Progress in Rehabilitation Treatments for Sepsis Patients in ICU
Abstract
Early active mobilisation and rehabilitation in the intensive care unit (ICU) is being used to prevent the long-term functional consequences of critical illness, sepsis patients need early rehabilitation treatment. Individualized rehabilitation is a safe and effective approach for patients with sepsis. This review aimed to introduce the necessity of rehabilitation for patients with sepsis in the ICU, the composition of the rehabilitation team, the time to begin rehabilitation, the focus of rehabilitation, and the main approaches.
Article Information
- Received
- Accepted
- Published
Academic Editor: Neslihan Lok, Selcuk University, Faculty of Health Sciences
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2022 Ling Wang, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Ling Wang, Department of Intensive Care Unit, People’s Hospital of, Qiandongnan, Miao and Dong Autonomous Prefecture, Kaili, Guizhou 556000, China —
Competing Interests
The authors have declared that no competing interests exist.
Funding
Guizhou Science and Technology Support Plan(2020 4Y139);Qiandongnan Miao and Dong Autonomous Prefecture Science and Technology Support Plan(202112);Cultivation of High-Level Innovative Talents in Guizhou Province
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Sepsis is a life-threatening organ dysfunction that is caused by a patient’s maladaptive response to infection1.Anti-infection therapy and organ function supportive therapy are two focuses of the intensive care unit (ICU). However, recent observational studies have shown ICU processes to be inadequate for the treatment of sepsis: among survivors of sepsis, more patients have serious sequelae 2, 3, 4, while 50% of sepsis patients also have serious psychological problems 5, 6. Finally, sepsis patients have more difficulty returning to the community. During ICU treatment, sepsis patients have a significantly increased chance of developing thromboembolism 7. Limb restraints when applied to the patient for the purpose of safety significantly reduce limb muscle strength 8, which is a negative outcome for many sepsis patients. The use of sedatives has allowed for greater compliance to medical standards in the treatment of sepsis, but it has also brought its own complications. Several factors can lead to the decline of physiological function of patients with sepsis, while incidence of ICU-acquired weakness (ICU-AW) also increases among patients with sepsis 9. Rehabilitation may be associated with a reduced risk of 10-year mortality in the subset of patients with particularly long ICU courses10. Early exercise is of great significance to the rehabilitation of patients with sepsis11. ICU treatment not only is used to rescue patients from life-threatening organ failure, but also provides comprehensive and effective help for patients to return to the community. Rehabilitation therapy is essential for patients with sepsis. Studies have shown that early rehabilitation can reduce the occurrence of delirium, shorten the duration of delirium, reduce the use of sedative drugs, reduce the time of mechanical ventilation, improve heart and lung function, and maintain limb muscle strength 12, 13, 14, 15, 16. Therefore, early rehabilitation is an effective method for patients to maintain physiological function. This review discusses rehabilitation treatment of sepsis patients in ICU. It is intended to inform guidance for clinical practice. Figure 2
Sepsis leads to ICU-AW
ICU-AW occurs in 1 million patients every year 9.In patients with sepsis that leads to multiple organ dysfunction, the incidence of ICU-AW can be as high as 100% 17. Animal studies have shown that sepsis can lead to severe skeletal muscle protein loss, muscle atrophy and muscle weakness, as well as diaphragm and skeletal muscle dysfunction. Diaphragm and skeletal muscle dysfunction are the main causes of ICU-AW in sepsis patients 18. Mechanical ventilation, insufficient nutrition intake, and long-term immobilization are involved in the occurrence of ICU-AW.
Timing of Rehabilitation for Sepsis Patients in ICU
Guidelines have suggested that for patients with respiratory failure that have normal hemodynamics and stability in respiratory function, rehabilitation treatment can be performed 19. One study reported that once the hemodynamics of patients with sepsis mechanical ventilation are stable and appropriate ventilator parameters are set, such as the concentration of inhaled oxygen ≤ 0.6, positive end expiratory pressure < 10 cmH2O, rehabilitation activities should be encouraged 20. Another study suggested that lung rehabilitation of patients with mechanical ventilation can be started 48 - 72 hours after entering the ICU 21. Three studies contended that once the condition of critically ill patients was relatively stable, rehabilitation should be started as soon as possible, preferably within 72 hours, in which case patients benefit significantly better than delayed intervention 22, 23, 24. Moreover, patients can walk on the ground during mechanical ventilation; tracheal intubation was not a contraindication for early rehabilitation exercise 25. During the rehabilitation period, if vital signs fluctuate to such a degree that it deteriorates and endangers the patient’s life, then it is recommended to suspend the rehabilitation treatment 22, 26.
Rehabilitation Goals of Sepsis Patients in ICU
The goal of rehabilitation is to enable a disabled patient to recover their function to the maximum extent that they can, and to return to the community. In the process of rehabilitation, each stage may have a different set of goals for the patient. Rehabilitation is for training patients to improve their function and adapt to the environment, while it also requires the participation of care-members, colleagues, and friends to assist them with a successful return to the community 27.
Development of Rehabilitation Plan for Sepsis Patients
The formulation of a rehabilitation plan and the evaluation of the rehabilitation of ICU sepsis patients are benefited by ICU doctors and rehabilitation doctors working together. ICU doctors will ideally provide effective organ function support, especially respiration and circulation, thus ensuring the stability of vital signs during rehabilitation. Likewise, rehabilitation physicians may perform effective rehabilitation methods according to the patient's condition and preferences, while fully considering the benefits and potential risks of each rehabilitation approach. If there is a change in the patient's condition, the intensity and quantity of rehabilitation measures can be modified accordingly. ICU doctors and rehabilitation physicians are better served by adopting daily evaluation strategies such as to develop personalized rehabilitation programs that are suitable for patients 22, 24.
ICU Rehabilitation Team
Rehabilitation medicine often adopts the "multidisciplinary cooperation clinical rehabilitation integration" rehabilitation model 28, 29, 30. That is to say: this model informs clinicians that they should approach rehabilitation by forming a rehabilitation team. The coordinator of the ICU rehabilitation team is usually a doctor of critical care medicine, and its members include ICU doctors and nurses, rehabilitation doctors, rehabilitation therapists, rehabilitation nurses, respiratory therapists, and psychologists. The rehabilitation team in China also includes traditional Chinese medicine physiotherapists. Figure 1
Figure 1. Impact of delayed ICU rehabilitation in early sepsis. This diagram illustrates the sequential impact of delayed rehabilitation for patients with sepsis as a result of the inflammatory process and the detrimental short and long –term out comes.
Download figure
Figure 2. Cumulative incidences of mortality among intensive care survivors of sepsis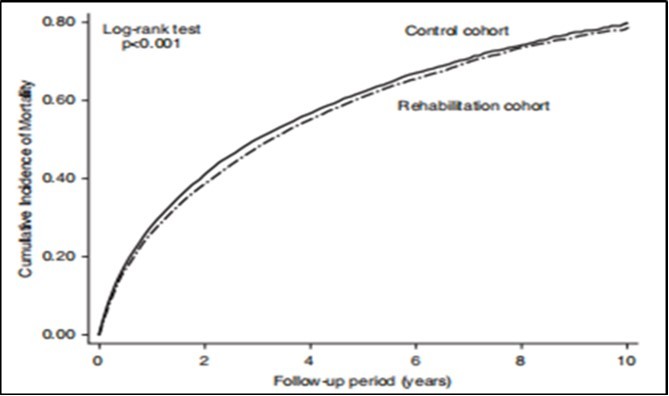
Download figure
Rehabilitation Measures for Sepsis
Commonly used rehabilitation techniques include physical therapy, occupational therapy, psychological counseling and treatment, rehabilitation engineering, rehabilitation nursing, and the physical therapy of traditional Chinese medicine. Patients who are able to cooperate with treatment are benefited by engaging in active rehabilitation training as early as possible, and patients who are unable to cooperate are benefited by taking passive rehabilitation training measures. Lung rehabilitation, heart rehabilitation, psychological rehabilitation, and limb function exercise of sepsis patients are the focus of rehabilitation treatment 31, 32.
Psychological Rehabilitation
Psychological intervention provides emotional support for patients and helps them relieve psychological pressure. At present, there is no unified standard or model for psychological intervention 33, 34, 35. Intervention methods include drug therapy and psychotherapy, usually as combined measures. A study showed that psychological intervention can improve the psychological discomfort reaction of ICU patients and improve the treatment compliance of patients 36. A psychological intervention study conducted by ICU in a hospital in Italy showed that the incidence rate of PTSD decreased significantly within 12 months after discharge from psychological intervention, which was more conducive to the patient’s return to social life 37. An ICU diary can document the experience of patients in ICU; it can help patients fill in the significant loss in memory, and it puts delusional memory in a context, which is also conducive to psychological rehabilitation 38. A randomized clinical trial conducted in 24 ICUs in the UK showed that preventive psychological intervention in ICU not only significantly reduced delirium and fantasy during ICU, but also reduced mental illness after ICU 39.
Physical Function Exercise
The main components of exercise include passive and active exercise in bed, sitting in bed, muscle strength training, bedside standing, and walking 40. Early exercise is more conducive to the recovery of cardiopulmonary function, and it leads to a reduction in the time on mechanical ventilation 41. Researchers have applied an electric rehabilitation machine, combined with functional exercise, to patients with severe pneumonia in order to improve their respiratory function, shorten the duration of mechanical ventilation and their ICU stay 42. For patients who are alert, clinicians can attempt to transition them from passive movement to active movement, that is: the care team can gradually carry out rehabilitation training with the patient by having the patient sit beside the bed, sit in a chair beside the bed, and stand beside the bed 43. When the patient’s muscle strength is greater than or equal to grade 4, they can walk indoors with walking aids or wheelchairs such as to exercise the function of their lower limbs 44. For patients who are not able to cooperate, lateral rotation therapy can be used to prevent soft tissue and joint contracture, peripheral nerve compression and other injuries. For patients who cannot move autonomously after coma or sedation, the joints of their limbs can be moved passively while the patient is lying on the bed. Appropriate interruption of patients’ sedation and rehabilitation training can help reduce the incidence of ICU-AW 43. For alert patients, their legs can be lifted to perform movements akin to riding a bicycle, which increases lower limb muscle strength. Researchers have used the dynamometer to provide resistance exercise training for patients, and the trained patients’ muscle strength is enhanced, while their physical function is also improved when they leave the hospital 45.
Other Rehabilitation Measures
Neuromuscular electrical stimulation is a low-frequency electrical therapy which can prevent muscle atrophy by stimulating nerve fibers to activate motor neurons, thereby increasing blood flow and contractile force of muscle 46, 47. Early acupoint electrical stimulation can improve lower limb muscle strength of patients with sepsis acquired weakness 48. Chinese massage therapy has an advantage in its strong physical penetration despite being non-invasive. Chinese massage therapy stimulates local muscle contraction, promotes blood circulation, and improves neuromuscular excitability. Finally, Chinese massage therapy also dredges channels and collaterals, thereby taking the whole body into account 49.
Conclusion
Individualized rehabilitation is a safe and effective approach for patients with sepsis. Rehabilitation therapy can improve exercise endurance, cardiopulmonary function, and pulmonary function, and it can reduce ICU-related complications. Rehabilitation measure is an important means to realize the successful return of sepsis patients to the community. There remains significant work to be done in the application of rehabilitation medicine to the field of sepsis.
References
- 1.J M Cavaillon, Chrétien F. (2019) From septicemia to sepsis 3.0-from Ignaz Semmelweis to Louis Pasteur. , Genes & Immunity 5, 371-82.
- 2.Scherag A, C S Hartog, Fleischmann C. (2017) A patient cohort on long-term sequelae of sepsis survivors: study protocol of the Mid-German Sepsis Cohort. , BMJ Open 8, 016827.
- 3.Gtz T, Günther A, O W Witte, F M Brunkhorst, Hamzei F. (2014) Long-term sequelae of severe sepsis: Cognitive impairment and structural brain alterations - an MRI study (LossCog MRI). , BMC Neurology 1, 145-48.
- 4.Taito S, Hatori H, Shimogai T. (2018) Do change of care and rehabilitation for patients with mechanical ventilation increase chances of return to work? : Discussion on organ support therapy in the intensive care unit and return to work: a nationwide, register-based cohort study. Intensive Care Medicine. 7, 998-99.
- 5.Young D, Barber V, Griffiths J, D A Harrison, P A Watkinson. (2020) Depression and post Traumatic stress disorder after critical illness: a UK-wide prospective cohort study. , Critical 1, 310-14.
- 6.Nikayin S, Rabiee A, M D Hashem. (2016) Anxiety symptoms in survivors of critical illness: a systematic review and meta-analysis. , General Hospital Psychiatry 6, 23-29.
- 7.Royster W, Ruff S, Patel V, Nicastro J, Coppa G et al. (2018) Sepsis is a risk factor for developing deep vein thrombosis after open colectomy. , International Journal of Surgery 1, 305-06.
- 8.S M Parry, Z A Puthucheary. (2015) The impact of extended bed rest on themusculoskeletal system in the critical care environment. , ExtremPhysiol Med 1, 16-18.
- 9.Fan E, Cheek F, Chlan L, Gosselink R, Naeem A. (2017) An official american thoracic society clinical practice guideline: the diagnosis of intensive care unit-acquired weakness in adults. , American Journal of Respiratory & Critical Care Medicine 12, 1437-40.
- 10.P W Chao, C J Shih, Y J Lee. (2014) Association of postdischarge rehabilitation with mortality in intensive care unit survivors of sepsis. , American Journal of Respiratory & Critical Care Medicine 9, 1003-1011.
- 11.Kayambu G, R J Boots, J D Paratz. (2011) Early rehabilitation in sepsis: a prospective randomised controlled trial investigating functional and physiological outcomes The i-PERFORM Trial (Protocol Article). , Bmc Anesthesiology 1, 1-11.
- 12.C J Tipping, Harrold M, Holland A, Romero L, Nisbet T et al. (2017) The effects of activemobilisation and rehabilitation in ICU on mortality and function:a systematic review . , Intensive Care Med 2, 171-83.
- 13.Alvarado P M, Girbau M A, Garcia S A. (2018) Current situation of rehabilitation before the implementation of a program of early mobilization in a polyvalent ICU. , Annals of Physical and Rehabilitation Medicine 61, 295.
- 14.Tipping C, Harrold M, Holland A. (2004) Systematic review of the effects of early rehabilitation of ICU patients on mortality and function. , Journal of the Egyptian Society of Parasitology 3, 999-1008.
- 15.D L Li, X M Huang, S K Cen, Z J Meng, H Y Yan et al. (2018) Effect of early rehabilitation therapy on complications and prognosis in mechanically ventilated elderly patients with severe pneumonia. , Chinese Journal of Respiratory and Critical Care Medicine 1, 46-50.
- 16.D E Anekwe, s S Bi, Bussières A, Spahija J. (2019) Early rehabilitation reduces the likelihood of developing intensive care unit-acquired weakness: a systematic review and meta-analysis. , Physiotherapy 1, 1-10.
- 17.Latronico N, Herridge M, Hopkins R O, Angus D, Needham D M. (2017) The ICM researchagenda on intensive care unit-acquired weakness. Intensive Care Med. 9, 1270-81.
- 19.Severe Rehabilitation Committee of physical medicine and Rehabilitation Branch of Zhejiang Medical Associationet al. Expert consensus on severe rehabilitation in Zhejiang Province. , Zhejiang Medicine 24, 2191-96.
- 20.Bailey P, G E Thomsen, V J Spuhler. (2007) Early activity is feasibleand safe in respiratory failure patients. , Crit Care Med 1, 139-45.
- 21.Ding N, Zhang Z G, Zhang C Y, Li Y. (2019) What is the optimumtime for initiation of early mobilization in mechanically ventilated patients? A network meta-analysis. , PLoS One 10, 0223151.
- 22.H M Zhao. (2019) Individualized rehabilitation therapy for critically ill patients. , Chinese Journal of Tuberculosis and Respiration 9, 656-59.
- 23.S A Andreychenko, A V Serezhechkin, M V Bychinin, T V Klypa. (2020) Comparison of early and delayed rehabilitation outcomes in patients at the intensive care unit. Anesteziologiia i Reanimatologiia. 1, 51-56.
- 24.Uthup B R, Myszenski A, Saigh N, Samuel P S. (2021) Evaluating the Benefits of Early Intensive Rehabilitation for Patients With Sepsis in the Medical Intensive Care Unit: A Retrospective Study. Journal of Acute Care Physical Therapy, publish ahead of print.
- 25.C L Hodgson, Stiller K, D M Needham. (2014) Expert consensusand recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults . , Crit Care 6, 658-61.
- 26.Sommers J, R H Engelbert, Dettling-Ihnenfeldt D. (2015) Physiotherapy in the intensive care unit: an evidence-based, expert driven, practical statement and rehabilitation recommendations. , Clinical Rehabilitation 11, 1051-63.
- 27.Enjalbert M, Thevenot F, Motte G, J M Théry. (2015) Prévoteau B. Intensive care in rehabilitation and rehabilitation in intensive care. , Annals of Physical and Rehabilitation Medicine 58, 47.
- 28.H Z Shao, Ye L, B Y Qin. (2020) Research progress of early rehabilitation therapy for critically ill patients. , Chin J Crit Care Intensive Care Med 2, 206-10.
- 29.Momsen A, Rasmussen J, Nielsen C, Iversen M, Lund H. (2012) Multidisciplinary team care in rehabilitation:An overview of reviews. , Journal of rehabilitation medicine : official journal of the UEMS European Board of Physical and Rehabilitation Medicine 11, 901-12.
- 30.M P Selina, Peter N, Dale M N N. (2018) Implementing early physical rehabilitation and mobilisation in the ICU: institutional, clinician, and patient considerations. , Intensive Care Medicine 4, 470-73.
- 31.Mazza A, Paneroni M, Vitacca M, Ambrosetti M. (2019) The new concept of rehabilitation space. in the era of the Digital Health in cardio-respiratory rehabilitation. Giornale Italiano di Medicina del Lavoro ed Ergonomia 2, 121-24.
- 32.Sato R, Ebihara S, Kohzuki M. (2017) Recent Advances in Pulmonary Rehabilitation for Patients in the Intensive Care Unit (ICU). , Pulmonary Research & Respiratory Medicine-open Journal, Special Edition 2, 51-54.
- 33.Davis C, I A Faruk, Breyer D, R E Cumble, Zane R. (2020) The case for virtual sepsis surveillance and Intervention. Telemedicine and E-Health. 4, 335-39.
- 34.Huang W, Qin Y, Dai X. (2019) Breakthroughs in global critical care medicine. , Chinese Critical Care Medicine 1, 1-7.
- 35.Sosnowski K, Lin F, M L, White H. (2015) Early rehabilitation in the intensive care unit: An integrative literature review. , Australian Critical Care 4, 216-25.
- 36.Hua X, J Zhao Li, X. (2009) Influence of psychological intervention on mental stress and therapeutic compliance degree of patients in intensive care unit. , Chinese General Nursing 8, 2075-76.
- 37.Peris A, i M Bon, Iozzelli D, M L, Belloni L. (2011) Early intra-intensive care unit psychological intervention promotes recovery from post traumatic stress disorders, anxiety and depression symptoms in critically ill patients. , Critical Care 1, 1-10.
- 38.Jones C, Ckman B C, Capuzzo M, Egerod I. (2010) Intensive care diaries reduce new onset post traumatic stress disorder following critical illness: a randomised, controlled trial. , Critical Care 5, 1-10.
- 39.Wade D M, Mouncey P R, Richards-Belle A, Wulff J, Rowan K M. (2019) Effect of a nurse-led preventive psychological intervention on symptoms of posttraumatic stress disorder among critically ill patients: a randomized clinical trial. , JAMA The Journal of the American Medical Association 7, 665-66.
- 40.R K Lord, C R Mayhew, Korupolu R. (2013) ICU Early Physical Rehabilitation Programs: Financial Modeling of Cost Savings. , Critical Care Medicine 3, 717-24.
- 41.Nugent K, Edriss H. (2017) Official american thoracic society/american college of chest physicians clinical practice guideline: liberation from mechanical ventilation in critically ill adults. The Southwest Respiratory and Critical Care Chronicles. 19, 1-4.
- 42.X F Wang, K F Song, Zhou Q. (2019) Application of electric rehabilitation machine combined with functional exercise in rehabilitation of mechanically ventilated patients with severe pneumonia. , Journal of Qilu Nursing 13, 21-23.
- 43.Sommers J, R H Engelbert, Dettling-Ihnenfeldt D. (2015) Physiotherapy in the intensive care unit: an evidence-based, expertdriven, practical statement and rehabilitation recommendations . , Clin Rehabil 11, 1051-63.
- 44.Fuest K, S J. (2018) Recent evidence on early mobilization incritical-ill patients. , Curr Opin Anaesthesiol 2, 144-50.
- 45.Santos M A D, Camargo P N R, Ximenes C M T, S J Cristina, C D Machado et al. (2017) Effects that passive cycling exercise have on muscle strength, duration of mechanical ventilation, and length of hospital stay in critically ill patients: a randomized clinical trial. Jornal Brasileiro De Pneumologia Publicacao Oficial Da Sociedade Brasileira De Pneumologia. , E Tisilogia 2, 134-39.
- 46.Stefanou C, Karatzanos E, Mitsiou G. (2016) Neuromuscular electrical stimulation acutely mobilizes endothelial progenitor cells in critically ill patients with sepsis. , Annals of Intensive Care 1, 21-25.
- 47.Patsaki I, Gerovasili V, Sidiras G. (2017) Effect of neuromuscular stimulation and individualized rehabilitation on muscle strength in Intensive Care Unit survivors: A randomized trial. , Journal of Critical Care 8, 76-82.