Abstract
Purpose
The goal of this study is to determine the association of L162V polymorphism of PPAR-alpha gene, A603G polymorphism of tissue factor gene and the risk of coronary heart disease development in Russian population.
Materials and Methods
A clinical and genetic study of 414 patients with CHD and 220 people of comparable age without CHD which amounted to a control group was performed. L162L and L162V genotypes of L162V polymorphism of PPAR-α gene, A603A, A603G and G603G genotypes of A603G polymorphism of tissue factor gene were determined by polymerase chain reaction followed by restriction analysis.
Results
A carriage of L162V genotype and V allele of PPAR-α gene was associated with an increase risk of CHD in 2,13 times (L162V genotype) and in 2,21 times (V allele), with an increase in risk of CHD before the age of 45 years in 4,68 times (L162V genotype) and in 3,88 times (V allele). Significantly higher in patients with CHD compared with the general population and in patients with a carriage of G603G genotype and G allele of tissue factor gene was associated with the increase of CHD risk in 2,68 times (G603G genotype) and in 4,37 times (G allele), occurred more frequently in patients with debut of disease at age of 45 years and younger. The level of tissue factor was significantly higher in patients with CHD – carriers G603G genotype compared with carriers A603A genotype (217,9±15,2 pg/ml and 152,6±30,4 pg/ml, respectively, p=0,04). A carriage of the combination of L162V and G603G genotypes was associated with an increased risk of CHD in 3,04 times.
Conclusion
A carriage of V allele of L162V polymorphism of PPAR-α gene and G allele of A603G polymorphism of tissue factor gene, as well as their pair combination are associated with an increased CHD risk, especially at age 45 years or less.
Author Contributions
Academic Editor: Akshay Kakumanu, Fulcrum Therapeutics, United States.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 E.G. Sergeeva, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The risk of coronary heart disease (CHD) varies considerably in different ethnic groups, which may be due to genetic factors 1. Thus, one of the most important are the new genetic risk factors of CHD, associated with immune inflammation and intravascular thrombosis 2.
Especially important to study gene-to-gene interactions that increase the risk of early debut of CHD and myocardial infarction 3. The integration of immune response, haemorheology disorders and endothelial dysfunction occur through pleiotropy effects of peroxisome proliferator-activated receptor-α (PPAR- α) 4.
Activation of PPAR-α contributes to the suppression of various mechanisms of immune inflammation through a system of nuclear factor κ-β: production of proinflammatory cytokines (interleukin 6, 8, 1-β, interferon - γ, tumor necrosis factor-α, VCAM-1), the adhesion and the migration of mononuclear cells into the subendothelium, suppression of pro-inflammatory activity of the endothelium and the production of acute phase proteins 5. PPAR-α have a layered effect on lipid metabolism: increase the synthesis of high-density lipoprotein cholesterol, stimulate reverse cholesterol transport, lower triglyceride levels 6.
PPAR-α gene localized in the long arm of 22nd chromosome. L162V polymorphism PPAR-α gene is characterized by replacement of leucine to valine at 162 position and is due for replacement of G to C 484 5-position of gene's exon. L162V genotype PPAR-α gene was associated with components of the metabolic syndrome 7, with the early development of CHD (Northwick Park Heart Survey), occurs four times more frequently in patients with angiographically verified coronary atherosclerosis than in the control group 8. This genotype was associated with the early development of diabetes 9. Carriers of L162V genotypes with diabetes melitus type 2 had higher levels of total cholesterol and apolipoprotein AI 9.
One of the important pathophysiological mechanisms of activation of PPAR-α receptor is suppressing of tissue factor expression. Tissue factor is a primary element of coagulation cascade and is directly relevant to thrombogenesis. In case of cell's damage part of tissue factor molecules are tightly associated with the coagulation factor VIIa, supporting its function in an external way the accelerator of blood coagulation. A603G polymorphism tissue factor gene has prognostic value in acute coronary syndrome 10, therefore, its study with a clinical position is extremely important.
Tissue factor serum levels depend on external factors as well as genetic factors. T. Ott et al have found that carriage of G allele gene polymorphism A603G tissue factor is associated with higher concentrations of tissue factor in the blood plasma and increased risk of myocardial infarction 11.
A603G gene polymorphism of tissue factor was associated with death and reinfarction in patients with myocardial infarction 12. In addition, this polymorphism is associated with an increased risk of venous thrombosis and CHD 13.
It is found that PPAR-α decrease tissue factor expression and activity in human mononuclear cells 14. Therefore, the study of gene-gene interactions of PPAR-α and tissue factor genes is extremely important.
The goal of this study is to determine the association of L162V polymorphism of PPAR-alpha gene, A603G polymorphism of tissue factor gene and the risk of coronary heart disease development in Russian population.
Materials and Methods
The current study included 414 patients with CHD (men and women) aged 33 to 80 years (mean age – 61,6 ± 0,48 years). The control group consisted of 220 people without CHD of comparable age (mean age – 60,09 ± 0,72 years, p = 0.081).
The majority of the surveyed patients had a history of myocardial infarction – in 295 (71,3%) of all patients with CHD
Traditional CHD risk factors in different age groups of CHD onset are shown in Table 1. Such traditional CHD risk factors as hypertension, smoking, obesity or overweight, dyslipidemia, were detected more frequently than in half of observed cases.
Table 1. The traditional CHD risk factors in patients with onset of the disease at different ages| No | Traditional CHD risk factors | Age of CHD debut | Р | ||
| 45 years and younger (N=58) (1) | 46 – 59 years (N=203) (2) | 60 years and older (N=153) (3) | |||
| 1 | Arterial hypertension | 51 (87,9%) | 191 (94%) | 146 (95,4%) | Р1,2=0,096Р1,3=0,055Р2,3=0,388 |
| 2 | Smoking | 39 (67,2%) | 140 (68,9%) | 85 (57,4%) | Р1,2=0,471Р1,3=0,083Р2,3=0,007 |
| 3 | Family history of CHD | 28 (49%) | 82 (40,4%) | 61 (42,4%) | Р1,2=0,155Р1,3=0,172Р2,3=0,534 |
| 4 | Diabetes mellitus type 2 | 13 (22,4%) | 40 (19,7%) | 25 (16,3%) | Р1,2=0,375Р1,3=0,005Р2,3=0,0001 |
| 5. | Obesity / overweight | 44 (78,6%) | 142 (69,9%) | 89 (59,7%) | Р1,2=0,231Р1,3=0,012Р2,3=0,016 |
| 6. | Dyslipidemia(atherogenic index > 3) | 25 (71,4%) | 137 (67,5%) | 50 (61,7%) | Р1,2=0,316Р1,3=0,106Р2,3=0,151 |
There were no significant differences in the frequency of occurrence of such traditional factors of CHD as hypertension, family history, fasting hyperglycemia and dyslipidemia in patients with the debut of the disease in different age (p>0,05, Table 1). However, a history of smoking were detected significantly more often in the group of studied patients with CHD debut at the age of 46 – 59 years compared with the group of patients with debut of the disease at the age of 60 years and older (p = 0,0071, Table 1). In addition, diabetes mellitus type 2, obesity or overweight were more common in patients with CHD debut at the age of 59 years and less compared with the group with debut of disease at the age of 60 years and older (p<0,017, Table 1).
Molecular-genetic examination of patients with CHD and a control group of comparable age without CHD was performed. Deoxyribonucleic acid (DNA) extraction from venous blood leukocytes was carried out on the column "K-SORB-100" ("Syntol", Russian Federation).
To determine the polymorphic variants of L162V PPAR-α gene polymorphism PCR was performed on an automated thermocycler Tertsik on a thermal cycler (DNA Technology, Moscow).
Amplification of the fragment was produced using the following sequence of synthetic oligonucleotides (Beagle, Russian Federation):
• forward primer: 5'GACTCAAGCTGGTGTATGACAAGT-3;
• reverse primer: 5'CGTTGTGTGACATCCCGACAGAAT-3.
The reaction mix for restriction analysis included 18 mkl of the PCR product, 1mkl of restriction enzyme Hinf I (SibEnzyme, US LLC), buffer O. Incubation of mix produces at 37 °C for 12 hours.
Restriction analysis was performed using a vertical electrophoresis in 8% polyacrylamide gel followed by staining with ethidium bromide and visualization in the ultraviolet.
Polymorphic variants of A603G polymorphism of tissue factor is determined by PCR. Amplification of the studied fragment of tissue factor gene was carried out using synthetic oligonucleotides shown below (Beagle, Russian Federation):
• forward primer: 5'AGTCACTATCTCTGGTCGTA-3;
• reverse primer: 5'CTTCCCTTCCATTTGGTGAT-3.
Restriction analysis was performed with the use for the preparation of the reaction mix 1 mkl restriction enzyme Bst2UI (SibEnzyme, US LLC), 2 mkl tenfold buffer G, 0,2 mkl of the BSA. Incubating the mix was performed at 60оC for five hours, followed by visualizing a 2% agarose gel stained with ethidium bromide, using UV light.
Statistical analysis was performed using the statistical software package Statistica 10 (Stat Soft Inc., version 10.0.228.8, Oklahoma, USA). Analysis of qualitative binary signs held by means of Fisher's exact test.
Results
A comparative analysis of the distribution of L162L, L162V genotypes and frequency of alleles L and V of L162V polymorphism of PPAR-α gene in patients with CHD and in the control group of comparable age without clinical and angiographic evidence of CHD. Analytical data presented in Table 2.
Table 2. Distribution of L162L and L162V genotypes and frequency of alleles L and V of L162V polymorphism of PPAR-α gene in CHD patients and in the control group without CHD| Observed groups | PPAR-α gene genotype | Allele frequency | ||
| L162L | L162V | L | V | |
| CHD patients (n=414) | 358(86%) | 56(14%) | 7720,932 | 560,068 |
| Control group without CHD (n=220) | 206(93,6%) | 14(6,4%) | 4260,963 | 140,037 |
| p | 0,004 | <0,005 | ||
| OR | OR=2,13; CI:1,16÷3,9 | OR=2,21; CI:1,21÷4,01 | ||
Analysis of the distribution L162L, L162V L162V polymorphism genotypes PPAR-α gene in patients with coronary heart disease and in the control group without CHD revealed the following statistically significant differences. Distribution in CHD patients was as follows: L162L genotype – 358 of 414 (86%), L162V genotype – 56 of 414 (14%). In the control group without CHD distribution was as follows: L162L genotype – 206 of 220 (93,6%), L162V genotype – 14 of 220 (6,4%) (p=0,004, Table 2). Thus, L162V genotype of PPAR-α gene was significantly more common in patients with CHD than in the control group without CHD. Thus, the carrier L162V genotype was associated with an increased risk of CHD in 2,13 times in comparison with the control group without CHD (OR=2,13; CI:1,16÷3,9; p=0,008, Table 2). The incidence V allele was higher in CHD patients than in the control group and the carriage V allele associated with an increased CHD risk by 2,21 times compared with the control group without CHD (OR = 2,21; CI : 1,21 ÷ 4,01, Table 2).
(Table 2) – Distribution of L162L and L162V genotypes and frequency of alleles L and V of L162V polymorphism of PPAR-α gene in CHD patients and in the control group without CHD
The patients were divided into three groups: those with coronary heart disease debut at the age of 45 years or less, aged 46 – 59 years, 60 years of age and older. Results of the analysis of genotypes and alleles distribution of L162V polymorphism (PPAR-α gene) in patients with CHD with the debut of the disease at different ages are presented in Table 3.
Table 3. Distribution of L162L and L162V genotypes and frequency of L and V allele of L162V polymorphism of PPAR-α gene in CHD patients with the debut of the disease at different ages| Observed groups | Genotypes of PPAR-α gene | Allele frequency | ||
| L162L | L162V | L | V | |
| 1. Patients with CHD debut at age 45 years and younger (n=58) | 38(65,5%) | 20(34,4%) | 960,86 | 200,14 |
| 2. Patients with CHD debut at age 46 – 59 years (n=203) | 181(89,2%) | 22(10,8%) | 3840,95 | 220,05 |
| 3. Patients with CHD debut at age 60 years and older (n=153) | 139(90,8%) | 14(9,2%) | 2920,95 | 140,05 |
| p(1,2)р(2,3) | 0,000020,133 | 0,000050,13 | ||
| OR(1,2) | 4,68; CI:2,3÷9,52,P < 0,0001 | 3,88; CI:2,02÷7,46,P < 0,0001 | ||
L162V heterozygous genotype carried 20 of 58 (34,4%) patients with CHD with the debut of the disease at the age of not more than 45 years, 22 of 203 (10,8%) – at the age of 46 – 59 years. Thus, L162V genotype PPAR-α gene was detected significantly more often in patients with coronary heart disease debut at age of 45 or younger (p = 0,00002) and was associated with an increased risk of CHD at the age of 45 years or less in 4,68 times (OR = 4,68; CI: 2,3 ÷ 9,52, Table 3). V allele was detected significantly more often in patients with CHD incidence aged 45 years or less (p = 0,00005, OR = 3,88; CI: 2,02 ÷ 7,46).
An assessment tissue factor level in the serum of 110 patients with CHD and 60 people in the control group without clinical and angiographic evidence of CHD.
In the group of CHD patients tissue factor level was 197,3 ± 9,2 pg/ml, while in the group without CHD – 132,4 ± 7,6 pg/ml. Thus, the level of tissue factor was significantly higher in CHD patients than in the control group (p = 0,000004, Figure 1).
Figure 1. Content of tissue factor serum in CHD patients and controls without CHD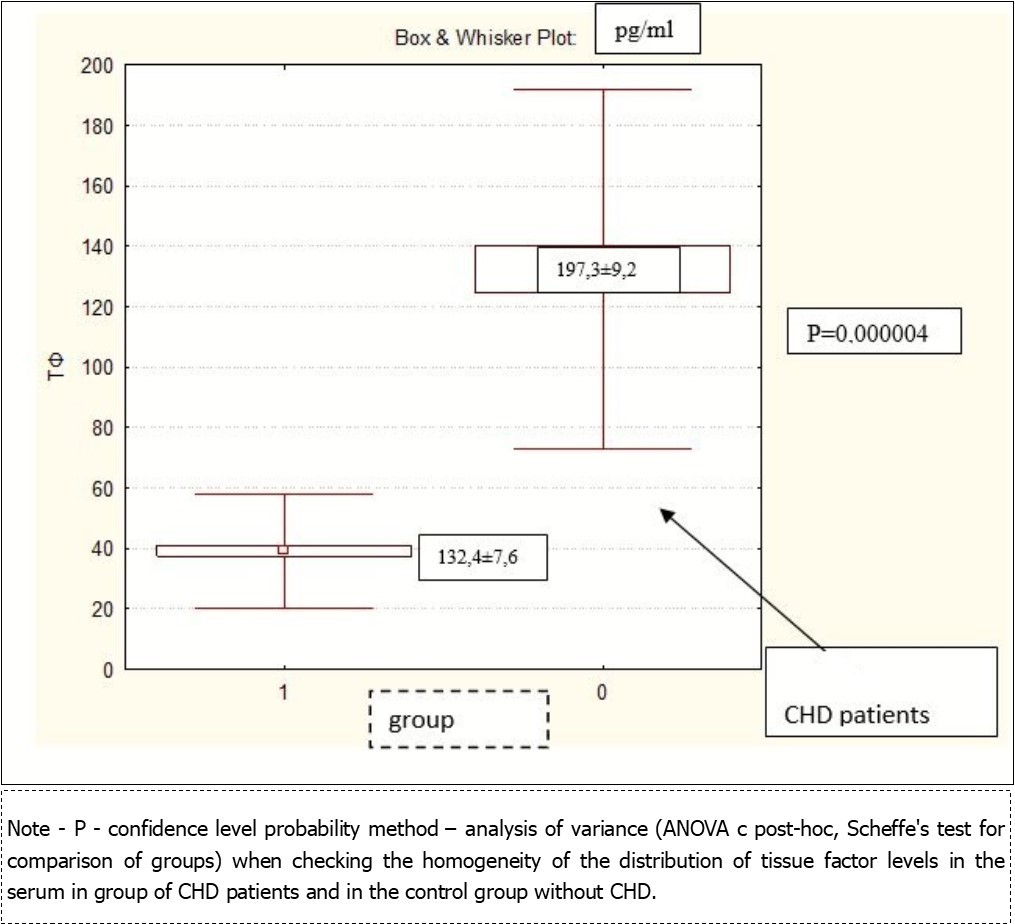
The distribution A603A, A603G and G603G genotypes of tissue factor gene in CHD patients differed from distribution of above mentioned genotypes of control group without clinical and angiographic evidence of CHD. Thus, G603G genotype was detected significantly more often in CHD patients than in the control group without CHD, and his carriage increased the risk of CHD (OR = 2,68, CI: 1,78 ÷ 4,01, p<0,0001, Table 4). G allele was significantly more often detected in CHD patients compared with the control group and was associated with an increased risk of CHD in 4 times.
Table 4. Distribution A603A, A603G, G603G genotypes and frequency of G and A alleles A603G polymorphism tissue factor gene in CHD patients and in the control group without CHD| Observed groups | Genotype of tissue factor gene | Allele frequency | |||
| A603A | A603G | G603G | A | G | |
| CHD patients (n=314) | 51(16,2%) | 144(45,8%) | 119(38,0%) | 2460,39 | 3820,61 |
| Control group (n=220) | 72(33%) | 107(49%) | 41(18%) | 2510,57 | 890,43 |
| p | <0,00001 | <0,0001 | |||
| OR | 2,68, CI:1,78÷4,01, р<0,0001 | 4,37, CI:3,28÷5,83,р<0,0001 | |||
An assessment of tissue factor level and distribution A603A, A603G, G603G genotypes of A603G polymorphism of tissue factor in patients with CHD and in the control group without CHD. The results are shown in Table 5.
Table 5. The tissue factor level in CHD patients - carriers of A603A, A603G, G603G genotypes of tissue factor| Observed groups | Genotypes of tissue factor gene | Р | ||||
| A603A | A603G | G603G | AA vs AG | AG vs GG | AA vs GG | |
| CHD patients (n=110) | 152,6±30,4 pg/ml | 195,9±12,4 pg/ml | 217,9±15,2 pg/ml | 0,15 | 0,26 | 0,04 |
| Control group (n=60) | 118±14 pg/ml | 132,9±8,1pg/ml | 150,6±18,5pg/ml | 0,35 | 0,32 | 0,16 |
The level of tissue factor was significantly higher in patients with CHD – carriers G603G genotype compared with carriers A603A genotype (217,9±15,2 pg/ml and 152,6±30,4 pg/ml, respectively, p=0,04), but not significantly different when comparing the groups of patients with CHD – carriers A603G A603A and genotypes as well as genotypes of A603G and G603G A603G gene polymorphism tissue factor (p> 0,05). In the control group the levels of tissue factor were not significantly different between carriers of different genotypes under study tissue factor gene polymorphism (p> 0,05, Table 4, Table 2).
Evaluation of distribution of A603A, A603G and G603G genotypes of tissue factor gene was performed between patients with CHD debut at the age of 45 years and younger and at the age of 46 – 59 years who were homogeneous with respect to the traditional cardiovascular risk factors. As the group surveyed patients with CHD debut at the age of 60 years and older was significantly different from the above groups on traditional cardiovascular risk factors such as diabetes, obesity or overweight, and smoking , it was excluded from the analysis.
Analysis of the distribution of genotypes of A603G polymorphism of tissue factor gene in patients with different age of CHD debut showed the following: G603G genotype was detected in 28 of 58 (48%) patients with age of onset of the disease of 45 years or younger, while only in 74 of 203 (36 %) persons with a debut at the age of 46 – 59 years. Thus, G603G genotype was significantly more frequent in patients with the debut of the disease at the age of 45 years and less than in the group with the older age, with no statistically significant effect on the risk (p = 0,049; OR=1,61, CI:0,83÷3,1, Table 6).
Table 6. Distribution of A603A, A603G, G603G genotypes and frequency of alleles G and A of A603G polymorphism of tissue factor gene in CHD patients with different age of the disease debut| Observed groups | Genotype of tissue factor gene | Allele frequency | |||
| А.A603A | В.A603G | С.G603G | A | G | |
| 1. Debut of CHD at the age of 45 years and younger (n=58) | 10(17,2%) | 20(34,5%) | 28(48,3%) | 400,34 | 760,66 |
| 2. Debut of CHD at the age of 46 – 59 years (n=203) | 34 (16,7%) | 95(47,0%) | 74(36,3%) | 1330,4 | 2430,6 |
| p(1((A+B)vsC),2((A+B)vsC)) | 0,049 | 0,071 | |||
| OR(1((A+B)vsC),2((A+B)vsC)) | 1,61, CI:0,83÷3,1; P = 0,157 | —– | |||
One of the most important pathophysiological mechanisms of activation of PPAR-α is the suppression of the expression of tissue factor, resulting in an extremely important study of gene-to-gene interactions of L162V polymorphism of PPAR-α gene and A603G polymorphism of tissue factor gene.
The combination of L162V genotype of PPAR-α gene and G603G genotype of tissue factor gene was detected significantly more often in CHD patients compared to the control group without CHD than other combinations of genotypes of observed gene polymorphisms (L162V / G603G genotypes – 17 of 314 (5,4%) of CHD patients and in 4 of 220 (2,5%) individuals in the control group, and was associated with an increased risk of CHD development in 3,04 times (OR = 3,04; CI: 1,01 ÷ 9,16).
Discussion
This Study was Conducted as Part of an Extremely Important Now Personalized Cardiology.
According to the Framingham study, the incidence of carriage of L162V polymorphism of PPAR-α gene in the general population was 6,9% 15. Thus, the occurrence of this genotype was twice as high (14%) in the group of CHD patients than in the population of the Framingham study and in the control group of persons without CHD.
Carriage of L162V genotype and V allele of studied polymorphism was detected significantly more often in CHD patients and was associated with an increased risk of CHD in 2,13 times (L162V genotype) and in 2,21 times (V allele) when compared with the control group without CHD. These findings echo the results obtained by A. Skoczynska and co-workers 16, which showed that the V allele of investigated polymorphism was detected in patients with angiographically verified coronary atherosclerosis in four times more likely.
In the works of many authors there are conflicting results about the relationship of the studied polymorphisms with risk of myocardial infarction. So, Reinhard W. and co-workers found no association between the L162V polymorphism and the risk of myocardial infarction in 2008 17.
L162V PPAR-α gene genotype was detected significantly more often in patients with coronary heart disease with the debut of the disease at age 45 or younger and was associated with an increased risk of coronary heart disease at the age of 45 years or less. V allele was detected significantly more often in patients with CHD and age onset of the disease 45 years or less, and his carriage was associated with increased CHD risk. Similar results were obtained in a prospective study Northwick Park Heart Survey 18, in which the connection was established of PPAR-α L162V genotype with the early development of coronary heart disease in patients of the North-West region of Europe. These results are consistent with two major clinical studies Helsinki Heart Study 19 and the Veterans Affairs High-Density Lipoprotein Intervention Trial 20, that proved pathogenetic significance of PPAR-α in the development of CHD destabilization. These studies have demonstrated the clinical significance of modulating the activity of PPAR-α in the development of algorithms for the prevention of acute coronary syndrome using fenofibrate. Treatment with this drug reduced the risk of acute coronary syndrome by 34%.
V allele of PPAR-α gene is associated with reduced transcriptional activity 21. This in turn leads to a decrease in the affinity to the relevant receptor ligands and antiatherogenic decrease PPAR-α effect on lipid metabolism and immune inflammation factors.
G603G genotype and G allele were detected significantly more often in patients with coronary heart disease than in the control group without CHD, and his carriage increased the risk of CHD in 2.68 times (G603G genotype) and 4.37 times ( G allele). The data are comparable with the results of a study carried out by I. Ott and co-workers 22, finding that the G allele carrier prevailed in patients with coronary heart disease when compared to the control group.
Carriage of G603G genotype and G allele were detected significantly more often in patients with onset of the disease at the age of 45 years and less than in the older age groups, with no statistically significant effect on risk. Unfavorable course of coronary heart disease may be due to a higher concentration of plasma tissue factor in heterozygous carriers of G allele with increased blood protrombogennogo potential 22.
Recent studies have shown the role of tissue factor in triggering acute coronary syndrome, that allows us to consider it as a new biomarker of risk for coronary heart disease and myocardial infarction. The level of tissue factor serum was significantly higher in patients with coronary heart disease than in the general population. According to data obtained H. Soejima and co-workers in 1999 23, the growth of levels of tissue factor is one of the predictive factors of cardiovascular events.
In this study, the level of tissue factor serum was significantly higher in patients with coronary heart disease - carriers G603G genotype compared with native A603A genotype. This, apparently, shows the presence of ischemic heart disease patients - homozygous carriers of G allele of the gene in tissue factor procoagulant chronic status.
The intact endothelium prevented direct contact with the bloodstream of tissue factor. In the case of activation of immune inflammation in the vessel wall the endothelial damage occur. The result is the release into the bloodstream of a large amount of tissue factor and start the coagulation cascade 24, 25.
This G603G genotype was associated with unfavorable features of CHD described above. Perhaps this is due to increasing levels of tissue factor with formation of chronic procoagulant status and increased risk of thrombosis.
As shown above, the combination of L162V genotype L162V polymorphism of PPAR-α and G603G genotype A603G polymorphism of tissue factor alone was associated with an increased risk of coronary heart disease. These results can be explained by the fact that one of the most important pathophysiological pathways activate PPAR-α is the suppression of expression of tissue factor 14. It is known that L162V polymorphism PPAR-α decreases the affinity of the receptor to the corresponding ligands, which not only leads to disturbances of lipid metabolism, and activation mechanisms of immune inflammation in the vascular wall, but also prevents the inhibition of the expression of tissue factor, which is already high in carriers prognostically G603G unfavorable genotype tissue factor gene. As a result of increased procoagulant potential of circulating blood.
Thus, it inhibits the ability of PPAR-α to reduce the expression of tissue factor by inhibition of NF-κB pathophysiological way 26. This, in turn, leads to an increase prokoagulyat and proinflammatory properties of blood plasma in patients with coronary heart disease - carriers of the above-mentioned adverse prognostic paired combinations of genotypes.
Conclusion
A carriage of V allele of L162V polymorphism of PPAR-α gene and G allele of A603G polymorphism of tissue factor gene, as well as their combination are associated with an increased CHD risk, especially at age 45 years or less.