Abstract
Matrices or tissue scaffolds provide a collagen structure for tissue remodelling while the removal of viable cells aims to minimize or prevent inflammatory or immunogenic response.
Allograft collagen scaffold can support the patient’s own cellular ingrowth, ingeneered to minimize an immune response and to yeld a bio-compatible matrix and support incoming cellular growth. The decellyularized dermis retains its growth factors, native collagen scaffold, and elastin, thanks to a LifeNet Health proprietaryprocessin technology.
Author Contributions
Academic Editor: Mohamed Elfahar, Pan-Arab Federation of Societies for the Surgery of the Hand, Egypt.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Wu, Tsung-Hsuan, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Fingertip injuries are defined as those distal to the insertion of the flexor and extensor tendons Primary goal of treatment is a painless fingertip with durable and sensate skin. 1 Methods of treatment include healing by secondary intention, skin grafting, shortening of the bone and primary closure, and coverage with local or regional flaps.
Evaluation
History and mechanism of the injury
Patient factors age, gender, handedness, occupation, and history of previous hand injuries
Function of flexor and extensor tendons
Rx
Antibiotics and tetanus prophylaxis
Soft-tissue loss without exposed bone
Soft-tissue loss with exposed bone
Amputation
Nail bed injuries
Treatment
For the treatment of fingertip injuries, the decision making process should proceed from the simpler techniques to the more complicated. When no bone is exposed, the open method is ideal for small or moderate sized wounds, and skin grafting should be considered for larger wounds . Distal transverse and dorsal oblique amputations with bone exposure can be treated with local advancement flaps. 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14
Conclusion
Derma cell was able to provide protection for the wound while encouraging rapid healing without the disadvantages of donor site morbidity and increased patient pain from an autograft. The rapid wound closure was encouraging and supports further use of Derma Cell for treating soft tissue trauma wounds.
Case no. 1. 32 y/o, male. Crush injury with tip amputation of right middle finger. (Figure 1, Figure 2,Figure 3, Figure 4.)
Figure 1. Post-op
Figure 2. 4 days post-op
Figure 3. 2 wks postr-o
Figure 4. a-b: 4 wks post-op
Case no. 2. 48 y/o, female. Laceration wound of right index finger; dorsal oblique soft tissue defect; nail bed defect; over DIPJ with bone and joint exposure. (Figure 5, Figure 6, Figure 7, Figure 8.)
Figure 5. Post-op
Figure 6. 4 wks post-op
Figure 7. 8 wks post-op
Figure 8. 11 wks post-op
Case no 3. 42 y/o, male. Crush injury with soft tissue defect of volar side of the left thumb. (Figure 9, Figure 10, Figure 11, Figure 12, Figure 13.)
Figure 9. 4 days post-op
Figure 10. 15 days post-op
Figure 11. 2 months post-op
Figure 12. 3 months post-op
Figure 13. 4 months post-op
Case 4. 44 y/o female. Laceration wound of the left thumb; dorsal oblique soft defect; nail bed defect. Over D IPJ with bone and joint exposure. (Figure 14, Figure 15.).
Figure 14. 4 days post-op
Figure 15. 3 months post-op
Case 5. 24 y/o male. Contact full thickness burn wound of right thumb; soft tissue defect of dorsal side of the IPJ; tendon exposure. (Figure 16, Figure 17, Figure 18)
Figure 16. 2 weeks post-op
Figure 17. 6 weeks post-op
Figure 18. 10 weeks post-op
Case 6. 54 y/o male. Chemical burn, full thickness burn wound of right middle finger; tendon exposure. (Figure 19, Figure 20, Figure 21).
Figure 19. 8 days post-op
Figure 20. 2 months post-op
Figure 21. 4 months pos-op
Case 7. 40 y/o female. Crush injury of the right hand; amputation of right middle finger through DIPJ with volar oblique defect; amputation of right finger through middle phalanx with volar oblique defect; bone exposure. (Figure 22, Figure 23, Figure 24, Figure 25).
Figure 22. 8 days post-op
Figure 23. 2 weeks post-op
Figure 24. 2 months post-op
Figure 25. 3 months post-op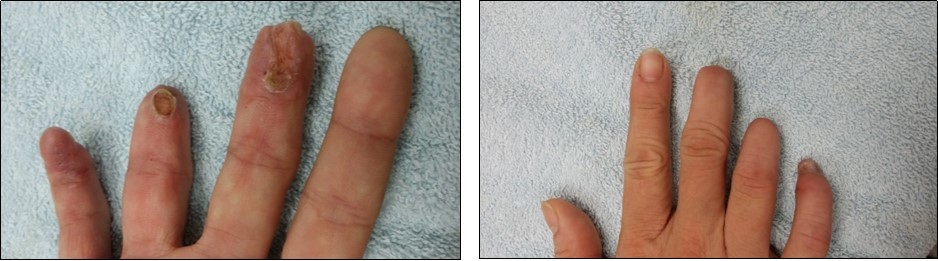
Result
The wounds progressed steadily, with full wound closure being achieved (average 1 to 4 months) after initial implantation. There were no signs of infection observed and the patient did not experience any reaction to the graft. Although the wound began healing slowly initially, the authors felt that was due to the complexity of the traumatic wound.
We T reat R outinely Finertip Injuries with ADM ( Derma cell ) .