed meats (like roast beef, turkey, lean ham, low fat cold/cuts, hotdogs? | |||
| Eat fried foods such as fried chicken, fried fish, French fries, fried plantains, tostones or fried yucca? | |||
| Eat regular potato chips, nacho chips, corn chips, crackers, regular popcorn, nuts instead of pretzels, low fat chips or low fat crackers, or air-popped popcorn? | |||
| Add butter, margarine, or oil to bread, potatoes, rice or vegetables at the table? | |||
| Eat sweets like cake, cookies, pastries, donuts, muffins, chocolate and candies more than 2 times a day? | |||
| Drink 16 ounces or more of non-diet soda, fruit drunk/punch or Kool-Aid a day? |