Abstract
Basal cell carcinoma (BCC) is the most common type of skin cancer, which arises from the basal layer of the epithelium. It is a slow growing tumor and has a low metastatic potential, it accounts for 70–80% of all cutaneous malignancies in the head face and neck region .Defects near nasal tip and ala of the nose are one of the most difficult site to cover in a single stage, bilobed flap is reported to be used very effectively to close the defect in these areas. This article reports a case of basal cell carcinoma involving the ala of the nose which was excised and the reconstruction was done using bilobed flap.
Author Contributions
Academic Editor: ANGELA PIA Cazzolla, Department of Dentistry and Child Complex Operating Unit of Dentistry at the University of Bari, Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Surej Kumar L.K, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Basal cell carcinoma (BCC) is a slow growing, locally destructive, malignant tumor of the skin. It is derived from nonkeratinizing cells that originate from the basal layer of the epidermis and was first described in 1824 by Jacob 1Although basal cell carcinoma is a malignant neoplasm, it rarely metastasizes. The incidence of metastatic basal cell carcinoma is estimated to be less than 0.1%. Nasolabial flap, median forehead dorsal nasal flap, glabellar flaps,bilobed flaps, cheek and craniofacial flaps are used for nasal reconstruction.
In this case report a defect measuring 2.5 cm diameter following excision of a basal cell carcinoma in the left ala of the nose was reconstructed with a bilobed flap2, 3, 4.
Case Report
A 50 year old female patient reported to our department with complains of circular black discoloration on the left side of the nose, the discoloration has been slow growing and has reached the current state in a span of 3 years (Figure 1).There was no pain associated with it, but was aesthetically concerned with the lesion .Surgical excision and reconstruction of defect using bilobed flap was planned under general anaesthesia.
Figure 1. Preop clinical Photograph
Standard Markings for the bilobed flap design were done and excision of the lesion was carried out 2 mm from the margin of the tumor (Figure 2). The excised lesion was sent for histopathological examination.
Figure 2. Surgical Excision of the defect
Reconstruction was performed using modified bilobed flap. The flap was designed (Figure 3) in such a manner that the flap could be turned over the defect on the ala of the nose and closure of the donor site could be done primarily without deformity.
Figure 3. Orientation of Bilobed Flap design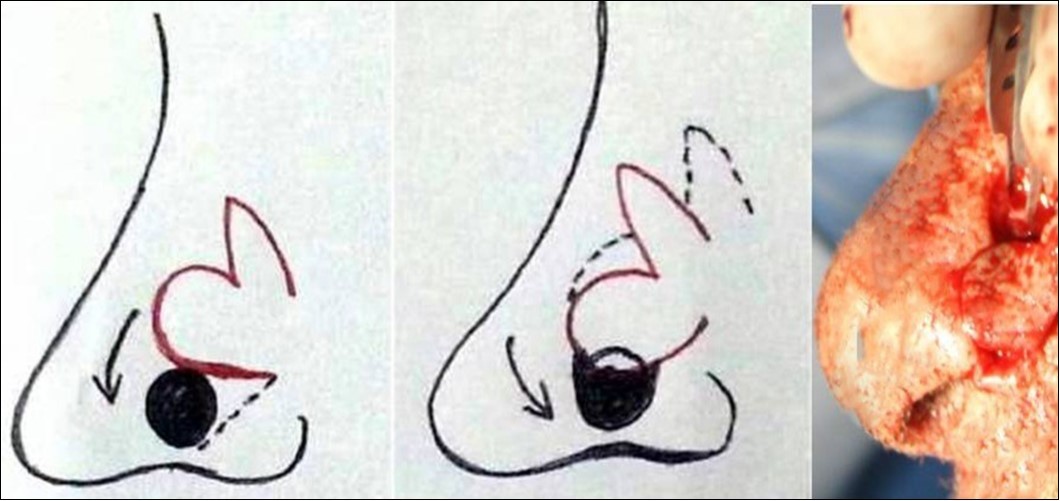
The area surrounding the Ala of nose was infiltrated with 2% lignocaine with 1:200000 adrenaline. The flap was raised based on the size of the defect to be covered, the central lobe of the flap was rotated into the primary defect (Figure 4) and the secondary defect was closed primarily by direct suture (Figure 5). The patient has been followed up for 3 years with no evidence of recurrence.
Figure 4. Approximation of defect using bilobed flap prior to closure
Figure 5. Closure of Defect
Discussion
The principles of management of BCC include early detection, complete removal of the lesion and careful follow-up to detect recurrence or new primary tumours. The choice of treatment should be determined based on the histological type of lesion, its size and location, patient age and medical condition of the patient. Treatment of basal cell carcinoma can be surgical or non-surgical. Surgical techniques include excision, curettage & cautery, cryosurgery and Mohs’ micrographic surgery. An excision margin of 4 mm around the tumor is recommended where possible. The main advantage of surgical excision is that excision margins can be examined histologically to check for tumor clearance. In contrast, no tissue is available for histological examination after cryosurgery, while curettage samples do not provide adequate tissue to be able to examine tumor margins histologically. Furthermore, both cryosurgery and curettage & cautery can result delayed wound healing when compared to excision 5, 6.
The surgical defects near the nasal tip and ala of the nose is one of the most difficult sites to cover with a flap in a single stage, the bilobed flap can used very effectively to close the defect in these areas 2. Aesthetics will be compromised when free skin grafts are used even though it provides a good covering of the wound but as such it will not replace the defect2.Next in reconstructive ladder is the use of local flaps, they are the choice of treatment for reconstruction of the alar defect of the nose since it is a smaller defect and will not have much of esthetic problems. The way the flap is used and the timing of the reconstruction depends very much on the nature of lesion and the type of defect3.
Esser7 was the first person to describe bilobed flap in 1918 as an ideal structure for closing defects in the nasal tip. It was popularised by Zimany8 in 1953 where he published a description of this flap in the English literature. It is a double transposition flap with a single pedicle in which the first flap is transposed into a defect and the second, smaller flap is transposed to fill the secondary defect caused by the larger flap transposition. Thus, the forces of tension are distributed in various directions, and the skin distortions and redundancy generated by a simple transposition flap or by primary closure are reduced. Zitelli9 In 1989, methodized the bilobed flap for the reconstruction of defects in the nasal tip and alar.
Various other authors10, 11 introduced changes in sizes and lobe angles in order to reduce the incidence of distortion in the tip and alar retraction. Subsequently the defects in other anatomical sites have been repaired using the bilobed flap12.
The advantage of bilobed flap is that it enables the closure of defect with no or minimal distortion of the surrounding tissues and it also allows the transfer of skin with similar colour and texture. It can be randomly or axially applied, structured in a skin or as fasciocutaneous and myocutaneous manner, and is easy to perform. Because of the above mentioned advantages, it can be applied in other regions of the face, neck, trunk, and limbs.
Its ability to close defects of different sizes and in different regions with the same ease and efficiency shows the versatility of the flap. The various modifications from its initial introductory design has made its implementation easier and improved its outcomes. This progressive evolution enables surgeons to be more innovative when it comes to choosing the lobe sizes and angles and that the term “bilobed” highlights not only the flap but also the principle of tissue transfer.
Conclusion
Bilobed flap has brought in new dimensions to the world of aesthetic surgery; it has reduced the burden on the surgeons in the difficult and challenging task of reconstruction of nasal defects. The main advantages of this flap include the similarity in colour and texture in relation to the site of the defect, easy reproducibility, the low rates of complication and the possibility of designing it in different sizes and tissue compositions. All these makes bilobed flap truly versatile in all ways.