Abstract
Background
Colon cancer is one of the leading causes of cancer death world-wide. There is a steady increase in incidence over the past four decades in developing countries. This has been partly attributed to increasingly low intake of vegetables among other causes.
Aims
Therefore this study aims to evaluate the protective effect of aqueous extract of Ocimumgratissimum (OG) leaves (a staple vegetable) on experimental model of colon carcinogenesis induced with 1, 2 Dimethylhydrazine (DMH). This is compared with celecoxib (a cyclooxygenase-2 inhibitor) which is used in the chemoprevention of colon cancer.
Methods
Sixty adult male Wistar rats were randomly divided into six groups: A to F, n=10. Group A was the normal control, Group B was given only DMH weekly for 16 weeks,Groups C, D and E were given graded doses of OG for two weeks prior to cancer induction by DMH. After which both OG and DMH were given for 16weeks. Group F received celecoxib daily for two weeks prior to cancer induction. Colonic wall was analysed grossly, histologically and biochemically. The induced lesions were staged investigated and staged using Duke’s Staging method.
Results
The result showed tumour incidence in groups B and C while no evidence of primary colonic tumour was observed in groups A, D, E and F. There was a dose dependent increase in the goblet cell count in the groups treated with OG with group E being statistically higher than group F. There was a significant reduction in collagen staining intensity (F = 129.74, p < 0.0001) for the colonic wall in group B when compared to other groups. There was a decreased nucleo-cytoplasmic ratio in groups C, D, E and F when compared to group B. There was a significant increase in the concentration of nitric oxide and prostaglandin E2in group B when compared to other groups D, E and F.
Conclusion
In conclusion, this research showed a protective effect of Ocimumgratissimum leaves on 1, 2-dimethylhydrazine-induced colon cancer which further corroborated its ethno-medicinal use.
Author Contributions
Academic Editor: Ahmed M S Hegazy, Associate Professor, Anatomy and Embryology, Faculty of Medicine, Benha University, Egypt. Anatomy Department, Faculty of Medicine, Northern Border University (NBU), Saudi Arabia
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Ugochukwu Umeaku, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cancer is still a significant cause of morbidity and mortality in the world1. This condition is worse in developing countries like Nigeria which still have a poor health care delivery system2. The incidence of colon cancer in Nigeria though much less when compared to the western world, has been increasing steadily over the past four decades. This has been partly attributed to westernization of the traditional Nigerian diet among other causes. It is the fourth commonest cancer in Nigerian men3. Its incidence in Nigeria has increased from 18.4 per annum between 1954-1969 to 86.8 per annum between 1991-20074. It is the second commonest cause of cancer death in the United States, only after cancer of the lungs5.
Both genetic and environmental (diet) factors play key roles in the aetiology of colon cancer6. Molecular mechanisms are diverse, and recent data suggest two main pathways: a mutational pathway, which involves inactivation of tumour suppressor genes such as adenoma polyposis coli (APC); and microsatellite instability which occurs in hereditary non-polyposis colon cancer (HNPCC) and a proportion of sporadic carcinomas.
The dietary factors most closely associated with increased colon cancer rates are low intake of un-absorbable vegetable fiber and high intake of red meat, processed meat and animal fat7, 8, 9. It is noted that reduced fiber content leads to decreased stool bulk and altered composition of the intestinal microbiota10. This change may increase synthesis of potentially toxic oxidative by-products of bacterial metabolism, which would be expected to remain in contact with the colonic mucosa for longer periods of time as a result of reduced stool bulk11. Also chronic inflammatory conditions such as Crohns disease and ulcerative colitis are strongly associated with the development of colon cancer12.
Deficiencies of vitamins A, C, and E, which act as free-radical scavengers, may compound damage caused by oxidants13. It has been observed that aspirin or other NSAIDs especially COX-2 inhibitors such as celecoxib have a protective effect14. This effect is mediated by inhibition of the enzyme cyclooxygenase-2 (COX-2), which is highly expressed in 90% of colorectal carcinomas15. COX-2 is necessary for production of prostaglandin E2, which promotes epithelial proliferation, particularly after injury. Also it has been observed that there is an up-regulation of nitric oxide synthase in humans who have colonic adenomas (pre-malignant lesion)16.
Ocimumgratissimum is a perennial plant that is woody at the base. It has an average height of 1-3m high tall17. Akinmoladun et al., 2007 observed that the phytochemical constituents of aqueous extract of Ocimumgratissimum leaves include saponins, tannins, phlobatannins, anthraquinones, steroids, terpenoids, flavonoids and cardiac glycosides. He also confirmed the anti-oxidative potential of Ocimum gratissimum18. It is well established that chemicals or agents with anti-oxidative properties are protective against colon cancer. Man et al., 2010 found out that saponins is an anti-cancer agent as well as have medical applications in that regard19.
This research work aimed to find out the effect of aqueous extract of Ocimumgratissimum leaves (a staple vegetable) on 1, 2 Dimethylhdrazine (DMH) induced colon cancer in adult male Wistar rats.
Materials and Methods
Aqueous extract of Ocimum Gratissimum Leaves
The leaves were procured from a local market at Ile-Ife, Osun State. It was identified by the taxonomist at the Department of Botany, Obafemi Awolowo University, Ile-Ife, Osun State and given a voucher number (IFE – 17485). The leaves were air dried, grounded and milled into a powder form. 50g portion of the milled leaves were weighed and soaked in 500ml of distilled water in a beaker. The mixture was then shaken and kept on the laboratory bench for 4hrs before filtering. The filtrate was evaporated to dryness in a rotary evaporator to obtain a paste which was further dried in a dessicator with constant changing of the self indicating silica gel. Appropriate mass of the residue (mass was prepared from the required doses) was prepared in distilled water (1 ml) and given to the rats. The dosages used were 80mg/kg, 40mg/kg and 20mg/kg.
Phytochemical Screening
The qualitative assessment of the phytochemical constituents of Ocimumgratissimum is as presented in Table 1.
Table 1. Phytochemical Constituents in the Aqueous Extract of Ocimum gratissimum leavesAnimals
Ethical Clearance was obtained from the Ethical Committee of the Institute of Public Health, Obafemi Awolowo University Ile-Ife, Nigeria. (HREC No: IPHOAU/12/586). The experiment was conducted on male Wistar rats, weighing between 150 - 180g. The rats were kept at room temperature, fed with standard pellet diet and allowed free access to clean water. They were housed in metallic cages and acclimatized for two weeks before commencement of the experiment.
Drug and Chemical
Celecoxib (200mg), manufactured by Pfizer Pharmaceuticals LLC, KM1.9 Road 689, Vega Baja, Puerto Rico was bought. 1, 2 – Dimethylhydrazine Dihydrochloride was bought from Santa Cruz Biotechnology Incorporated, Heidelberg, Germany.
Study Design
This research was carried out on 60 adult male Wistar rats which were divided into 6 groups, tagged group A, B, C, D, E and F. Ten rats were randomly selected into each group. Group A served as the normal control while Group B was given only DMH. Animals in groups C, D, E and F were given their respective chemo-protective agent of study two weeks before cancer induction by DMH. The cancer induction was at a dose of 25mg/kg/week imtramuscularly for 16weeks (Perše and Cerar, 2005)7. The DMH was then given as well as the agent of study (OG) concurrently to groups C, D and E for 16weeks. During this time OG at the doses of 20mg/kg/day, 40mg/kg/day and 80mg/kg/day orally was administered to rats in Groups C, D and E respectively. DMH and celecoxib (at 10mg/kg/day orally) were given concurrently to group F for 16weeks.
Sacrifice and Gross Examination of Tumour
The rats were sacrificed 24hrs after the last administration. The tumours seen in the colon were observed grossly and photographed. The rats in each group were divided into two equal halves. The colons of the first half were fixed in 10% formol saline. These tissues were stained with haematoxyline-eosin stain and Verhoff’s van Gisson according to standard protocol. The mucosae of the colon in the second half were scrapped and homogenized. The homogenate was de-proteinized. Nitric oxide and Prostaglandin E2 were assayed. The concentration of nitric oxide in the homogenate was done using the improved Griess method (Bryan and Grisham, 2007)20 while the prostaglandin E2 concentration was done using an ELISA kit bought from Wuhan Elabscience Biotechnology Company Limited, Building 4, Room 403, Guandong Science and Technology Industry Park, WuHan, China.
Duke’s Staging and Grading of Colon Cancer
Stage 0: no primary tumour seen
Stage A: tumours involve the wall of the bowel only (“Wall” is defined anatomically as including the mucosa, submucosa and circular and longitudinal fibers of the muscularis propria. Spread beyond the deep muscle layers in the absence of lymph node deposits, even if it comes into the serosa covering the colon comes into the Duke Stage B category).
Stage B: tumour extend through the wall without lymph node metastasis
Stage C: tumour have lymph node metastases.
Stage D: to indicate the presence of distant metastases.
Statistical Analysis
Data were analyzed using One-way ANOVA and expressed as Mean ± SEM. P < 0.05 was considered statistically significant except otherwise stated.
Results
Animal Weight
There was a significant net weight loss in the positive control group while there was a net weight gain in the groups administered with OG extracts. These weight increases were in a dose dependent manner as shown in Figure 1.
Figure 1. Bar chart is showing the change in rat weight between the start and end of the research work across the various groups. a, b, bc, c and d on top each bar signifies that mean with different letters differs significantly at p<0.05 while means with the same letters do not differ significantly at p<0.05 (using one way ANOVA with Duncan multiple range test).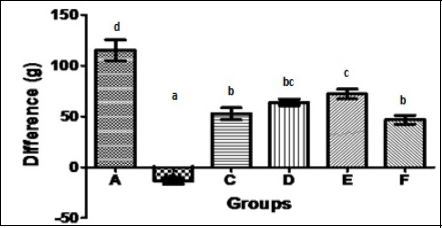
Gross Examination
There was tumour incidence of 90% in Group B while it was 40% in the group given the lowest dose of OG (Group C). There was no tumour seen in other groups as shown in Figure 2 and Table 2. A rat in Group B showed a tumour metastasis to the posterior abdominal wall (Figure 3).
Table 2. Total tumour incidence and number among the various groups| Groups | Tumour Incidence (%) | Total Tumour Number per group |
|---|---|---|
| A | 0.00 | 0.00 |
| B | 90.00 | 10.00 |
| C | 40.00 | 4.00 |
| D | 0.00 | 0.00 |
| E | 0.00 | 0.00 |
| F | 0.00 | 0.00 |
Figure 2. Gross pictures showing the distribution of colonic tumours (red arrows) across groups.
Figure 3. Metastasis to the posterior abdominal wall which measured 5cm x 5cm x 3cm in one of the rats in Group B.
Histopathological Examination/Duke Staging of Tumours
This was done according to the Duke Staging System. Staging of cancers mainly qualifies tumour progression. Photomicrographs show normal colonic mucosa in group Group A. This places the rats in Duke Stage 0. However, Group B and C (Figure 4) showed distortion of the normal mucosal arrangement of the colon due to proliferation of malignant glands (adenocarcinoma). At higher magnification (400x) irregularly shaped glands with high nucleo-cytoplasmic ratio were observed in Groups B and C. Loss of goblet cells was also observed. Groups D, E, and F have a seemingly normal histo-architecture when compared to the normal control. Similar staging as in group A (stage 0) applies to rats in groups D, E and F, since there was no primary colonic tumour seen in them. For the rats in Group B out of the five rats studied histologically, four had tumours that were only present on the colonic wall which puts them in Duke Stage A. The remaining rat had a tumour deposit in the posterior abdominal wall as shown in Figure 5 which puts it in Duke Stage D. For the rats in Group C out of the five rats studied histologically, two had primary colonic tumours that were limited to the colonic wall which puts them in Duke Stage A while the remaining three had no primary colonic tumour seen which puts them Duke Stage 0. All these information are presented in Table 3.
Table 3. Duke Staging of the tumours| Groups | Duke’s Stage | Total | ||||
|---|---|---|---|---|---|---|
| 0 | A | B | C | D | ||
| A | 5 | - | - | - | - | 5 |
| B | - | 4 | - | - | 1 | 5 |
| C | 3 | 2 | - | - | - | 5 |
| D | 5 | - | - | - | - | 5 |
| E | 5 | - | - | - | - | 5 |
| F | 5 | - | - | - | - | 5 |
Figure 4. Photomicrographs of the colon. Group A (Control), Group B (DMH Only), Group C (DMH + OG20), Group D (DMH + OG40), Group E (DMH + OG80), Group F (DMH + Celecoxib). (H & E 100x). M – Mucosa, SM – Submucosa, MP – Muscularis propria, MG – Malignant glands 
Figure 5. Bar chart showing the nucleo-cytoplasmic ratio of the cells lining the mucosa of the colon among the rats in the various groups.Each value represents Mean ± SEM, n=5. a and b within columns signifies that mean with different letters differs significantly at p<0.05 while means with the same letters do not differ significantly at p<0.05 (using one way ANOVA with Duncan multiple range test).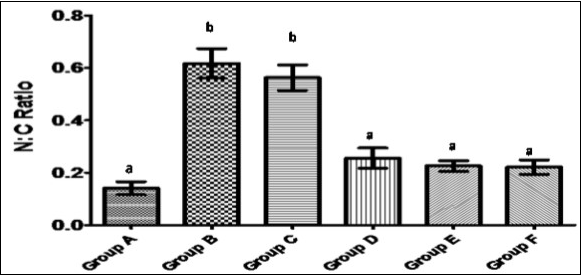
Stage 0 no evidence of primary tumor; Stage A tumors involve the wall of the bowel only; Stage B tumors extend through the wall without lymph node metastasis; Stage C tumors have lymph node metastases; Stage D category indicates the presence of distant metastases.
Nucleo-Cytoplasmic Ratio and Goblet Cell Density
There was a significant reduction of goblet cells in groups B and C when compared to other groups. The goblet cell count for groups D and E were not significantly different (Table 4).
Table 4. Showing Goblet Cell Count across the Various Groups| Groups | Goblet Cell Count (cells/µm 2 ) |
| A | 193.33 ± 4.06d |
| B | 76.33 ± 3.48a |
| C | 89.67 ± 3.18b |
| D | 185.00 ± 2.65cd |
| E | 187.33 ± 3.28cd |
| F | 182.67 ± 1.45c |
There was a significantly increased nucleo-cytoplasmic ratio (p<0.0001, F = 27.29) in groups B and C (0.61 ± 0.17 and 0.51 ± 0.09 respectively) which had malignant glands in them when compared to groups A, D, E and F (0.14 ± 0.08, 0.25 ± 0.12, 0.22 ± 0.06 and 0.20 ± 0.07 respectively).
Density of Collagen Fibers
They were loss of collagen fibers in the basement membrane and sub-mucosa in groups B and C which had malignant growth in them (Figure 6). The collagen staining intensity was done using Image – J software and the result which was plotted on a bar chart (Figure 7). There was a significant reduction in collagen staining intensity (p<0.0001, F=129.74) in group B (23.44 ± 2.87%) when compared to groups A, D, E and F (72.74 ± 2.81%, 63.98 ± 3.35%, 65.94 ± 3.37% and 67.95 ± 3.16% respectively). This staining intensity for collagen was increased in a dose dependent manner (p<0.05) in groups D and E when compared to group B.
Figure 6. Photomicrographs of the colon. Group A (Control), Group B (DMH Only), Group C (DMH + OG20), Group D (DMH + OG40), Group E (DMH + OG80), Group F (DMH + Celecoxib). (Verhoeff’s van Gisson Stain 100x). M – Mucosa, SM – Submucosa, MP – Muscularis propria, MG – Malignant glands. Red Staining – Collagen Fibres.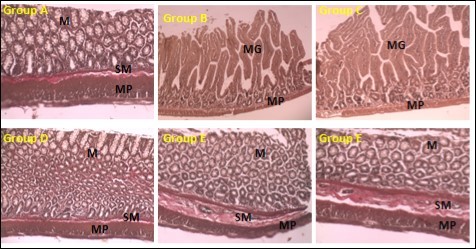
Figure 7. Bar chart shows collagen staining intensity (%) in the colon in the rats among the various groups. a, b, c, cd and d on top each bar signifies that mean with different letters differs significantly at p<0.0001 while means with the same letters do not differ significantly at p<0.0001 (using one way ANOVA with Duncan multiple range test). 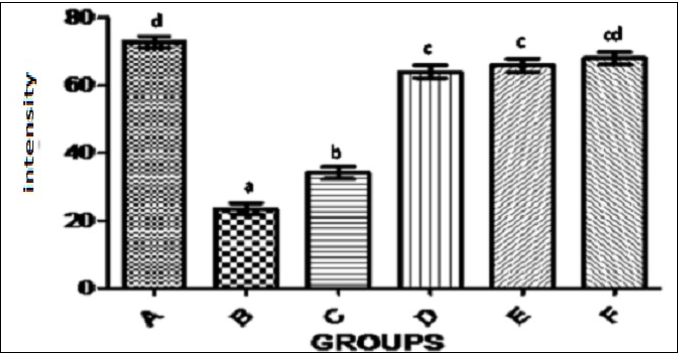
Prostaglandin E2 and Nitric oxide
Prostaglandin E2 concentration was significantly higher in groups B and C which had malignant glands present in them (p<0.0001, F=10.73) when compared to groups A, D, E and F (Table 4).
There was a significant increase in the concentration of nitric oxide (p<0.0001, F=15.75) in groups B when compared to that in groups A, D, E and F. The values of nitric oxide in groups D, E and F are not statistically significant while that of A, B and C differ significantly (p<0.0001) (Table 5).
Table 5. Table showing the concentration of Prostaglandin E2 and Nitric Oxide in the colonic mucosa of the rats across the various groups.| Groups | Prostaglandin E 2 ( pg /mg protein) | Nitric Oxide (µmol/mg protein) |
| A | 1.54 ± 0.07a | 5.32 ± 0.03a |
| B | 2.16 ± 0.05b | 6.20 ± 0.14d |
| C | 2.00 ± 0.02b | 5.92 ± 0.07c |
| D | 1.77 ± 0.08a | 5.60 ± 0.06b |
| E | 1.65 ± 0.02a | 5.57 ± 0.02b |
| F | 1.63 ± 0.06a | 5.56 ± 0.10b |
Discussion
In this study, we investigated the male rats to avoid the effect of hormonal changes of oestrus cycles of females21. Progressive loss of body fat and lean body mass accompanied by profound weakness, anorexia, and anemia accompanying cancer is referred to as cachexia. Unlike starvation, the weight loss seen in cachexia results equally from loss of fat and lean muscle22. There is some correlation between the tumour burden and the severity of the cachexia13. It is suspected that tumour necrosis factor (TNF) produced by macrophages in response to tumour cells or by the tumour cells themselves mediates cachexia23. TNF at high concentrations mobilizes fats from tissue stores and suppress appetite; both activities would contribute to cachexia (or weight loss). Other cytokines, such as IL-1, IL-6 and interferon-γ, synergizes with TNF to cause weight loss (or cachexia)23. Mice bearing ectopically-implanted C26 colon carcinoma are widely used as an experimental model of cancer cachexia24. The weight loss seen in the positive control group may be related to the presence of tumour growth within them. The weight gain observed in the groups given OG was directly proportional to the concentration of OG given. This is similar to a work by Costelli et al., 1993 that showed weight loss in tumour bearing rats25. They also showed that this is mediated by TNF. There was also a weight gain in the group treated with celecoxib. This is similar to the work by Lai et al., 2008 which showed that celecoxib ameliorates the effect of tumour cachexia (weight loss associated with cancer) in patients with cancer of the gastrointestinal tract26. The weight gain seen in the group treated with celecoxib is statistically similar to those given the lowest dose of OG even though the group was characterized by tumour growth suggesting that even though the lowest dose of OG given was not completely effective at preventing tumour growth, it showed similar ameliorating effect on tumour cachexia when compared to celecoxib treated group. Higher doses of OG have a better preventive effect against tumour cachexia than celecoxib as seen in this research work. Yanagihara et al., 2013 reported the protective role of flaviniods one of the compounds in OG on tumour cachexia27. The phytochemical screening in this study confirms the presence of flavonoids.
There was no observable tumour seen in the rats treated with celecoxib which is a selective COX-2 inhibitors as well as higher doses of OG. Non-steroidal anti-inflammatory drugs especially the COX-2 inhibitors have long been known to be protective against the development of colon cancers28. They do so by inhibiting the production of prostaglandin E2 which promotes the growth of clones of malignant cells. The absence of tumours in the groups given higher doses of OG may be due to the protective effect of the phytochemical constituents of OG on cancer. Alkaloids which are present in OG have been shown to be protective against colon cancer development in humans29. Cardiac glycosides which are also present in OG are known to be protective against cancer development30. George et al., 2017 also demonstrated a protective effect of flavonoids against DNA mutation which is an important step in carcinogenesis and as earlier mentioned are present in OG31. Steroids which are also anti-inflammatory will also reduce the concentration of prostaglandin E2 which is associated with colon cancer. Steriods are also present in OG as seen in the phytochemical screening. Tannins which are present in OG are also known to be chemopreventive against the development of colon cancer32. Terpenoids which are also present in OG have been observed to induce colon cancer cell death33. All these show that OG leaves have a preventive effect against colon cancer development and this effect is similar to that obtained with celecoxib. The colon cancer seen in the positive control group shows that the DMH is effective in inducing colon cancer.
Staging of cancer helps to give an idea about tumour progression. A rat in the positive control group had colon cancer at Duke stage D while those seen in group C are in Duke stage A. This showed that OG also has an ameliorating effect on tumour progression. The Duke stage of the rats given celecoxib and those given higher doses of OG was Stage 0. This means that higher doses of OG prevented the development of cancer just like celecoxib as earlier emphasized. The rat with stage D had tumour deposits in the posterior abdominal wall which is similar to the work by Ye et al., 2013 which also documented tumour spread to the posterior abdominal wall34. Apart from posterior abdominal wall, they can also metastasize to the liver and lungs13.
There was a reduction in goblet cells in the colon of the positive control group as well as the group given the lowest dose of OG. This reduction in goblet cells is an evidence of loss of differentiation within malignant colonic glands. Maliganant colonic glands were seen in the positive control group and the group given the lowest dose of OG. This finding is similar to the work carried out by Xu, (1990) where he sterelogically studied goblet cells in the colon. He found out that goblet cell count in the colon reduces as the differentiation of the colonic epithelium reduces35. He noticed that it can be reduced as much as 50% in settings of adenocarcinoma. This may be responsible for some of the symptoms like constipation, obstruction, perforation e.t.c. which patient with colon cancer experience. The groups given celecoxib and higher doses of OG have higher number of goblet cells.
There is reduced collagen staining in the basement membrane, lamina propria and submucosa in the positive control group and the group given the lowest dose of OG. While rats given higher doses of OG as well as celecoxib had higher amount of collagen in their basement membrane, lamina propria and sub-mucosa. Degradation of collagen within the basement membrane, lamina propria and sub-mucosa is an important step in tumour invasion and metastasis36. These are mediated by the proteolytic effect of tumour cells which secrete matrix metalloproteinases on the collagen within the basement membrane, lamina propria and sub-mucosa. These cancer cells generally need to degrade the collagen in basement membrane and lamina propria in other to progress to higher stages of the disease. OG has demonstrated a protective effect in this regard by limiting the degradation of collagen. This is similar to the work done by Bode et al., 2000 which showed that collagen fibers are reduced in the basement membrane in colon cancer37.
Increased nucleo-cytoplasmic ratio was seen in the cells of the malignant glands in positive control group and those given the lowest dose of OG. Those given the standard drug as well as higher dose of OG had a low and normal nucleo-cytoplasmic ratio. This still corresponds to the result on tumour incidence because malignant cells as a rule have increased nucleo-cytoplasmic ratio. It is also a reflection of the possible protective effect of OG on colon cancer development because before cells become malignant they are expected to accumulate ribonucleic acids and nucleotides in the nucleus before cell division can start. This leads to increase in nuclear diameter and subsequently increased nucleocytoplasmic ratio. So based on the above mentioned it can be said celecoxib and higher doses of OG have a preventive effect on colon carcinogenesis.
Nitric oxide (NO) is a ubiquitous, water soluble, free radical gas, which plays key role in various physiological as well as pathological processes. NO has emerged as a molecule of interest in carcinogenesis and tumour growth progression. However, there is considerable controversy and confusion in understanding its role in cancer biology. It is said to have both tumoricidal as well as tumour promoting effects which depend on its timing, location, and concentration38. NO has been suggested to modulate different cancer-related events including angiogenesis, apoptosis, cell cycle, invasion and metastasis38. Nitric oxide delivered by inflammatory cells, in particular, is important in causing changes in intestinal epithelial cells, setting the stage for colon cancer development39. There is up-regulation of nitric oxide synthase in rats who have colonic adenomas (pre-malignant lesion)17. The concentration of nitric oxide is higher in the positive control group and the group given lowest dose of OG. This is because nitric oxide is associated with inflammation and chronic inflammation is a known predisposing factor to development of colon cancer. The concentration of nitric oxide seen in the standard group as well as groups given higher doses of OG are similar which showed that higher doses of OG reduced the concentration of nitric oxide, a gas associated with inflammation in the same way as celecoxib does. By so doing, OG at higher doses reduces the concentration of NO in the colon just like celecoxib thereby preventing colon cancer development. Alkaloids, steroids, anthraquinones, flavonoids, saponins and tannins which are phytochemical constituents of OG are known to have anti-inflammatory properties39.
Cyclooxygenase-2 (COX-2) is highly expressed in 90% of colorectal carcinomas and 40% to 90% of adenomas (premalignant lesion). COX-2 is necessary for production of prostaglandin E2, which promotes epithelial proliferation including clones of malignant epithelial cells13. Prostaglandin E2 (PGE2) induces colon cancer stem cell like expansion in vivo and ex vivo40. Based on this, non-steroidal anti-inflammatory drugs (NSAIDS) especially COX-2 inhibitors are given to patients with colonic adenoma to prevent progression to carcinoma41. The concentration of prostaglangin E2 was higher in the positive control and the group given the lowest concentration of OG. The level of prostaglandin E2 in groups given celecoxib (standard group) as well as groups given higher doses of OG are low and are statistically similar. This shows that higher doses of OG reduce the concentration of PGE2 in the same way as will be expected for celecoxib. Prostaglandin E2 is also a cytokine and a derivative of arachidonic acid which is produced during inflammation. This result is in consonance with that obtained from nitric oxide which shows the anti-inflammatory properties of OG. Just as discussed in the preceeding paragraph, alkaloids, steroids, anthraquinones, flavonoids, saponins and tannins which are phytochemical constituents of OG are known to have anti-inflammatory properties.
In conclusion aqueous extract of OG leaves most likely protects against development of colon cancer and as such might be beneficial in the primary prevention of colon cancer.