Abstract
A health financing perspective examines fairness in financial contribution, considering risk pooling, progressive funding, and protection against catastrophic spending.
Author Contributions
Academic Editor: Omnia Hamdy, National Institute of Laser Enhanced Sciences, Cairo University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Javad Javan-Noughabi
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction

Health care systems are responsible for providing preventive, therapeutic and rehabilitation services 1. But, payments for this services must be according to ability to pay 2. Thus, the World Health Organization (WHO) developed the concept of Fairness in financial contribution (FFC) as a one of the three main goals of a health systems 3. Before we describe the FFC, we must first define the household’s Capacity to pay ( ). Household’s Capacity to pay is defined as household’s total expenditure (
). Household’s Capacity to pay is defined as household’s total expenditure ( ) minus household’s subsistence expenditures (
) minus household’s subsistence expenditures ( ) or household’s food expenditure (
) or household’s food expenditure ( ) (if
) (if  ).
).
 if:
if: 
 if:
if:
The ratio of a household’s out-of-pocket (OOP) payments for health to their capacity to pay is defined as the household financial contribution (HFC).
Finally, the FFC index formula is as follows:
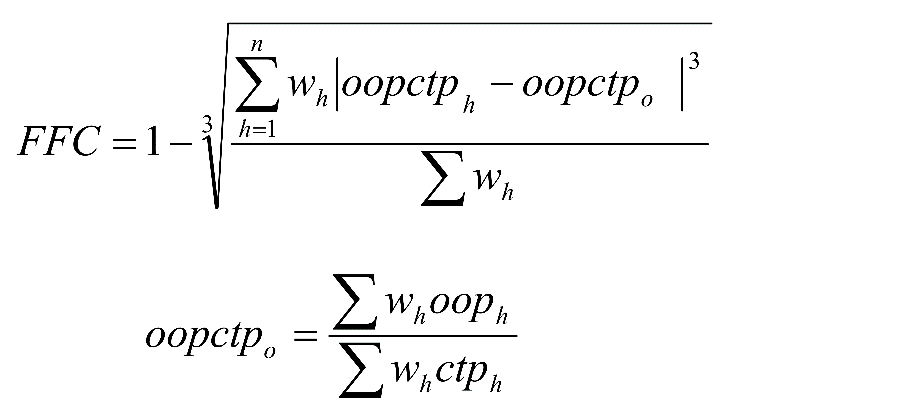
The range of FFC index is between 0 and 1. 1 represents the most fairness and 0 represents the most unfairness 4.
Fairness in financing contribution will be achieved if all households pay an equal share of their capacity to pay for health. If HFC exceeds a certain threshold, catastrophic health expenditures (CHE) will be occurred. Based on WHO criteria, CHE occurs when out-of-pocket (OOP) payments for healthcare are more than or equal to 40 % of a household’s capacity to pay (HFC>40%) 4. The lack of prepayment mechanisms for risk pooling and low household capacity to pay are the main factors that increase the possibility of the exposure to catastrophic expenditures 5.
Healthcare Financial Mechanisms
CHE is directly related to OOP and indicates the inappropriate health coverage. OOP is the most unfairness and regressive mechanism of healthcare financing without any risk pooling 3. The literature showed that every year, more than one hundred million people suffered from catastrophic health expenditures due to OOP payments, especially in developing countries 6. OOP payments are including medical direct, non-medical direct and indirect costs. The probability of the CHE increases when non-medical direct and indirect costs are taken into account 7.
The World Bank noted that, “By 2030, no one should fall into poverty because of out-of-pocket health care expenditures” 8. Also, World Health Day 2018 named as ‘Universal Health Coverage: Everyone, Everywhere’ 9. As a result, healthcare financing should be based on financial risk-protection mechanisms such as general taxation and social insurance. Studies showed that the coverage by health insurance reduces the probability of occurrence of CHE 10, 11, 12, 13, 14. However, Insurance can significantly increase the risk of incurring catastrophic health care expenditures through “moral hazard”. Moral hazard defined as increases the rate of health care utilization due to lowering the cost of health care 15.
Capacity to Pay
Household income level is a key factor affect the capacity to pay that have an inverse association with CHE 16. Generally, Rural and poorer households are at higher risk of catastrophic health expenditures 16, 17. Studies showed that households with four or more members were less likely to experience CHE 13, 16, 18. The prevalence of CHE is higher in Households headed by older and unemployed people 10. Having the chronic illness among household members increase the likelihood of CHE. This factor affect the both of OOP and CTP 18.