Abstract
This report presents a case of collision tumors of low-grade B-cell lymphoma and poorly differentiated adenocarcinoma in the caceum of a 63-year-old woman. Lymphoma was diagnosed incidentally after appendectomy for a clinical presentation of acute appendicitis. Imaging follow-up demonstrated mesenteric lymphadenopathy and liver lesions, and all surgically resected regional mesenteric lymph nodes and liver biopsy were found to be infiltrated by both mucosa-associated lymphoid tissue (MALT) lymphoma and adenocarcinoma. Systemic chemotherapy was administered for advanced colonic adenocarcinoma with liver metastases. The occurrence of synchronous lymphoma and adenocarcinoma of the colorectal region is rare, and this is a previously unreported case of a patient that was diagnosed during management of acute appendicitis.
Author Contributions
Academic Editor: Anil Tombak, Faculty of Medicine, Turkey.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Kara T, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Collision tumors of lymphoma and colorectal adenocarcinoma are rare entities and just a few studies exist 1, 2, 3, 4, 5, 6, 7, 8 in the literature. In the case of mucosa-associated lymphoid tissue (MALT) lymphoma which is now known as marginal zone lymphoma MALT type, the gastrointestinal tract is the most frequently involved extranodal site with the stomach being the most common location 7. Primary lymphoma of the colon is rare, comprising only 0.2% to 1.2% of all colonic malignancies 9, and colonic lymphomas represent 5.6% to 20% of all gastrointestinal lymphomas 10. Furthermore, lymphoma synchronously accompanied by adenocarcinoma of the colon is extremely rare 6. Review of literatures revealed no reports of simultaneous occurrence of colonic adenocarcinoma and MALT lymphoma that was diagnosed during management of acute appendicitis as is presented below.
Case Presentation
A 63-year-old woman presented to the Department of General Surgery as an outpatient with abdominal pain. Physical examination showed the signs of acute appendicitis and appendectomy was performed. During microscopic examination, a small focus of atypical monotonous lymphoid cell population was seen and the material was sampled totally. The pathological examination revealed MALT lymphoma (Figure 1), with diffuse positivity of cluster of differentiation (CD) 20 (Figure 2), CD 79a and B-cell lymphoma (Bcl- 2) (Figure 3) with just a few CD3 positive lymphoid cells. However, no evidence of adenocarcinoma was found in the appendectomy specimen. After the diagnosis of lymphoma, a complete colonoscopy was planned and this revealed a solid tumoral mass in the caecum measuring 5x4x4 cm. Computed tomography of the abdomen and pelvis revealed mesenteric lymphadenopathy associated with a mass in the caecum with multiple nodules in liver consistent with metastasis (Figure 4). Frozen sections were not obtained since the treatment method would not be affected. The patient underwent anterior resection with regional lymphadenectomy, with the pathological assessment of the resected specimen revealing a collision tumor consisting of a poorly differentiated adenocarcinoma extending through the muscularis propria with MALT lymphoma (Figure 5). Microscopic evaluation of the 11 regional lymph nodes in the mesentery of the resected colon and liver biopsy showed diffuse infiltration of MALT lymphoma with metastasis of adenocarcinoma (Figure 6). According to immunohistochemistry, atypical lymphocytes were positive for CD 20, Bcl-2, and negative for CD3, CD5, CD10, CD23, Bcl-6, terminal deoxynucleotidyl transferase, and cyclin D1. The proliferation fraction (MIB-1 immunostaining) was approximately 20%. The morphological and immunohistochemical findings were used to confirm the diagnosis of synchronous presentation of MALT lymphoma and colon adenocarcinoma within the caecum, mesenteric lymph nodes and liver metastases.
Figure 1. Appendix lumen infiltrated with B lymphoid cells (h&e;x100)
Figure 2. CD 20 positivity of lymphoid cells (CD20, x200)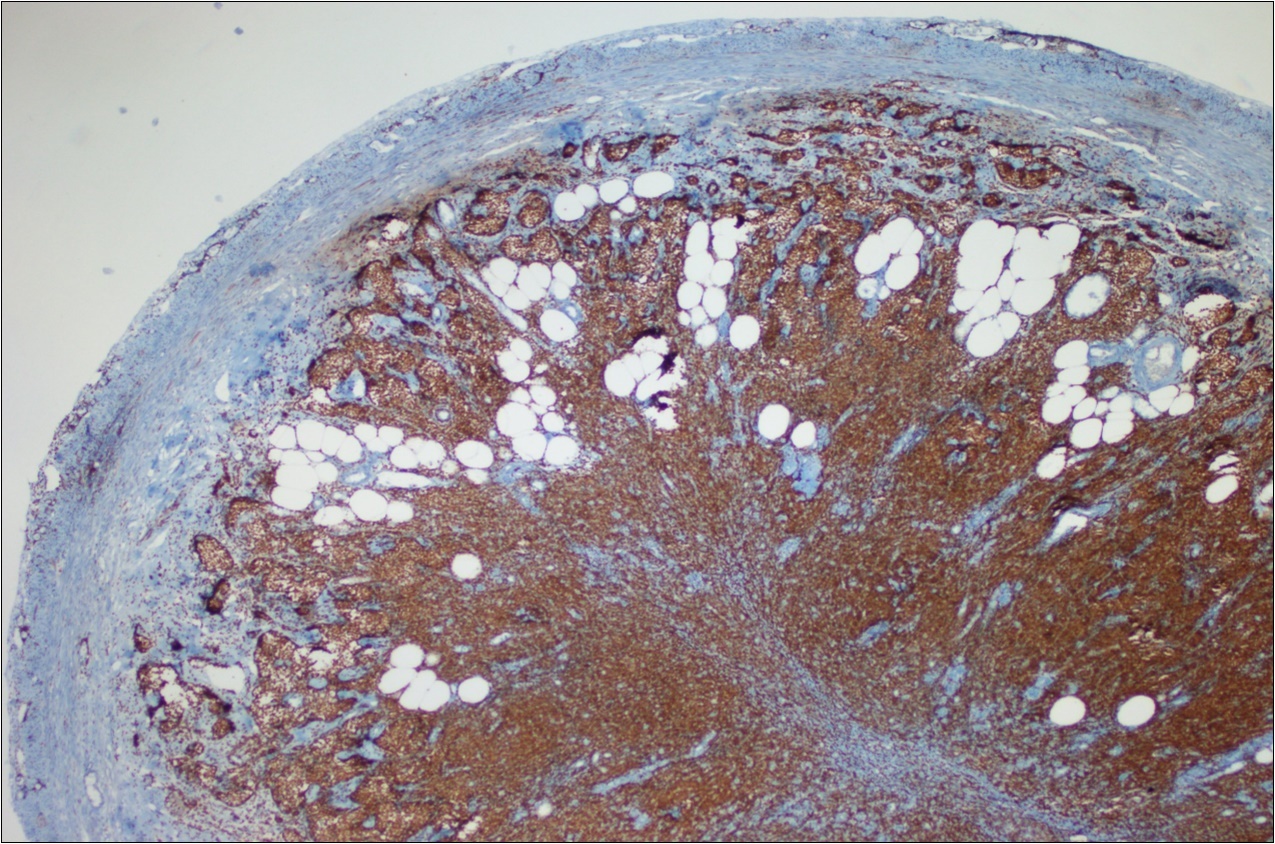
Figure 3. Bcl-2 positivity of lymphoid cells (Bcl-2, x200)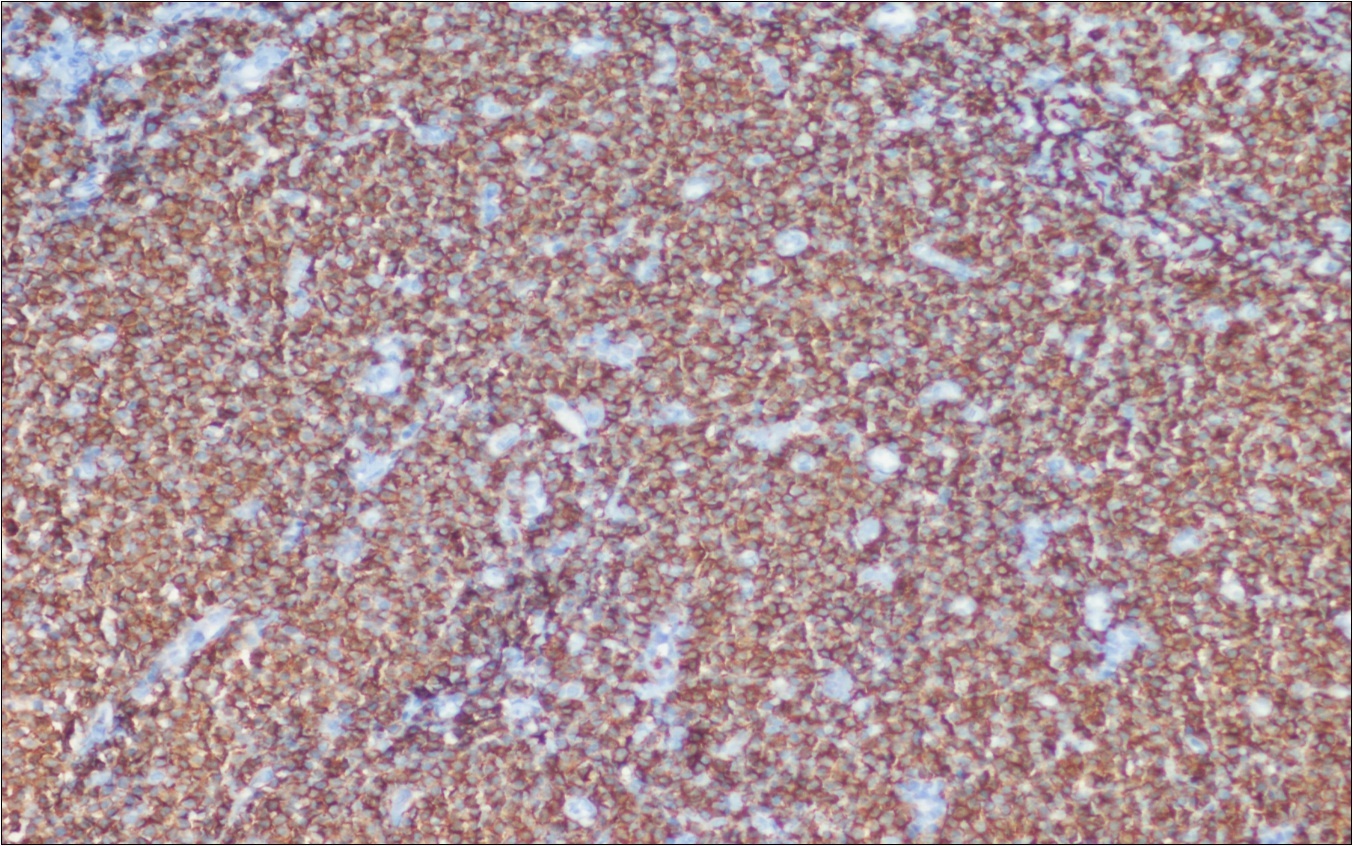
Figure 4. Adenocarcinoma with MALT lymphoma infiltration of liver (h&e;200)
Figure 5. Adenocarcinoma with MALT lymphoma infiltration of colon (h&e;200)
Figure 6. Adenocarcinoma with MALT lymphoma infiltration of lymph node (h&e;200)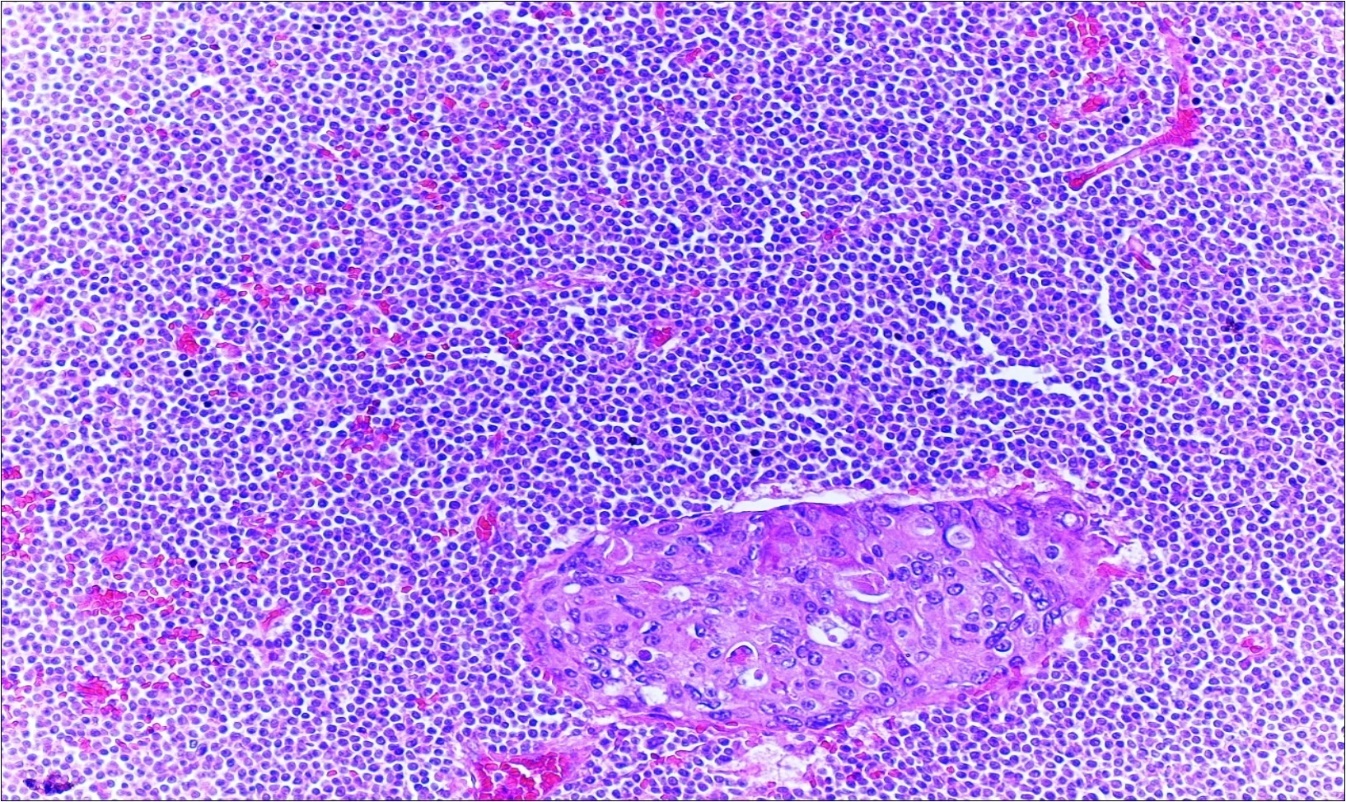
Discussion
Second malignancies are classified as synchronous or metachronous. According to Gluckman’s definition, “synchronous carcinomas” include carcinomas that present either simultaneously or within a six-month period of identification of the original tumor 1.
The gastrointestinal tract is the most frequently involved extranodal site in non-Hodgkin lymphoma, with stomach being the most common (50%-60%) followed by the small intestine (30%) 7.
Mucosa-associated lymphoid tissue MALT tumors are a distinct subtype of non-Hodgkin’s lymphoma associated with predisposing infectious or autoimmune processes, resulting in chronic lymphoid proliferation. Though the stomach is the most common site, MALT tumor has been reported in non-gastric sites like salivary gland, lung, eyes, adnexa, and skin. The colon is a rare location for MALT lymphoma 5.
Synchronous mantle cell lymphoma and adenocarcinoma (5 cases) were the most frequent diagnoses followed by synchronous extranodal marginal zone lymphoma of MALT and adenocarcinoma (3 cases). The involved sections of the colon included the caecum, ascending colon, sigmoid colon and rectum. Nearly all cases were preoperatively diagnosed as colonic adenocarcinoma. This indicates that it is a challenge to recognize synchronous colonic adenocarcinoma and malignant lymphoma preoperatively 7. The appropriate selection of immunohistochemical tests may help to establish the diagnosis. Immunohistochemical results can be resolved by molecular analysis, particularly when lymphomas are components of collision tumors of the colon.
Several case details of colonic synchronous mantle cell lymphoma and adenocarcinoma were reported in the literature, but to the best of our knowledge upon review of literature the present case is the first which was diagnosed firstly as lymphoma incidentally within the appendectomy specimen with synchronous adenocarcinoma and lymphoma in the colonic resection specimens. One of the features that distinguishes our case from the other cases was lymphoma infiltration of metastatic lymph nodes and the other was the presence of adenocarcinoma metastasis in liver parenchyma with lymphoma infiltration in the portal tracts.
There are some hypotheses suggesting the etiology of collision tumors. One hypothesis is that the two primary tumors arise in continuity through a chance accidental ‘meeting’. Another hypothesis is that the presence of the first tumor alters the microenvironment, precipitating the development of the second adjacent tumor 6.
Chance coincidence is favored. However, local factors such as absent immune surveillance in the lymphoma which possibly allow carcinoma cells to grow has also been suggested. The association between gastric MALT lymphoma and chronic H. pylori infection is well established. The mainstay of treatment for localized gastric MALT lymphoma is antibiotic therapy directed against H. pylori infection with complete remission reported in 70% to 80% of cases 11. Various infectious agents like H. pylori and hepatitis C virus have been implicated as a possible link in the development of non-gastric MALT 7. For colonic MALT lymphoma, there is no standardized therapy and the best treatment modality has long been debated. Most cases use surgery or chemotherapy as the first-line treatment, and rarely complete resolution with H. pylori therapy has been reported 11.
In conclusion, coexisting primary malignant lymphoma and colonic adenocarcinoma in one patient is a very rare event. Pathologists should be aware of the existence of synchronous tumors in the small and large intestines. Chance coincidence or poor immunity in patients may contribute to the etiology, but further research is required to determine the true underlying etiology of these cases.