
Despair Beyond Repair? Severity of Hopelessness in Depressed Psychiatric Inpatients
Abstract
Background:
Depression is related to suicidal ideation, attempts, and completion. However, depression fails to provide any specific identification for suicide risk. Hopelessness has been found to provide a more accurate estimate of suicide risk than seen in depression severity, and hopelessness can serve as a useful predictor of eventual death by suicide.
Aims:
The present study was designed to examine various levels of hopelessness and their association with other symptoms experienced by depressed psychiatric inpatients.
Method:
150 adult psychiatric inpatients were evaluated using a structured diagnostic interview and several standardized self-report questionnaires. All patients met criteria for a depressive diagnosis at the time of the evaluation. Patients were classified into four discrete categories of hopelessness using the Beck Hopelessness Scale.
Results:
No differences were observed when the four groups of depressed psychiatric inpatients were compared on demographic variables and background clinical events. However, several key differences were observed between groups on measures of depression severity, suicidal ideation, and tendencies to cope by distraction.
Conclusions:
It appears useful to evaluate suicide risk as it changes across different levels of hopelessness. Depressed patients with higher levels of hopelessness report more severe problems on several dimensions related to suicide risk.
Article Information
- Received
- Accepted
- Published
Academic Editor: Rebecca Robillard, Chronobiology and Sleep Group, Brain and Mind research Institute, the University of Sydney
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 James C. Overholser, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: James C. Overholser, Ph.D., ABPP, Department of Psychology, Ca, se Western Reserve University, 10900 Euclid Avenue, Cleveland, Ohio, 44106-7123 —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
An important component of severe depression is hopelessness, the expectation that current life problems will never be resolved.1 Hopelessness is associated with the current diagnosis and future risk of developing depression.2 In a survey of a random sample of 1,722 community adults in Finland, Haatainen and colleagues 3 found that hopelessness was fairly common in the general public (31% mild hopelessness, 8% moderate, and 2% severe hopelessness). In addition, hopelessness serves as a central risk factor for suicide among depressed patients.4
When patients become overwhelmed with feelings of hopelessness, they may give up their coping efforts as their goal-directed behavior begins to shut down.5 Depressed patients may exacerbate their negative moods through tendencies for rumination and passive brooding.6 These qualities could become highly disruptive for treatment. Higher levels of hopelessness may make patients less responsive to psychological treatments.7 Furthermore, in a study examining the pharmacological treatment of major depression, Papakostas and colleagues8 found that hopelessness predicted a poor response to drug treatment and created a risk for more severe depression when treatment was completed.
Higher levels of hopelessness are found in individuals who display suicide ideation,3, 9 suicide attempts,10, 11 and death by suicide.12, 13, 14 In addition, the persistence of suicidal ideation is significantly related to the degree of hopeless expectations 15. Hopelessness was elevated in high-risk patients who continued to display suicidal ideation one-month after their hospital admission.16 Furthermore, higher levels of hopelessness have been found in patients who attempted suicide using a premeditated strategy,17 and the added time spent dwelling on suicide plans was found to result in a higher degree of medical lethality in the suicide attempt 18
In a classic study, Beck, Steer, Kovacs, and Garrison19 examined 207 psychiatric inpatients who had been hospitalized for suicidal ideation. Over the next 5-10 years, 14 of these patients died by suicide. Results showed that elevated scores on the Beck Hopelessness Scale identified 91% of the completers. Subsequently, in a large scale clinical follow-up evaluation of 1,958 psychiatric outpatients, Beck and colleagues20 found that higher levels of hopelessness predicted eventual death by suicide. A cut-off of 9 or higher on the BHS identified 94% of the small sample of patients (n=17) who died by suicide. However, another study21 found that BHS scores were typically elevated (i.e., 9 or higher) even for those suicide attempters who did not go on to die by suicide during the four-year follow-up period. A cut-score of 9 results in a high rate of false positive classifications.21 Thus, it remains unclear as to the potential utility of the dichotomous split. The simple classification is helpful for most clinicians, but it may lack the accuracy and detail needed to identify patients at risk.
Prior research has not adequately examined the potential impact of different severity levels of hopelessness. Most studies22 have compared high hopelessness to low hopelessness groups, while neglecting the potential impact of intermediate levels of hopelessness. Problems arise when using the standard dichotomous cut-off scores, increasing the potential of false negative prediction errors23 as well as false positive prediction errors.24 When hopelessness scores are dichotomized into high versus low groups using the 9-point cut-off, hopelessness is not always effective in differentiating patients at risk for eventual death by suicidal versus non suicidal deaths.24 The situation becomes even more complicated because the scoring guidelines for the BHS25 encourage investigators to adjust the recommended cut-off score depending on the sample and purpose of the assessment, raising the cut score in order to reduce the risk of either false positive cases, or lowering the cut score in order to reduce the risk of false negative prediction errors. Thus, grouping strategies may benefit from more subtle gradations across the different levels of hopelessness severity.
The present study was designed to examine the clinical utility of hopelessness by categorizing depressed patients into distinct levels of hopeless attitudes. It was expected that higher levels of hopelessness would be associated with more severe depression and a greater number of stressful life events than seen in patients with low levels of hopelessness. In addition, it was expected that intermediate levels of hopelessness would be related to moderate levels of emotional distress (i.e., depression severity and suicidal thoughts).
Method
Subjects:
At the time of participation in the study, all patients were currently hospitalized at a private psychiatric hospital where the average inpatient stay lasts 6-10 days per admission. A total of 150 adult psychiatric inpatients were assessed during their short-term hospital stay. Patients ranged in age from 18 – 73 (M = 36.22, SD = 10.13). To be eligible for participation in the study, the patients had to report symptoms of depression, and patients were excluded if they displayed evidence of psychosis, organic brain damage, intellectual disability, or bipolar disorder. At the time of their participation in the study, all patients met criteria for a depressive disorder, including Major Depressive Disorder – single episode (n=27), Major Depressive Disorder – recurrent episode (n=107), Dysthymia (n=13), or Adjustment Disorder with Depressed Mood (n=3). These diagnoses were based on DSM-IV criteria,26 and the diagnoses were verified through the use of the Structured Clinical Interview for DSM-IV Disorders (SCID).27 In addition, 41% of patients met criteria for a secondary Axis I syndrome, with the most common co-morbid disorders including Alcohol Abuse (n=10), Alcohol Dependence (n=13), PTSD (n=7), and Panic Disorder (n=4).
Measures:
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID)27 is a thorough diagnostic interview designed to evaluate the presence of Axis I major mental disorders according to the diagnostic criteria established by the American Psychiatric Association.26 Graduate student research assistants were trained in DSM-IV psychiatric diagnosis, clinical interviewing skills, and the SCID structured diagnostic interviewing procedures using advanced coursework, videotapes, and direct observational methods. Trained interviewers met with each patient individually and spent 40-60 minutes discussing the patient’s current and lifetime presence of psychiatric symptoms. Only patients who met criteria for a depressive diagnosis were included in the study.
Beck Hopelessness Scale (BHS)28 includes 20 true-false statements designed to assess the severity of pessimistic views about the future. The BHS has shown evidence of reliability and predictive validity.19, 29 According to the BHS scoring manual,26 BHS scores can be categorized into four levels of severity: minimal (0-3), mild (4-8), moderate (9-14), and severe (15-20). However, prior studies have not examined the utility of these classifications, and other studies3 have used slightly different cut-off scores. In the present study, the standard 4-level cut-off scores were used to classify patients into minimal, mild, moderate, and severe levels of hopelessness.
Beck Depression Inventory (BDI)30 includes 21 items designed to evaluate the severity of different depressive symptoms. Scores can range from 0 – 63, with higher scores reflecting more severe depression. BDI scores range from minimal depression (0-9), mild (10-15), moderate (16-29) and severe depression (30-63). The BDI has consistently demonstrated evidence of reliability and validity in a wide variety of settings. Prior studies have demonstrated high internal consistency but low temporal stability31which makes sense given the transitory nature of emotional reactions.
Beck Scale for Suicidal Ideation (BSSI)32 includes 19 items designed to quantify the presence and severity of suicidal thoughts. Items examine key issues in suicide risk, such as a suicide plan and reasons for living. The BSSI has demonstrated evidence of reliability and validity in clinical samples.33 Prior research on the BSSI34 has demonstrated a high degree of internal consistency (α = .95) and a moderate level of test-retest reliability (r = .54). In addition, the BSSI has shown evidence of concurrent validity through its correlations with other measures of suicidal thoughts.35
Daily Emotion Report (DER)36 includes 32 statements designed to measure tendencies for coping with dysphoric feelings. The DER items explore the patient’s actual responses to negative emotions as opposed to hypothetical situations.37 Items are rated from 1 (almost never) to 4 (almost always) in terms of their frequency of use with higher scores reflecting a stronger tendency to rely on the coping strategy. Cluster analyses have divided the scale into two significant item groupings that were used to create subscales measuring rumination and distraction.36 The DER Rumination scale examines the destructive tendency to withdraw from social activity and focus on the painful emotions. Higher scores on the DER Rumination scale reflect a stronger reliance on ruminative thoughts when confronted with assorted problems. The DER Distraction scale examines the potentially useful strategy of keeping busy with assorted activities in an attempt to focus away from the negative emotions. Higher scores on the DER Distraction scale reflect the use of self-distraction when upset and tendencies to cope with stress by avoiding thoughts about the problems.
Procedures:
Informed consent was obtained prior to any data collection. After completing the SCID interview, all patients were asked to complete the packet of self-report questionnaires in the same order. All patients completed a clinical data form that gathered information about demographic factors, the current presence of suicidal ideation, recent and lifetime suicidal attempts, substance abuse, physical and sexual abuse, and any family history of mental illness. Patients were classified into four groups based on their scores from the Beck Hopelessness Scale, using the standard cut-off scores.25
Data Analysis Plan:
When comparing the four groups, analyses used chi-square comparisons for categorical variables, and oneway ANOVAs were used for continuous measures. When the oneway ANOVA was found significant, Tukey post hoc comparisons were used to identify the specific group differences. The Tukey test was used with alpha set at p < .05 The Tukey statistical test identifies group Mean scores that are significantly different from other Means, but does not report a composite statistical score. All analyses were calculated using the SPSS statistical program.
Results
Self-report measures were examined for their distribution of scores. Across all patients in the present study, BDI scores ranged from 1 - 59, with a Mean of 28.93 (SD = 12.01). BSSI scores ranged from 0 - 41, with a Mean of 11.52 (SD = 11.01). DER Rumination scores ranged from 30 - 62, and a Mean of 46.31 (SD = 7.68). DER Distraction scores ranged from 20 - 58, and a Mean of 36.01 (SD = 7.49). BHS scores ranged from 0 to 20, with a Mean of 10.83 (SD = 6.25). Using the cut-off scores for minimal (0-3), mild (4-8), moderate (9-14), or severe (15-20) levels of hopelessness, 28 (18.66%) patients were found to report minimal hopelessness, 26 (17.33%) patients reported mild hopelessness, 41 (27.33%) patients reported moderate hopelessness, and 55 (36.66%) patients reported severe hopelessness.
The four groups of depressed patients did not display any significant differences on the assorted demographic variables (see Table 1). Thus, the four groups were similar in terms of age, race, gender, marital status, and educational level. No significant differences across groups were found in terms of several key family factors, including mental illness in the patient’s mother or the patient’s father. Also, no significant differences across groups were seen in the lifetime presence of previous suicide attempts by the patient’s mother or by the patient’s father. In addition to the background information summarized in Table 1, no significant differences across groups were seen in the lifetime presence of substance abuse by the patient’s mother (Ҳ2 (3) = 0.86, ns) or by the patient’s father (Ҳ2 (3) = 0.69, ns). Finally, no significant differences across groups were seen in the likelihood of depression in the patient’s mother (Ҳ2 (3) = 3.46, ns) or the patient’s father (Ҳ2 (3) = 3.76, ns).
Table 1. Demographic Comparison of Four Groups of Depressed Psychiatric Inpatients Based on Levels of Hopelessness (N = 150)| Variables | MinimalHopelessness | MildHopelessness | ModerateHopelessness | SevereHopelessness | Statistic |
| N | 28 | 26 | 41 | 55 | |
| Age M | 36.11 | 34.77 | 35.31 | 37.65 | F (3,147) = 0.65, ns |
| (SD) | (12.79) | (9.11) | (11.22) | (8.07) | |
| Race (% Caucasian) | 96.4 | 92.3 | 90.5 | 90.9 | Ҳ2 (3) = 0.97, ns |
| Gender (% female) | 64.3 | 37.5 | 47.2 | 51.0 | Ҳ2 (3) = 0.29, ns |
| Educational background | Ҳ2 (3) = 2.36, ns | ||||
| % high school diploma | 60.0 | 37.5 | 47.2 | 51.0 | |
| % college degree | 40.0 | 62.5 | 52.8 | 49.0 | |
| Marital status | Ҳ2 (3) = 3.22, ns | ||||
| % married, cohabitating | 64.3 | 53.8 | 42.9 | 54.5 | |
| % single, divorced, widowed | 35.7 | 46.2 | 57.1 | 45.5 | |
| Maternal mental illness (% present) | 12.0 | 8.3 | 25.6 | 10.0 | Ҳ2 (3) = 5.50, ns |
| Mother attempted suicide (% yes) | 8.0 | 13.0 | 12.8 | 9.6 | Ҳ2 (3) = 0.56, ns |
| Paternal mental illness (% present) | 9.5 | 9.5 | 23.1 | 14.9 | Ҳ2 (3) = 2.82, ns |
| Father attempted suicide (% yes) | 14.3 | 4.8 | 5.4 | 6.4 | Ҳ2 (3) = 1.98, ns |
| Variable | MinimalHopelessness | MildHopelessness | ModerateHopelessness | SevereHopelessness | Statistic |
| Axis I Major Depressive Disorder (% present) | 82.1 | 92.3 | 90.2 | 90.9 | Ҳ2 (3) = 1.94, ns |
| Axis I comorbidity (% present) | 32.1 | 50.0 | 32.5 | 42.3 | Ҳ2 (3) = 2.72, ns |
| History of drug abuse (% present) | 33.3 | 50.0 | 35.7 | 47.3 | Ҳ2 (3) = 2.82, ns |
| Recent drug abuse (% present) | 42.9 | 26.9 | 23.8 | 16.4 | Ҳ2 (3) = 7.00, ns |
| History of physical abuse (% present) | 39.3 | 50.0 | 52.4 | 47.3 | Ҳ2 (3) = 1.22, ns |
| History of sexual abuse (% present) | 33.3 | 38.5 | 50.0 | 41.8 | Ҳ2 (3) = 2.07, ns |
| BDI Depression severity M | 17.78a | 21.12a | 30.67b | 37.87c | F (3,146) = 32.35, p < .0001 |
| (SD) | (10.77) | (8.94) | (8.52) | (12.56) | |
| DER Rumination M | 42.29 | 43.80 | 47.69 | 48.03 | F (3,146) = 2.94, p < .05 |
| (SD) | (9.43) | (7.91) | (6.53) | (7.08) | |
| DER Distraction M | 41.50a | 39.29a | 36.19a,b | 32.11b | F (3,146) = 8.97, p < .001 |
| (SD) | (6.96) | (8.53) | (5.48) | (6.78) | |
| BSSI Suicidal ideation severity M | 4.54a | 4.96a,b | 10.34b | 19.02c | F (3,146) 22.26, p < .0001 |
| (SD) | (8.38) | (6.90) | (8.53) | (10.79) | |
| Suicidal ideation (% present) | 74.1 | 73.1 | 87.8 | 94.5 | Ҳ2 (3) = 9.73, p < .02 |
| Recent suicide attempt (% present) | 32.1 | 42.3 | 23.8 | 43.6 | Ҳ2 (3) = 4.74, ns |
| Lifetime suicide attempt (% present) | 46.4 | 65.4 | 61.9 | 72.7 | Ҳ2 (3) = 5.63, ns |
The four groups of depressed patients were compared on a variety of psychiatric disorders and clinical problems (see Table 2). Across the entire sample, the majority of patients (89.3%) met criteria for a Major Depressive Disorder at the time of their hospital stay. In addition, several patients (8.7%) met criteria for Dysthymic Disorder, and a few patients (2.0%) met criteria for an Adjustment Disorder with Depressed Mood. No significant differences were observed across groups in their primary psychiatric diagnosis at the time of admission to the hospital. Across the entire sample, 67 (44.6%) of the patients met criteria for an additional Axis I disorder. However, no significant differences across the four patient groups were seen in the rate of comorbid secondary Axis I psychiatric disorders.
When examining information from the patient’s background questionnaires, the four groups of depressed patients did not display significant differences in terms of recent substance abuse, or lifetime substance abuse. Also, despite a high prevalence of abuse in the current sample, no significant differences across groups were observed in the likelihood of reporting a personal history of being physical abused or sexually abused.
Significant differences across groups were found on depression severity as measured by BDI scores (F (3,146) = 32.35, p < .0001). In order to identify the specific group differences, Tukey post hoc comparisons on BDI Mean scores revealed significant differences (p < .05) across the groups. Patients in the severe hopelessness group endorsed significantly more elevated scores on the BDI than patients than any of the other three groups. Furthermore, patients in the moderate hopelessness group reported significantly higher BDI scores than patients in either the minimal hopelessness or mild hopelessness groups (see Figure 1).
Figure 1. Differences in severity of (as measured by BDI) across four groups of depressed psychiatric inpatients.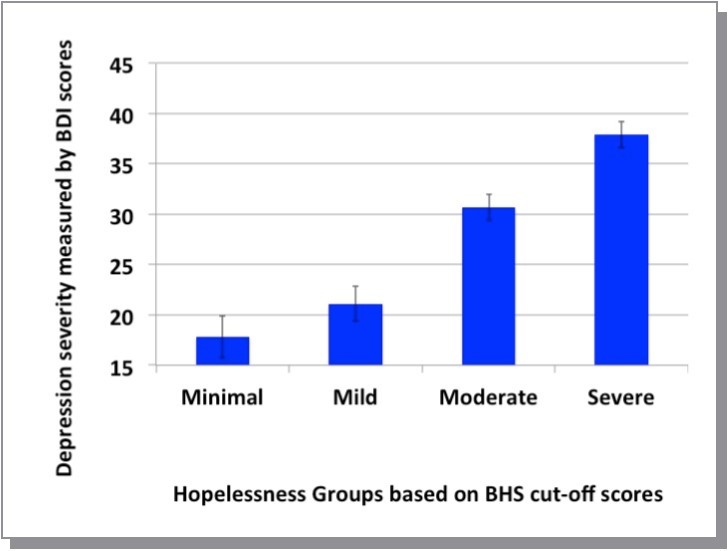
Download figure
Significant differences across groups were observed on the DER Rumination scale (F (3,146) = 2.94, p < .05). However, because the magnitude of this effect was rather small, Tukey post hoc comparisons failed to identify any significant differences between the specific groups on the DER Rumination scale. Significant differences across groups were observed on the DER Distraction scale (F (3,146) = 8.97, p < .001). Tukey post hoc comparisons revealed significant differences (p < .05) across specific groups. Patients with severe levels of hopelessness reported significantly lower scores on DER Distraction as compared to patients in either the minimal hopelessness or the mild hopelessness groups.
When examining the presence or absence of suicidal ideation during their hospital stay, significant differences across groups were found for the current presence of suicidal ideation (Ҳ (3) = 9.73, p < .02), with severe hopelessness patients being most likely to report suicidal ideation at the time of evaluation. Furthermore, at the time of their admission to the hospital, patients in the moderate hopelessness group displayed more frequent suicidal ideation than seen in either the minimal hopelessness or the mild hopelessness groups.
When examining the severity of suicidal ideation as measured by the BSSI, significant differences were observed across groups (F = (3,146) 22.26, p < .0001). Tukey post hoc tests revealed significant differences (p < .05) on BSSI Mean scores between the groups. Patients with severe hopelessness reported significantly more intense suicidal ideation than patients in any of the other three groups. Furthermore, patients with moderate levels of hopelessness reported significantly more intense suicidal ideation than patients with minimal hopelessness (see Figure 2).
Figure 2. Differences in severity of suicidal ideation (as measured by BSSI) across four groups of depressed psychiatric inpatients.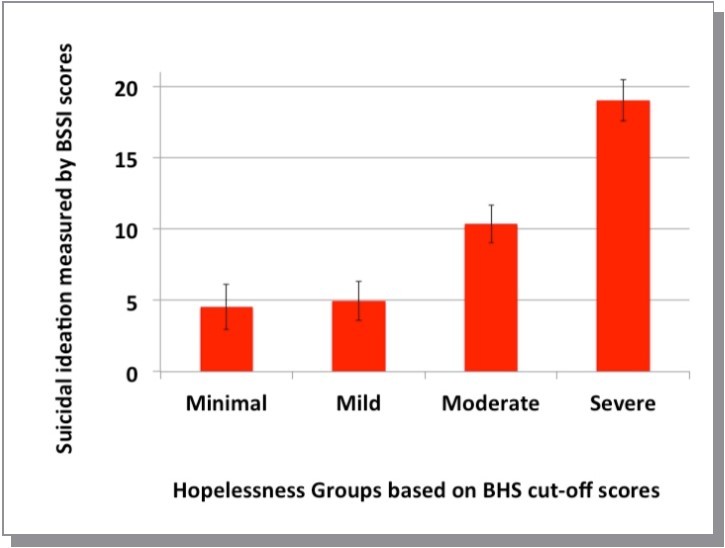
Download figure
When examining actual suicidal behaviors, the four groups of patients did not differ in the rate of recent suicide attempts (Ҳ2 (3) = 4.74, ns) or the rate of lifetime suicide attempts (Ҳ2 (3) = 5.63, ns).
Post Hoc Analyses
Because the earlier analyses revealed important relationships between depression, hopelessness, and suicidal ideation, it was important to examine the differential impact of hopelessness on suicidal ideation after controlling for depression severity. A hierarchical regression analysis was used to examine the unique contribution of hopelessness when assessing suicidal ideation (as measured by the BSSI), after controlling for depression severity (as measured by the BDI). At the first step, the hierarchical multiple regression analysis examined the relationship between BDI depression scores and BSSI Suicidal Ideation scores. Results showed that suicidal ideation was significantly associated with the severity of depression (R2 = .320, F (1, 147) = 69.09, p < .0001). At the second step of the hierarchical regression, the four hopelessness groups (classified as minimal, mild, moderate, or severe levels of hopelessness) were added to the predictive model. Despite the inter-correlation between hopelessness and depression, results showed that the BHS Hopelessness groups added a small but significant amount of variance to the explanation of BSSI suicidal ideation (ΔR2 = .049, F (1, 146) = 11.41, p < .001)
Discussion
Hopelessness plays a critical role in the pathway from depression to suicide risk. In the current study, as compared to patients with minimal hopelessness, depressed patients with moderate or severe hopelessness reported more severe depression, more frequent suicidal thoughts, more intense suicidal ideation, and tendencies for ineffective coping strategies (such as rumination) when struggling with difficult life problems. Preliminary evidence suggests that suicidal ideation is aligned with moderate and severe levels of hopelessness even when controlling for the severity of depression. Negative expectations for the future may provide insights into the mind of the suicidal individual, providing a more direct link to suicide risk than obtained through the presence or severity of depression.14 Negative expectations about the future can aggravate a dysphoric mood and push the patient toward a suicidal crisis.
Despite the strong association between depression and suicide, the direct link between depression severity and suicide risk is greatly reduced when hopelessness is included in the predictive model.14 The present results support the small but important addition that is made to the prediction of suicide risk when using hopelessness groups in addition to depression severity. Thus, hopelessness remains a useful risk factor for suicide.4 However, it is important to retain a broad view of suicide risk, conceptualizing a suicidal crisis as a process that develops over time.16 Thus, depression and hopelessness may set the stage for a suicidal crisis. Depending on the presence and severity of other proximal and distal risk factors, the crisis can extend from suicidal ideation, to suicide attempts, and death by suicide.38 It is often important to include stressful life events into a comprehensive view in order to appreciate the situational factors that often serve to trigger the acute distress underlying a suicidal crisis.39 Hopelessness may serve as an important predisposing factor that becomes aggravated during periods of high stress.40 When problems arise, severe levels of hopelessness may promote feelings of despair and a tendency to give up, thereby blocking effective coping and potentially interfering with successful treatment.
The efficient assessment of hopelessness is central to the clinical management of an acute suicidal crisis, and hopelessness can be monitored throughout the course of outpatient follow-up treatment after a suicide attempt.41 Because of the close relationship between hopelessness and suicidal tendencies in depressed patients, it is important to assess and monitor pessimistic views over time. Clinicians may need to actively assess levels of hopelessness throughout the duration of treatment to ensure that patients do not cross the threshold from mild to moderate levels of hopelessness. Clinicians are advised to remain actively supportive whenever working with clients who report moderate or severe levels of hopelessness. Ideally, intervention strategies can be used to identify, explore, and reduce tendencies for hopelessness in depressed patients.
The present findings are limited because of their reliance on patient self-report. However, previous research has shown that across the available self-report measures, the BHS provides the best estimate of pessimistic expectations.29 Nonetheless, the BHS has been hindered by its low specificity.29, 23 Furthermore, a simple cut-off using 9 or above on the BHS is not always effective in identifying depressed patients who later die by suicide.24 Instead, it seems likely that the use of four levels of hopelessness may facilitate a more sophisticated interpretation of hopelessness severity ratings.
From a statistical view, cut-off scores can be more limiting than continuous dimensional ratings.42 However, the present study was designed to examine the clinical utility of hopelessness subgroups because clinicians often rely on categorical levels to interpret scale scores. The simple 4-level classification scheme is compatible with standard clinical practice. BHS scores can be easily classified as minimal, mild, moderate or severe levels of hopelessness. The present results identified few differences between groups who reported minimal versus mild levels of hopelessness. However, patients who reported moderate or severe levels of hopelessness also reported a range of clinical problems and suicide risk factors. Patients with moderate levels of hopelessness displayed important differences from the other groups in terms of depression severity, suicidal ideation, and maladaptive coping. Thus, it seems useful to identify patients who report moderate or severe levels of hopelessness.
The present study included standardized measures that were collected on a clinical sample, and all psychiatric diagnoses were verified through the use of structured diagnostic interviews. However, several patients met criteria for a comorbid Axis I psychiatric diagnosis. It is possible that other psychiatric conditions could have added unwanted variability into the assessment of depression and suicide risk. Some prior studies have found a relationship between suicide risk and PTSD43 as well as panic disorder.44 Thus, the present findings should be interpreted with caution.
The present study examined information that was collected directly from a group of depressed psychiatric inpatients. Future studies may be able to examine whether the present findings generalize to outpatient psychiatry clinics, general medical centers, and community controls. More streamlined versions of the Hopelessness Scale could facilitate the efficient monitoring of pessimistic expectations in a variety of settings,45 such as primary care clinics or school-based settings. The BHS is best viewed as a brief screening measure that can be followed by more thorough interview measures when hopelessness exceeds minimal or mild levels.
The present results showed the important influence of hopelessness on the presence and severity of suicidal ideation in depressed psychiatric inpatients. However, BHS hopelessness groups were not significantly related to actual suicide attempts, perhaps because of the low base rate of suicidal actions. Thankfully, suicide is an infrequent event, even among psychiatric patients. Furthermore, suicide is a complex problem that is influenced by a variety of factors, and it remains difficult to predict actual cases of suicidal behavior.40
Researchers and clinicians should go beyond a focus on the reduction of depressive symptoms and strive to improve strategies for monitoring and reducing hopeless attitudes. A decline in hopelessness precedes, and potentially helps to produce significant reductions in suicidal thoughts.46 Because higher levels of hopelessness have been associated with maladaptive coping responses, therapy may strive to disrupt this destructive cycle and improve clients’ ability to manage their difficult times. The cultivation of client strengths may help to reduce feelings of hopelessness.47
Contribution of Authors:
1.James Overholser, helped with data collection, analysis, interpretation, writing
2.Lauren Fisher, helped with data collection, analysis, interpretation, writing
3.Abby Braden, helped with data collection, analysis, interpretation, writing
4.Nicole Peak, helped with data collection, analysis, interpretation, writing
References
- 1.A T Beck, Wenzel A, Riskind J, Brown G, Steer R. (2006) Specificity of hopelessness about resolving life problems. , Cognitive Therapy and Research 30, 773-781.
- 2.Alloy L, Clements C. (1998) Hopelessness theory of depression. , Cognitive Therapy and Research 22, 303-335.
- 3.Haatainen K, Tanskanen A, Kylma J, Honkalampi K, Koivumaa-Honkanen H et al. (2004) Factors associated with hopelessness. , International Journal of Social Psychiatry 50, 142-152.
- 4.Hawton K, Comabella C, Haw C, Saunders K. (2013) Risk factors for suicide in individuals with depression. , Journal of Affective Disorders 147, 17-28.
- 5.Haeffel G, Abramson L, Paige B, Shah J. (2008) Hopelessness theory and the approach system. , Cognitive Therapy and Research 32, 281-290.
- 6.Treynor W, Gonzalez R, Nolen-Hoeksema S. (2003) Rumination reconsidered: A psychometric analysis. , Cognitive Therapy and Research 27, 247-259.
- 7.Birmaher B, Brent D, Kolko D, Baugher M, Bridge J et al. (2000) Clinical outcome after short-term psychotherapy for adolescents with Major Depressive Disorder. , Archives of General Psychiatry 57, 29-36.
- 8.Papakostas G, Petersen T, Homberger C, Green C, Smith J et al. (2007) Hopelessness as a predictor of non-response to fluxetine in Major Depressive Disorder. , Annals of Clinical Psychiatry 19, 5-8.
- 9.Keilp J, Grunebaum M, Gorlyn M, LeBlanc S, Burke A et al. (2012) Suicidal ideation and the subjective aspects of depression. , Journal of Affective Disorders 140, 75-81.
- 10.Holmo K, Melartin T, Haukka J, Holma I, Sokero T et al. (2010) Incidence and predictors of suicide attempts in DSM-IV Major Depressive Disorder. , American Journal of Psychiatry 167(7), 801-808.
- 11.Jager-Hyman S, Cunningham A, Wenzel A, Mattei S, Brown G et al. (2014) Cognitive distortions and suicide attempts. , Cognitive Therapy and Research 38, 369-374.
- 12.Kuo W-H, Gallo J, Eatoin W. (2004) Hopelessness, depression, substance disorder, and suicidality. , Social Psychiatry & Psychiatric Epidemiology 39(6), 497-501.
- 13.Sinclair J, Harriss L, Baldwin D, King E. (2005) Suicide in depressive disorders. , Journal of Affective Disorders 87, 107-113.
- 14.Zhang J, Li Z. (2013) The association between depression and suicide when hopelessness is controlled for. , Comprehensive Psychiatry 54, 790-796.
- 15.Zhang Y, Law C, Yip P. (2011) Psychological factors associated with the incidence and persistence of suicidal ideation. , Journal of Affective Disorders 133, 584-590.
- 16.Links P, Nisenbaum R, Ambreen M, Balderson K, Bergmans Y et al. (2012) Prospective study of risk factors for increased suicide ideation and behavior following recent discharge. , General Hospital Psychiatry 34, 88-97.
- 17.Spokas M, Wenzel A, Brown G, A T Beck. (2012) Characteristics of individuals who make impulsive suicide attempts. , Journal of Affective Disorders 136, 1121-1125.
- 18.Baca-Garcia E, Diaz-Sastre C, Basurte E, Prieto R, Ceverino A et al. (2001) A prospective study of the paradoxical relationship between impulsivity and lethality of suicide attempts. , Journal of Clinical Psychiatry 62(7), 560-567.
- 19.A T Beck, Steer R, Kovacs M, Garrison C. (1985) Hopelessness and eventual suicide: A ten-year prospective study of patients hospitalized with suicidal ideation. , American Journal of Psychiatry 142(5), 559-563.
- 20.A T Beck, Brown G, Berchick R, Stewart B, Steer R. (1990) Relationship between hopelessness and ultimate suicide. , American Journal of Psychiatry 147(2), 190-195.
- 21.Nimeus A, Traskman-Bendz L, Alsen M. (1997) Hopelessness and suicidal behavior. , Journal of Affective Disorders 42, 137-144.
- 22.Whisman M, Miller I, Norman W, Keitner G. (1995) Hopelessness depression in depressed inpatients. , Cognitive Therapy and Research 19, 377-398.
- 23.McMillan D, Gilbody S, Bereford E, Neilly L. (2007) Can we predict suicide and non-fatal self-harm with the Beck Hopelessness Scale?. , Psychological Medicine 37, 769-778.
- 24.Wenzel A, Berchick E, Tenhave T, Halberstadt S, Brown G et al. (2011) Predictors of suicide relative to other deaths in patients with suicide attempts and suicide ideation. , Journal of Affective Disorders 132, 375-382.
- 26.American Psychiatric Association. (2000) Diagnostic and statistical manual of mental disorders (4th Ed, Text rev.).Washington,DC:Author.
- 27.First M, Spitzer R, Gibbon M, Williams J. (1995) Structured Clinical Interview for DSM-IV Axis I Disorders (SCID, Version 2).New York State Psychiatric Institute: Biometrics Research Department.
- 28.Beck A, Weissman A, Lester D, Trexler L. (1974) The measurement of pessimism. The Hopelessness Scale. , Journal of Consulting and Clinical Psychology 42, 861-865.
- 29.Glanz L, Haas G, Sweeney J. (1995) Assessment of hopelessness in suicidal patients. , Clinical Psychology Review 15, 49-64.
- 30.A T Beck, C H Ward, Mendelson M, Mock J, Erbaugh J. (1961) An inventory for measuring depression. , Archives of General Psychiatry 4, 561-571.
- 31.Dori G, J C Overholser. (2000) Evaluating depression severity and remission with a modified Beck Depression Inventory. , Personality & Individual Differences 28, 1045-1061.
- 32.A T Beck, Kovacs M, Weissman A. (1979) Assessment of suicidal intention: The Scale for Suicide Ideation. , Journal of Consulting and Clinical Psychology 47, 343-352.
- 33.A T Beck, R A Steer, W F Ranieri. (1988) Scale for suicide ideation: Psychometric properties of a self-report version. , Journal of Clinical Psychology 44, 499-505.
- 34.A T Beck, Steer R. (1991) Manual for the Beck Scale for Suicidal Ideation. San Antonio,TX:Psychological Corporation.
- 35.A T Beck, Brown G, Steer R. (1997) Psychometric characteristics of the Scale for Suicide Ideation with psychiatric outpatients. , Behavior Research and Therapy 35(11), 1039-1046.
- 36.Nolen-Hoeksema S, Morrow J, Fredrickson B. (1993) Response styles and the duration of episodes of depressed mood. , Journal of Abnormal Psychology 102, 20-28.
- 37.Peak N, J C Overholser, DeJong T, Zaccariello M. (2007) A psychometric investigation of the Daily Emotion Report in a sample of depressed inpatients. , Journal of Clinical Psychology 63(9), 835-841.
- 39.J C Overholser, Braden A, Dieter L. (2012) Understanding suicide risk: Identification of high-risk groups during high-risk times. , Journal of Clinical Psychology 68(3), 334-348.
- 41.J C Overholser. (1995) Treatment of suicidal patients: A risk-benefit analysis. Behavioral Sciences and the Law 11, 81-92.
- 42.Cochrane-Brink K, Lofchy I, Sakinofsky I. (2000) Clinical rating scales in suicide risk assessment. , General Hospital Psychiatry 22, 445-451.
- 43.Conner K, Bossarte R, He H, Jyoti H, Arora J et al. (2014) Posttraumatic stress disorder and suicide in 5.9 million individuals receiving care in the veterans health administration health system. , Journal of Affective Disorders 166, 1-5.
- 44.Katz C, Yaseen Z, Mojtabai R, Cohen L, Galynker I. (2011) Panic as an independent risk factor for suicide attempt in depressive illness. , Journal of Clinical Psychiatry 72(12), 1628-1635.
- 45.Fisher L, J C Overholser. (2013) Refining the assessment of hopelessness: An improved way to look to the future. , Death Studies 37(3), 212-227.
Cited by (9)
This article has been cited by 9 scholarly works according to:
Citing Articles:
Neuropsychiatric Disease and Treatment (2025) Crossref Semantic Scholar OpenAlex
Comprehensive Psychiatry (2023) Crossref OpenAlex
M. Pompili, Bernardo Dell'osso, G. Rosso, M. Amore, Antonello Bellomo et al. - Comprehensive Psychiatry (2023) Semantic Scholar
Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring (2022) Crossref Semantic Scholar OpenAlex
Lung Cancer (2020) Crossref OpenAlex
B. Andersen, T. Valentine, Stephen B Lo, D. Carbone, C. Presley et al. - Lung Cancer (2019) Semantic Scholar
J. Lehmann, X. Jiménez - (2018) Semantic Scholar OpenAlex