Abstract
Purpose
To study outcome and spectral domain optical coherence tomography (SD-OCT) macular findings in patients who underwent surgery for spared macula giant retinal tear (GRT) retinal detachment.
Methods
a retrospective study of 12 patients with spared macula giant retinal tear (GRT) retinal detachment who underwent vitrectomy (N=7), vitrectomy with an encircling scleral buckle (n=4) and scleral buckle (n=1) with at least 3 months follow up after silicon oil removal (SOR) . Post-SOR macular SD-OCT scans were studied in all eyes.
Results
Final reattachment achieved in all eyes with single primary surgery. Post-SOR SD-OCT macular finding was photoreceptors layer disruption in 6 eyes, epiretinal membrane (ERM) in 4 eyes, Macular hole in 1 eye and choroidal neovascularisation in 1 eye. Significant correlation found between final Best-Corrected Visual Acuity (BCVA) and macular pathology on SD-OCT p value (0.048).
Conclusion
SD-OCT plays a high role in diagnosis of macular alterations that can be associated with poor functional outcome in anatomically successful GRT surgery with spared macula pre-operatively.
Author Contributions
Academic Editor: Paraskevi Riga, Aristotle University of Thessaloniki, Greece.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Eman Abo Taleb, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Giant retinal tears (GRT) are retinal breaks with circumference that extend over 3 clock hours or more. Treatment of choice is a pars plana vitrectomy (PPV) with reposition of the inverted central retinal flap using perfluorocarbon liquids, endolaser, or cryocoagulation and tamponade of the retina using silicone oil. In addition, some surgeons prefer to use an encircling scleral buckle or a scleral buckle for a portion of the circumference.1
During the last 30 years advances in vitreoretinal surgical techniques resulted in high percentages of anatomical success in giant retinal tear (GRT) detachment repair surgery. Despite the high percentages of satisfactory anatomic results, very often the functional results still remain puzzling.2
Visual disturbances are mainly related to macular abnormalities which may be easily overlooked during standard clinical examination using slit-lamp biomicroscopy.3Spectral-Domain Optical Coherence Tomography (SD-OCT) provided an additional tool for clinicians for in vivo studies of the individual layers of the macula with high resolution and thus provided further information for structural postoperative macular changes. Most of the studies utilizing the SD-OCT emphasize the value of the integrity of the photoreceptors layers as an index for visual rehabilitation after anatomically successful retinal detachment surgery. However, discrepancies between the results of the different studies still exist.2
The purpose of this study is to study the correlation between poor BCVA and SD-OCT macular findings post-silicon oil removal (SOR) in giant retinal tear retinal detachment without macular involvement preoperatively.
Methods
This retrospective study of 12 patients (12 eyes) who underwent retinal detachment surgery for macula on GRT over a 10-year period from May 2004 to November 2013 at Retina Foundation and Asopalav Eye hospital Ahmedabad , India. Informed written consent was obtained from each patient before surgery. Medical records of these patients have been reviewed and subjects with macula on giant retinal tears have been identified. Data sheets have been designed and patient information including age, sex, lens status (phakic, pseudophakic, or aphakic), laterality (right or left eye), duration of retinal detachment, extent of GRT and preoperative grade of PVR have been noted.
All patients underwent complete preoperative ophthalmic examinations including best-corrected visual acuity (BCVA) using the Snellen chart, slit-lamp biomicroscopy, intraocular pressure (IOP) measurement using non-contact tonometer, fundus examination by indirect ophthalmoscopy, and B-scan ultrasonography if required.
All eyes have been operated under general or local anaesthesia. At the beginning of surgery, 360° peritomy has been done followed by slinging of the four recti muscle and placement of an encircling equatorial band No. 240 (2.5 mm), but not tied till the retina was flattened. Conventional 3-port pars plana vitrectomy (PPV) procedure using 23-gauge or 25-gauge vitrectomy system coupled with contact wide field viewing system have been used. Vitrectomy has been performed and then perfluorocarbon]liquid (PFCL) has been injected into the vitreous cavity to unroll the retina and displace the subretinal fluid. This has been followed by diathermy of the edges of the tear, excision of the anterior flap, and smoothening of the edges of the posterior flap. Meticulous removal of the peripheral vitreous base under wide field viewing with indentation with all efforts made to remove as much vitreous as possible. Under PFCL tamponade, 360° laser (several rows extended up to the retinal periphery) has been applied to seal the retina. Finally, PFCL air exchange followed by silicon oil air exchange has been done. The height of the buckle aimed to be relatively low and broad to minimize radial folds formation. All patients have been instructed for postoperative face down for 10 hours daily for at least seven days. All surgeries have been done by one surgeon. In phakic eyes, the lens was spared in all cases. Follow-up examinations have been done at postoperative Day 1, Months 1, 3, and 6. Silicon oil removal, with or without cataract surgery, has been planned following signs of oil emulsification. All patients have been followed up regularly for at least three months after silicone oil removal with complete ophthalmological examination each visit with special attention to best-corrected visual acuity (BCVA), lens status, IOP and peripheral retinal status. Images have been acquired with Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Germany), which combines a confocal scanning laser ophthalmoscope with spectral-domain OCT of the macula after SOR. The OCT recording protocol consisted of a sequence of 97 horizontal sections recorded in the high resolution mode (1024 A-scans/30°), covering an area of 20° (horizontal) × 20° (vertical) with a distance of approximately 60mm between individual sections. In selected cases, vertical or oblique scans have been obtained to better study the observed abnormalities.
For statistical analysis, Snellen visual acuity has been converted to the logarithm of the minimum angle of resolution (logMAR). Mean has been used for description of quantitative data, and percentages have been used for qualitative data. Univariate analyses, such as the chi-square test and Fisher exact test, have been used to compare qualitative data, whereas the two-sample t-test has been used to compare quantitative. Statistical analyses have been done using SPSS statistical software (version 19.0; SPSS, Inc., Chicago, IL). For all statistical tests, P ≤ 0.05 has been considered significant.
Results
Twelve eyes (12 patients) with macula on GRT have been included in the current study. The mean age was 46.5± 2.51 years (range: 27 years-58 years). Male gander was more prevalent 9 patients (75%) than female gander 3 patients (25%). GRTs were idiopathic in 7 eyes (58.3%), myopia in 3 eyes (33.3%) and trauma in 1 eye (8.3%) previous cataract surgery in 7 eyes (72.7%). Table 1.
Table 1. Baseline Characteristics| Mean age | 46.5±2.51 (27-58) |
| Age Group | |
| ≤30 | 1 (8.3%) |
| >30 | 11 (91.7%) |
| Gender | |
| Male | 9(75%) |
| Female | 3 (25%) |
| Eye | |
| Right | 7 (58.3%) |
| Left | 5 (41.7%) |
| Risk factor | |
| Idiopathic | 7 (58.3%) |
| Myopia | 3 (33.3%) |
| Trauma | 1 (8.3 %) |
| Mean duration of symptoms | 18.25±6.7 (4-90) |
The mean presenting visual acuity (VA) was logMAR 0.785±0.562. A significant proportion of eyes presented with VA between 20/200 and 20/40 (6 eyes 50%) and 2 eyes (16.7%) with presenting VA better than 20/40 and 4 eyes (33.3%) with presenting VA less than 20/400 . PVR found in 11 eyes (91.3%) with two eyes (16.7) with PVR grade C or greater.
The circumference of the GRT was between 90˚-180˚ in 11 eyes (91.7%), between 180˚-270˚ in only one eye (8.3%). Pars plana vitrectomy was done on 7 eyes (58.4%), 4 eyes (33.3%) were treated by combined scleral buckling and PPV and one eye (8.3%) GRT macula on was treated with cryotherapy and scleral buckle surgery.
Final reattachment was achieved in all eyes with single primary surgery with final visual acuity more than 20/40 in 0 eyes (0.0%).High IOP was the most common Post-operative silicon oil complications 6 eyes (50%) and 2 eyes (16.7%) cataract with no significant correlation with final post-SOR BCVA p value 0.38 . The mean time for SOR was 12.08±9.91 months range between (6 months-36 months). No significant difference between preoperative BCVA (log MAR=0.785) and post-SOR BCVA (log MAR=0.908). Table 2.
Table 2. Outcome| Post-SOR BCVA in comparison with pre-operative BCVA | |
| Improve | 3 (25%) |
| Decrease | 9 (75%) |
| Unchanged | 0 (0.0%) |
| Final anatomy | |
| attached | 12 (100%) |
| Not attached | 0 (0.0%) |
Post-SOR SD-OCT macular findings were Photorecepter layer disruption 6 (50%), Epiretinal membrane 4 eyes (33.3%) Figure 1, macular hole 1 eye (8.1) and choroidal neovasculrization on 1 eye (8.3%) Figure 2 with significant correlation with final post-SOR BCVA p value 0.048 Table 3.
Figure 1. 4 years Post-SOR SD-OCT image of a 42-year-old patient with BCVA 6/12 after anatomical repair of a macula-on GRT with PPV + SOI with preoperative BCVA 6/18. We can, notice the presence ERM and CME.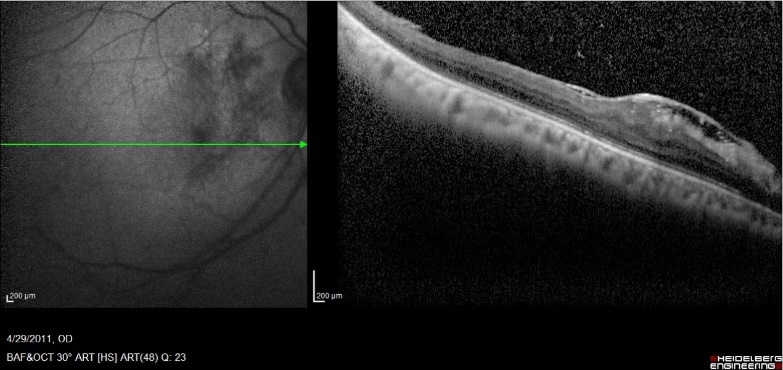
Figure 2. 3 years Post-SOR SD-OCT image of a 44-year-old patient with BCVA 6/36 after anatomical repair of a macula-on GRT with encilrclage PPV + SOI with preoperative BCVA 6/6. We can notice the presence of SRNVM, IS/OS (ellipsoid zone) disruption, and RPE changes.
| Photorecepter layer disruption | 6 (50%) |
| Epiretinal membrane | 4 (33.3%) |
| Macular hole | 1 (8.3%) |
| Choroidal neovascularization | 1 (8.3%) |
| significant correlation between final BCVA and macular finding on OCT p 0.048 |
Discussion
Poor functional outcome can occur after anatomically successful macula on GRT surgery. Our study using SD-OCT reveals that the anatomical changes at the level of the macula are the reason of poor visual recovery after a successful retinal reattachment surgery in macula on GRT retinal detachment. Although the evaluation of microanatomy of the macula (photoreceptors layer) may be helpful for further understanding the pathophysiology of poor vision. In our patients incomplete visual recovery in the absence of anterior segment pathology was always associated with macroanatomical features (epiretinal membrane, thickening, or choroidal neovascularization) that seen in SD-OCT. We found that BCVA may worsen on long-term after GRT macula on repair, the disruption of photoreceptor IS/OS is found to be the most important correlate of visual acuity and function in the long-term follow-up. Saadia Rashid and et al in their study of five-year follow-up of macular morphologic changes in FD-OCT after RRD repair, they found that persistent inner segment–outer segment disruption correlates with worsening or persistently poor visual outcome.4
Panagiotis and et al on their study about SD-OCT findings in macula after treatment of RRD with spared macula preoperatively, they found that Subretinal fluid can be found early and it was responsible for diminution of early BCVA after successful treatment of rhegmatogenous retinal detachment and OCT identifies the presence of fluid and contributes to the study of the fluid’s evolution.5
Cystoid macular edema appears to be the most frequent early postoperative macular complication associated with poor visual outcome. However, CME tends to decrease with time and sometimes disappear spontaneously.2 In our study CME and subretinal fluid which they are responsible for early postoperative poor BCVAwere not seen in our patients as their OCT was done years after surgery.
Epiretinal membrane formation resulting in contraction and distortion of the retina is another complication that can be associated with decreased visual acuity and metamorphopsia after anatomically successful retinal detachment surgery.6,7 In the present study,we evaluated the presence of ERM with SD-OCT imaging and the macula distortion. The presence of ERM was quite frequent with four patients (33.3%).
Another less frequent pathology related to poor visual outcome is the macular atrophic changes with subretinal neovascular membrane (SRNVM) one patient (8.3%) and the development of a macular hole one patient (8.3) during or immediately after GRT macula on surgery. Our results was quite similar to Miltiadis and et al study where they have studied SD-OCT findings in patients with incomplete visual recovery after anatomical successful retinal detachement.2,8