Abstract
Frailty describes a medical syndrome that confers increased vulnerability to disproportionate changes in health status following minor stressors. With loss of homeostatic reserve in multiple physiological systems, frailty conveys an increased risk of adverse health outcomes. Despite the lack of a clear universal definition, the utilisation of two landmark operational models has allowed a rapid expansion in frailty-centred research.
The pathophysiology of frailty is yet to be elucidated in the literature, but a critical role for a heightened inflammatory state is hypothesised. Raised levels of pro-inflammatory cytokines are associated with frailty, with emerging evidence relating their biochemical action with development of the frailty phenotype.
Dysregulation of both the innate and adaptive immune system are key components of the frailty syndrome. Remodelling of the T cell compartment and upregulated inflammatory pathways are theorised to propagate the heightened inflammatory state critical in the frailty syndrome. Increased neutrophil counts, in conjunction with ineffective neutrophil migration associated with age, is theorised to produce tissue damage and secondary inflammation conducive of the inflammatory picture in frailty.
Beyond the gold standard of the comprehensive geriatric assessment, management of frailty is a fast-evolving area of research. Exercise interventions have shown promising results, improving functional ability and showing beneficial immunomodulation. Vitamin D supplementation, with proposed anti-inflammatory effects, nutritional support and pharmacological treatments all provide promising areas for future therapeutic intervention.
Author Contributions
Academic Editor: Roman Kireev, Senior Researcher
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 William Drew, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Frailty and the Frail Immune System
Frailty is a syndrome characterised by the loss of homeostatic reserve in multiple physiological systems. It is a serious issue for an increasingly elderly population that is associated with increased vulnerability to dramatic health changes in response to often minor stressor events 1. Described as the most problematic consequence of population ageing2, frailty conveys an increased risk of adverse outcomes, including falls, disability and mortality. The resultant burden on both health and social care systems globally is only set to increase in an internationally ageing population3, 4. Now recognised as a clinical syndrome disparate from disability and comorbidity5, the importance of identifying and introducing effective management for patients with frailty is becoming increasingly evident.
Defining Frailty
The term “frailty” has been used previously to describe a whole host of conditions, ranging from general debility, bone weakness to cognitive impairment6, 7. However, over the last 20 years, frailty as a concept has evolved to be defined as a distinct clinical syndrome, widely recognised as a vital diagnosis due to its association with poorer clinical outcomes and increased health care utilisation. Despite this, there is still no universal consensus for the classification of frailty as a syndrome. Currently, there are two widely accepted operational definitions: the frailty phenotype model and the frailty index model, compared in Table 1.
Table 1. The Frailty Phenotype and Frailty Index operational models of the frailty syndrome. With the lack of a single unifying definition, these two operational models provide the definitions of frailty used in research and clinical practice. The frailty phenotype model identifies an individual as frail by the presence of three of the five symptoms shown above. An individual is classed as pre-frail if they exhibit one or two of the symptoms. The frailty index model classifies an individual as frail if their number of deficits, as a proportion of the total deficits assessed, is greater than 0.2. Deficits can include any variable that is associated with ill health, increases in prevalence with age but does not saturate (≥1%) at old age.| The Frailty Phenotype Model Fried 9 | The Frailty Index Model Rockwood 14 |
| 3/5 of the following:Weight lossSelf-reported ExhaustionLow physical ActivitySlownessWeakness | Deficit accumulation of >0.2 of total assessed deficits (minimum 30)Deficits can include any variable that fulfils the following criteria:Associated with adverse health outcomesIncreased in prevalence with agePrevalence ≥ 1% (but not saturated) in old age |
The phenotype model, more widely utilised in research8, was pioneered by Fried9. It states that frailty can be thought of as a clinical phenotype incorporating five features: shrinking (unintentional weight loss), poor endurance and energy (self-reported exhaustion), low physical activity level (low energy expenditure), slowness (slow gait speed) and weakness (weak grip strength)9. Individuals with three or more of these features were classified as frail, one or two features as pre-frail. Frailty classified in this way was shown to correlate with an increased risk of adverse outcomes, including falls, mobility and function, hospitalisation and death 9. This association was shown to hold true in different and more diverse cohorts such as a Chinese cohort 10.
The frailty index model was pioneered by Rockwood and describes frailty as the cumulative effect of individual deficits 11. Patients with more deficits were more likely to be frail 11 and were at an increased risk of adverse outcomes including mortality 12, 13. Deficits were classified as 92 variables, originally identified to classify health status in the elderly14. These variables include symptoms and signs, functional impairments and laboratory abnormalities covering a wide range of domains such as social, psychological and medical. The frailty index itself is calculated as the presence (score of 1) or absence (score of 0) of each variable as a proportion of the total. An index above 0.2 is classified as frail. At an index of 0.65, the deficit accumulation is not sustainable with life15. This model of frailty produces a gradation between frailty and good health. It recognises that frailty is not just a phenomenon that is present or absent, but usually presents as a gradual decline into increasing frailty. The frailty index is seen as mathematically attractive, with a distribution similar to that seen in systems with in-built redundancy 2 This supports the theory of an accumulation of deficits leading to reduced homeostatic reserve, resulting in the vulnerability which is fundamental to the frailty syndrome2. Rockwood’s theory has since been refined to a more manageable 30 variables, without losing validity in different data sets 16.
Despite the two vastly different approaches to characterising frailty, both approaches show statistical convergence17. Although each model has their advantages; the Frailty index can identify risk of adverse outcomes from intermediate frailty more specifically and lead to more targeted treatments 17. The two models are distinct but complimentary, with their combined/sequential use encouraged 18.
Frailty, co-morbidity and disability are three inter-related clinical entities, which only recently were proven to be distinct. Recent research has shown that there is consistently a population of frail individuals without co-morbidities or disability 5,19,20. Despite this, the conditions overlap extensively, as a result of causal relationships between the three. Frailty often precedes disability 21, whilst disability and co-morbidity can contribute to the development of frailty 5.
Reports on the prevalence of frailty vary from study to study due to a lack of a universal, corroborated definition of frailty. A systematic review of 21 studies yielded a weighted average prevalence of 10.7% in community dwelling older adults (aged 65 and older) 22. However, this review was subject to a wide variation in reporting, resulting in huge disparity in prevalence estimates between the included primary studies. What was clear however, was the close association with age, with around a quarter of individuals over the age of 85 classified as frail 22. There was also a clear association with gender, frailty being more prevalent in women that is independent of age 22.
Pathophysiology
Despite continued research efforts, the clear pathogenesis of frailty is still yet to be elucidated. Principally, the pathogenesis and progression of frailty is associated with accelerated accumulation of cellular and molecular damage in multiple bodily systems. This damage occurs naturally in normal ageing 23, and most body systems have in built redundancy (or physiological reserve) which can account for decline in age or disease 24. However, there is a threshold of damage, beyond which impaired body system function becomes evident. Frailty manifests in an individual who has crossed the threshold of damage in multiple physiological systems 25. Importantly, the number of body systems affected, rather than the amount of damage in one system, is the strongest predictor of frailty 25.
The main three systems focused upon in frailty-centred research are the immune system, endocrine system and nervous system 6. However, changes in multiple body systems have documented impacts on the frailty syndrome including: the renal system 26, the cardiovascular system 27, 28, the haematological system 28, 29 and the respiratory system 30.
There are a number of associated factors that potentially contribute to the pathogenesis of frailty, but these are sparsely illustrated and without a significant evidence base in the literature. We can postulate that chronic low-level inflammation has a key pathophysiological role 31, 32 as the inflammatory markers IL-6, TNFα and CRP, are elevated in frailty 33, 34, 35 There is also a direct association between frailty and an increased total white blood cell count at baseline 35, a routine clinical indicator for systemic inflammation 36. This chronic inflammation has both indirect and direct contribution to the pathophysiology of frailty. IL-6 and TNFα themselves show association with the loss of muscle mass strength in frailty 37. Inflammation has detrimental indirect effects on intermediary systems including decreased haemoglobin concentrations 38, insulin-like Growth Factor (IGF) levels 39 and micronutrient concentrations40. These effects reduce the physiological reserve of the affected bodily systems, contributing to the development of frailty.
Sarcopenia is the loss of skeletal muscle mass, strength and function41, which occurs age. With weakness and slowness comprising a key part of the frailty phenotype, sarcopenia and frailty are understandably very closely linked. Many even describe sarcopenia as ‘physical frailty’. However, we can hypothesize that sarcopenia is not only a component of frailty but it can actively cause or encourage the progression of frailty. Sarcopenia itself is associated with a chronic low level inflammatory state driven by oxidative stress and inflammatory cytokines, with raised levels of IL-6, TNFα and CRP, all considered key in the condition’s pathogenesis 42, 43. The development of sarcopenia can lead to a cycle of reduced physical activity, under nutrition and further inflammation that is extremely difficult to break 44, 45. These factors have all been implicated in the pathophysiology of frailty suggesting a causative role for sarcopenia. The endocrine system is also believed to be fundamental in the pathogenesis of sarcopenia and consequently frailty. The decrease of oestrogen or testosterone in old age36 and reduced levels of IGF-1 in frail individuals 46 can result in sarcopenia. The close relationship between sarcopenia and frailty has been postulated to extend to the molecular level, with the dysregulation of the PI3K-Akt signalling proposed to play a role in the pathophysiology of both processes47.
The Frail Immune System
The chronic pro-inflammatory state associated with frailty 31, 32, 33, 34, 35 is accompanied by dysregulation in both the adaptive and innate immune systems 32. Whether these changes are cause or consequence of frailty is the topic of ongoing research and not yet elucidated in the literature.
As stated above, there is an association between frailty and raised levels of IL-6 and TNF-α 33, 34, 35, as part of the heightened inflammatory state accompanying the syndrome. These inflammatory cytokines play a crucial role in the pathogenesis and propagation of the frailty syndrome. IL-6 can cause muscle degradation in a number of ways: directly by action of the proteasome 48, through induction of insulin resistance 49 resulting in suppression of skeletal muscle hypertrophic Akt-mTOR activity 47, 50 and also through the induction of 11βHSD1 51 which synthesises the catabolic molecule cortisol 52. These processes are evident in human epidemiological studies which have shown that higher levels of IL-6 are predictive of both sarcopenia 53 and relevant frailty associated adverse health outcomes 54. TNFα can directly induce skeletal muscle wasting 55. This is especially relevant as TNFα levels in the skeletal muscles of frail older adults were shown to be elevated when compared to healthy younger individuals56. With regards to the impact of anti-inflammatory cytokines, there is a lack of evidence regarding an association between human frailty and IL-10. However, we can hypothesise that the molecule is involved in the syndrome’s pathogenesis and maintenance, with murine models of frailty utilising an IL-10 knockout model 57.
Evidence is emerging that the T cell compartment of the adaptive immune system undergoes remodelling in frailty syndrome. Age matched female patients who were frail have been shown to have significantly more CD8+CD28- and CD8+ T cells than non-frail women58. Furthermore, dysregulation of CD4 T cells has been shown to be predictive of a frailty-related phenotype in HIV infected men 59. These findings suggest that T cell dysregulation may well be associated in the frailty syndrome. This is reinforced by the finding that frail individuals have increased counts of T cells expressing chemokine CC receptor 5, representing an increase in a pro-inflammatory T-cell subset in frail older adults 60 perhaps contributing to the chronic inflammation in frailty. Further studies of the quantity, character and function of T cells in frail individuals are needed. Information regarding B cell function in frailty is extremely limited. There is emerging evidence that individuals with frailty have an impaired response to vaccination, but it is unclear whether this is secondary to the previously described T cell dysregulation or dysfunction in the B cell itself 32.
The innate immune system of frail individuals exhibits increased cellular and molecular inflammatory markers32. Increased IL-6 production by peripheral blood mononuclear cells (PBMCs) 61, 62 and elevated white blood cell count are both associated with frailty35, 63. We can postulate that these factors are crucial in the maintenance of the heightened inflammatory state seen in frailty. There is also evidence to show an upregulation of the CXCL10 gene in the monocytes of individuals with frailty64, as well as upregulation of other inflammatory pathway genes 65, further potential causes of the heightened inflammatory state in frail older adults. An association between oxidative stress, cellular senescence and frailty has been proposed, following the observation of increased expression of hydrogen peroxide-induced clone 5 (a protein that responds to oxidative stress and is key in cellular senescence) in monocytes of a frail individual 32.
Systemic neutrophil and monocyte counts have been shown to be raised in frailty 63. However, neutrophil chemotactic ability declines with age 66, 67 as does the ability of neutrophils to phagocytose bacteria 68or produce extracellular traps 69. Neutrophils, although crucial in bacterial clearance and tissue repair, can cause tissue damage as evidenced by the attenuation of muscle injury elicited on leukocyte depletion 70, 71, 72 Thus, in frailty we can postulate that an increased number of neutrophils, migrating inefficiently, and with reduced capacity to effectively clear bacteria might cause tissue damage and produce systemic inflammation 66, 67, potentially providing significant input to the heightened inflammatory state and muscle damage seen in frailty.
Management of Frailty
According to the British Geriatrics Society, a Comprehensive Geriatric Assessment (CGA) reflects the gold standard of care for patients with frailty 73. Frail patients admitted to hospital who received a CGA were more likely to return to their homes, less likely to suffer deterioration or death and showed improved cognition 74. The key components, first described by Rubenstein 75, are: co-ordinated multidisciplinary assessment, geriatric medicine expertise, identification of medical, physical, social and psychological problems and the formation of a care plan 74. The main limitation of the CGA is its resource intensive nature which can restrict its incorporation into practice.
As far as interventions to prevent or reverse frailty itself, there is currently limited available research. Therefore, to improve our understanding we have also considered studies have been conducted in populations that, although not explicitly categorised as frail, may well have been frail at the time of data collection. Exercise interventions of various types have shown promising results in the literature. Systematic reviews on the topic suggest that exercise may improve functional ability and decrease disability76, 77 in moderately frail individuals, but not in the severely frail 76. In these reviews, exercise was defined as activity requiring physical effort that is intended to improve or maintain fitness76, 77. The review conducted by Clegg et al 76 focused on home-based resistance exercise interventions, whereas the review conducted by Theou et al 77 encompassed both resistance and multicomponent interventions. The effects of resistance exercise in particular seem promising in clinical trials, reducing physical decline78 and counteracting the weakness associated with physical frailty 79. There is a growing body of evidence for the use of exercise to reduce the chronic low level inflammation critical in frailty42, 80. Resistance exercise in particular has been shown to modulate the immune system in frail older adults, reducing TNFα levels in skeletal muscle and permitting increased muscle protein synthesis 56. A Cochrane review of patients in long-term residential care, who are likely to be frail, suggests that physical rehabilitation can reduce disability and improve physical condition 81. This was supported by a separate meta-analysis that found that mobility and physical functioning was improved with physical exercise therapy in an older population with mobility issues 82. However, an update of the Cochrane review highlighted the difficulty of drawing valid conclusions using meta-analysis from such varied datasets and interventions but did suggest that individual studies have demonstrated benefit to health status with physical activity 83. The effect of exercise on the quality of life remains uncertain, with no conclusive evidence on the subject76, 82 High-intensity exercise seems to be the most effective when compared to low intensity exercise 79, 82 but there was insufficient evidence to make a strong recommendation 77.
Another potential treatment for frailty is nutritional and hormonal support. Caloric and protein support as well as Vitamin D replacement are both listed in the Frailty Consensus from 2013 84 as potential therapies for physical frailty. Protein supplementation has been shown to improve grip strength and reduce weight loss85. Protein supplementation has also been shown to improve physical performance in frail elderly volunteers 86 especially when combined with resistance exercise87, 88. A reduced Vitamin D level has shown strong associations with both prevalent and incident physical frailty after adjusting for common confounders 89. Vitamin D supplementation can reduce the risk of falls 90 improve strength 91 and reduce mortality 92 in older patients. However, it is worth noting that there is conflicting evidence regarding the benefit of vitamin D supplementation, with recent research suggesting that high dose supplementation can increase the risk of falls in older adults 93. This disparity in the literature on vitamin D supplementation may be due to inexpert targeting of the treatment and once the mechanism of action is better understood, studies may be able to show increased benefit. Recent research efforts have explored the immunomodulatory effects of vitamin D and its potential use in the treatment of inflammatory diseases94, 95, 96, 97 The anti-inflammatory effect of vitamin D on human immune cells is well documented, with reduced production of pro-inflammatory cytokines 98, 99. With the effect of vitamin D supplementation on inflammation currently being investigated 100, we can hypothesise that vitamin D supplementation could produce beneficial modulation of the frail immune system. Despite the lack of large-scale trials assessing the efficacy of vitamin D supplementation at preventing frailty directly, the limited evidence for immune modulation in a frail population and the conflicting evidence for its use in fall prevention, it provides a promising area of research for therapeutic intervention.
No substantial body of research supports other pharmacological treatments for frailty. It has been suggested that Angiotensin Converting Enzyme inhibitors (ACEi) can improve muscle structure 101 and prevent the decline in muscle strength 102. The LACE Trial 103, which is currently ongoing, is set to examine whether ACEi can be used to treat sarcopenia. However, this has not been examined in frailty or in enough details to make recommendations for clinical practice. ACEi have also been shown to produce anti-inflammatory effects in multiple patient groups 104, 105. Whether the anti-inflammatory effects of ACEi would prove beneficial in reducing the heightened inflammatory state present in frailty will need further investigation. Testosterone can improve strength, but carries with it significant risk of cardiovascular adverse events 106. IGF-1 administration affects skeletal muscle directly but has no proven effect on muscle strength 107.
Figure 1. The theorised influence of a heightened inflammatory state on the pathogenesis of the frailty syndrome. The chronic pro-inflammatory state manifest in frailty can lead directly or indirectly to the development of frailty and consequently the associated adverse health outcomes (depicted in red). This inflammatory picture can affect intermediary systems; sarcopenia and the decline of the musculoskeletal system associated with frailty pathogenesis. The remodelling of both the innate and adaptive immune systems associated with the frailty syndrome plays a key role, but whether this is cause or consequence is yet to be decided. Promising management options (depicted in blue) are emerging in the literature, providing beneficial immunomodulation and improving functional outcomes. 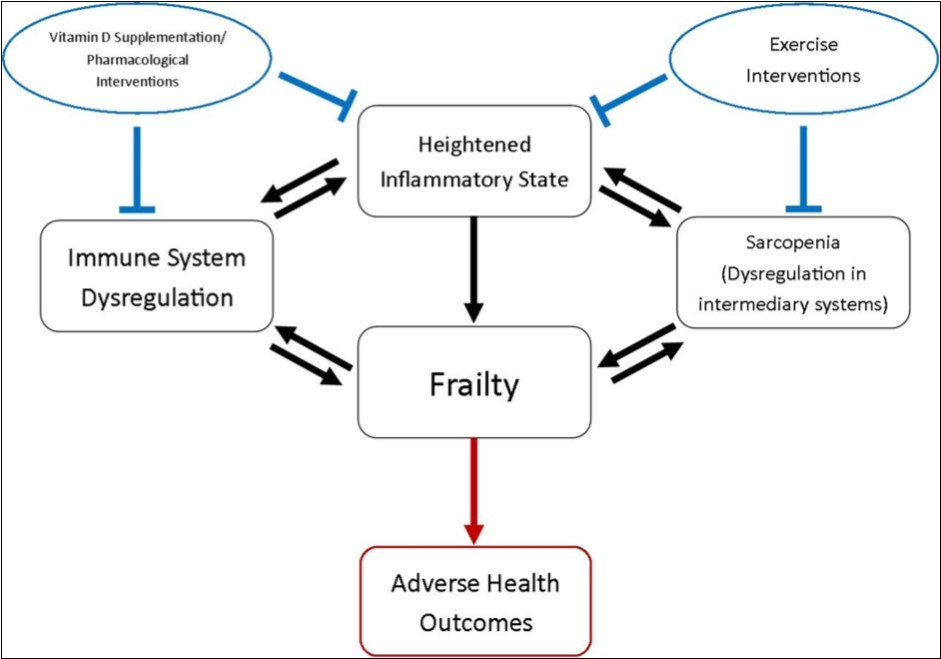
Figure 1 provides a summation of factors that have been implicated in the pathogenesis of frailty and therapeutic strategies that might improve patient outcomes.
Conclusion
Frailty is a medical syndrome with increasing importance in global health care. Associated with an increased risk of adverse outcomes in older adults, its identification and appropriate management is essential for effective patient care. Continued research efforts will further our knowledge regarding the syndrome’s complex pathophysiology and potential for curative management and therapeutics strategies. The immune system is hypothesised to have a key role in the pathogenesis of frailty, with significant changes observed in the immune systems of individuals with frailty. However, whether these changes are cause or consequence will be the subject of further research.
Acknowledgments
William Drew would like to express his gratitude to the Arthur Thomson Trust for financial support in the form of an Intercalation Bursary. Daisy Wilson is supported by a clinical research fellowship funded by the MRC-Arthritis Research UK Centre for Musculoskeletal Ageing Research. Elizabeth Sapey is funded by the Medical Research Council.