
Examining the Low Women Autonomy in Household Decision Makings in Sidama Zone, Southern Ethiopia
Abstract
The low level of women autonomy and the key pre disposing factors affecting household decision makings among many population groups in Ethiopia is not well understood among scholars, and is less investigated. This study examined the status and the micro level factors associated with women autonomy in Sidama, the most populous zone in Southern Ethiopia. A simple random sampling technique (using the available complete listing of households) was used to select the 231 sample households from one of the districts of the zone. Sidama zone was selected due to its historically strong customs of patriarchal family system. Quantitative and qualitative data were obtained using structured questionnaire and focus group discussions. Household, women and husband characteristics were used as explanatory variables while women autonomy index, developed from a set of questions, served as the dependent variable. The study revealed that women’s decision makings on core household and personal issues were very low in the study population. The predicted probability, using Ordinary Least Square Regression shows that women’s education, alcohol intake by husbands, household size and land size were the main determinants of autonomy in decision makings in the study area. The study recommended that concerned bodies should capitalize on educating women and girls through both formal and informal learning platforms, promote income generation activities through entrepreneurship, increased access to property and economic assets, training, microfinance and markets.
Article Information
- Received
- Accepted
- Published
Academic Editor: Manjubala Dash, Mother Theresa Postgraduate & Research Institute of Health Sciences, Pondicherry, 605006, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Eyasu Regassa, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Nigatu Regassa, Visiting research scholar, University of Saska, tchewan, SK, Saskatoon, Canada —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Background
Autonomy is understood as the ability to obtain information and make decisions about one's own concerns. Studies often assess women’s autonomy with an index measuring participation in decision making about various household issues such as major and minor household purchases, freedom of movement and decisions on household finance (Dabere et al, 2014;Woldemicael, 2007;Tiwari and Kumar, 2006; Bloom et al, 2001). Autonomy in decision makings at household level facilitates access to various household resources such as food, land, income and other forms of wealth, and social resources such as knowledge, power, prestige within the family and community (Mullany, 2006; Chanan, 1996). On the contrary, various studies reported that when women exercise low status and autonomy, their ability to obtain access to certain strategic resources (such as health services) declines, and in turn face various social and economic burdens (Jane, 2015; Dev et al, 2010). For instance, women's final say in decisions regarding day-to-day household purchases and spousal communication are significant explanatory variables in health seeking behaviors and fertility preferences (Woldemicael , 2009).
In Ethiopia, like many other patriarchal societies, women have little or no autonomy in every measure and standard (CSA and Macro, 2011; Hirut, 2010). Lack of access to productive resources such as land; lack of access to education, employment opportunities, basic health services, and protection of basic human rights; low decision making; violence and harmful traditional practices are some of the indicators of the socioeconomic marginalization of women in the country. Ethiopia is traditionally a patriarchal society that keeps women in a subordinate position and there is a belief in the general population that women are docile, submissive, patient and tolerant of monotonous work and violence (Hirut, 2010; Emebet, 2008). In the process of upbringing, boys are expected to learn and become self-reliant, major bread winners, and responsible in different activities, while girls are brought up to conform, be obedient and dependent, and specialize in indoor activities like cooking, washing clothes, fetching water and caring for children (Hirut, 2010; Emebet,2008; ESPS, 2008; UNFP, 2008; APFSU, 2007).
Despite the fact that the legal reforms undertaken over the last two decades with respect to protecting the rights of women and girls are found to be truly significant, it has far distance to get down to the household level. This is to say that women are still victims of various social and demographic outcomes mainly due to lack or absence of autonomy at household level. For example, a recent study on intimate partners’ violence in southern Ethiopia indicated that about 32 percent of women were abused by their husbands, ranging from verbal attack to severe physical assault (Nigatu,2011). While further studies are required, it can be said that the low autonomy in decision makings has significantly impacted women’s level of access and control over many community resources. For example, the National Demographic and Health Survey of Ethiopia (CSA and Macro, 2011) reported that only 25 percent of Ethiopian women were being attended by skilled health professionals partly due to their low decision making autonomy; that 57 percent of currently married women were employed compared to 99 percent of currently married men; and 30 percent of currently employed women were not paid for their work compared to 9% of men. As far as decision making in regards to three important dimensions, the report revealed that 54 percent of women participate in all 3 domains of decisions (health care, major household purchases and visits to family).
Previous studies have documented several factors associated with women’s low autonomy and decision makings at households. These factors usually revolve around women’s characterstics, household characteristics and husbands’ socio economic status. Women’s education is the most frequently reported variable in previous studies (Sultana, 2011; Dev 2010; Ami, 2008; Bloom et al, 2001). Other studies reported positive associations with women’s age, residence, employment and number of living children (eg. Dev et al, 2010). Studies on women autonomy in Southern Ethiopia, especially in the study zone, are very few. These few studies target some specific aspects of women’s access and control over resources (such as land, microfinance, health care or related domains), and many did not directly deal with women autonomy in its own right.
Therefore, this study attempts to answer the questions “What is the overall status of women autonomy (using broader domain of proxy variables) and what are the key predictors of women autonomy in decision makings?” in one of the districts in Southern Ethiopia (Hawassa Zuria District).
Methodology of the Study
The Study Setting
Sidama Zone is one of the 13 zones found in Southern Nations Nationalities and Peoples Regional State (SNNPRS) of Ethiopia. It is located in the North Eastern part of the region and bordered by Oromiya region in the North, East and Southeast, with Gedeo Zone in the South, and Wolaita Zone in the West (see Figure 1 below). The zone has a total area of 7200 Km2 divided into 19 Woredas/ districts/ and 2 city administrations. According to the zonal finance and economic development office, Sidama was estimated to have a total population of 3, 218,671 which takes the share of 19.78 % of the regional population. The average population density of the Zone was 461 people per kilometer square, making it one of the most densely populated zones in the region/country. A substantial area of the Sidama land produces coffee, which is the major cash crop in the region. Corn, wheat, barley and pepper are also produced in the zone. Chat and Pineapple are increasingly becoming common cash crops in the Zone next to coffee production. The study district is Hawassa Zuria with 23 kebeles (smallest administrative unit). The area size of the Woreda is 22, 643 hectare, and dry zone accounts 75 %.(SZFEDB, 2003). The total population of the district is 139,654 of which female population accounts 69, 158.
Figure 1. Administrative Map of the study area.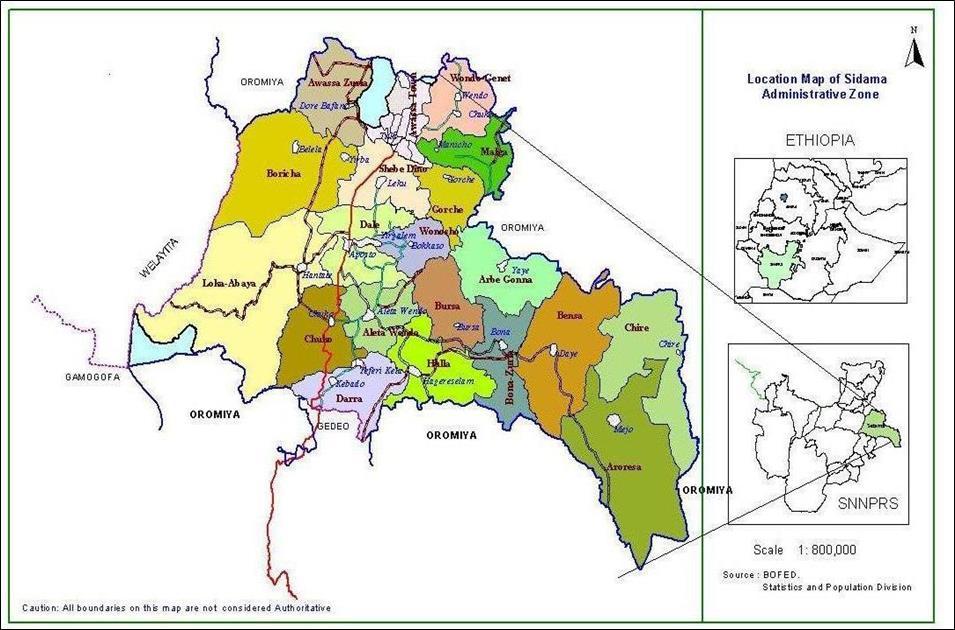
Download figure
Source: (Hawassa Zuria Woreda, Finance and economic development, information dissemination work process pamphlet, Volume 1, No 2, 2004,)
Note: Under ethnic based federalism of Ethiopia, a zone is defined as a relatively independent administrative unit in a province/region. A zone consists of several districts (woredas) and the districts in turn are composed of several villages (locally known as kebeles).
Data Source and Sampling Design
The study is a cross sectional quantitative study. The major data for this study were generated from married women accessed through household survey.
Once the study district was randomly selected from a total of 19 districts in the zone, a sample of 231 households was determined using the Cochrane population based sampling formula (Cochrane 1977) , taking into account precision level of 5% and level of women autonomy from previous studies. Three villages (kebeles) were randomly selected (namely Dore Bafano, Labu Koromo,Jara Damuwa kebeles) from the total list of 23 villages. More than 90 percent of the population in the three kebeles practice mixed agriculture and are among the most food insecured villages in the district. Then, from each selected kebele, we took 10 percent of the households, giving a size of 90, 110, and 31 households for the three kebeles respectively.
Data Collection
The data for this study were generated using a well structured interview schedule. The instrument, among other things, contained demographic and socio-economic characteristics of the respondents, women autonomy indicators and husband characteristics. Information on the dependent variable (women autonomy) was collected using more broader domains of participation in household decision makings. To better address the women’s safety and confidentiality of the information, we hired three women health extension diploma holders for data collection. The data were collected from women respondents using local language (Sidamigna). Pre-testing of the questionnaire and training of data collectors were performed before data collection commenced. Further, based on the recommendation of WHO (2001), safety and ethical considerations in the collection of autonomy and violence data were observed. For instance, we conducted the interview in a private setting in view of keeping the secrecy of the responses given by the respondent. The data collection took about 25 days.
Data Processing and Analysis
The study employed univariate analysis to describe the characteristics and other selected variables. In order to examine the association between the dependent variable (women autonomy) and the explanatory variables, multi-variate statistical techniques (ordinary least square regression model) was used. The model provides the net effect of each predictor controlling for the effects of confounding factors. This model assumes that a one unit change in the outcome variable associated with a given change in an independent variable is the same at any point in the outcome scale.
The dependent variable was measured by autonomy index computed from affirmative responses of decision making questions used in most studies (eg. CSA & Macro International, 2011; Dev et al, 2010). The DHS questionnaire, for instance, commonly uses four areas of women's autonomy in decision making, which includes decision makings on own health care, making major household purchases, making purchase for daily household needs and visits to her family or friends. In other studies women’s autonomy was measured by the composite index of three constructs of women’s autonomy: control over finance, decision-making power and extent of freedom of movement (Dabere et al, 2014; Woldemicael, 2007;Tiwari and Kumar, 2006; Bloom et al, 2001).
In the present study, we used eight autonomy indicators which include: decision maker on the use of wife’s money, major household sales and purchases, number of children to have, relatives visit, daily household needs, pregnancy and delivery time, and decision maker on sale of cattle or crops in need of finance to the household. After computing only the respondents’ and joint decisions with her husband, excluding responses of decisions made by the ‘’husbands alone and others decision’’, a continuum scale of 0 to 8 was formed where 0 represents ‘’no autonomy’’ and the scores ‘’1-8’’ represent ’’ some autonomy’’ in the scale.
Twelve socio economic and demographic variables were used as independent variables selected based on review of literature and model building procedure. The independent variables used in the study are: age difference between the spouses (commonly used as a proxy for power balance between husband and wife), education level of the husbands, educational status of the respondents, wealth index of the households (computed based on ownership of nine household assets), marital form or polygamy, husband frequency of alcohol taking, age of the respondents, household size, household members aged 15-64, duration or stay in area, land size, and work status of the respondents. We tested multi co-linearity among these independent variables using variable inflation factor (VIF), and all explanatory variables were found to be fairly independent of each other.
Results
Background Characteristics
Table 1 presents the socio economic characteristics of the respondents. It is seen that the large majority of the respondents (73.6 percent) did not have education or were illiterate The distribution of the respondents by religion shows that the protestant Christians take the biggest share (89.6 percent) and the remaining groups account for smaller proportions: Catholic (3.9 %) followed by Muslims ,others (2.2 %) and Orthodox (1.3 %). Husbands level of education indicates that larger proportion of them (43.7 percent) were at primary level of education.
Table 1. Percentage distribution of respondents by selected socio- economic and demographic characteristics, Sidama Zone, Hawassa Zuria Disrict, SNNPR, Ethiopia. (n=231)| Characteristics | Percent |
|---|---|
| Literacy Status of the Respondents | |
| Yes | 26.4 |
| No | 73.6 |
| Religion | |
| Orthodox | 1.3 |
| Catholic | 3.9 |
| Protestant | 89.6 |
| Muslim | 2.2 |
| Traditional | 0.8 |
| Others | 2.2 |
| Education Level of the Husbands | |
| Primary (1-6) | 43.7 |
| Secondary (7-8) | 11.3 |
| Higher Secondary (9- 12) | 2.6 |
| College diploma | 2.6 |
| College degree | 1.7 |
| No education | 38.1 |
| Wealth status of the households | |
| Poor | 57.6 |
| Medium | 40.7 |
| Better | 1.7 |
| Marital Form | |
| Polygamous | 22.9 |
| Monogamous | 77.1 |
| Main income Source of the Respondents | |
| Husband’s Money | 71.9 |
| Respondents own Saving | 10.8 |
| Support from Relatives, Government or NGO | 6.5 |
| From Sales of Cattle/Crops | 7.4 |
| From Formal Employment | 2.6 |
| Other | 0.8 |
| Land Size of the Household | |
| 0-025 hectare | 0.4 |
| 0.25-0.50 hectare | 27.7 |
| 0.5-1 hectare | 45 |
| 1-2 hectare | 23.8 |
| Above two hectare | 1.7 |
| Household size | |
| 0-3 | 13.9 |
| 4-6 | 40.3 |
| Above 6 | 45.8 |
| Headship of the Household | |
| Female | 8.7 |
| Male | 91.3 |
The analysis showed that 22.9 percent of the women were engaged in polygamous marriage arrangement, which is almost twice the national average (i.e. the DHS 2011 reported 11% for the country). Majority of the respondents (71.9 percent) reported that they depend on income generated only through their husbands, and only 10.8 percent reported from own saving, 6.5 percent support from relatives or aid from Government or NGOs, and 7.4 percent from sales of cattle and crops. Land ownership by households was small and fragmented. About 45 percent of the households owned between 1-2 hectares and more than 50 percent of the households owned less than 1 hectare. Wealth index computed based on households’ ownership of nine common assets (electricity, sewing machine, cart, mobile phone, flashlight, corrugated iron roofing, bike, radio and kerosene lamp) indicates that 57.6 percent of the households were classified as having low (0-3 assets) wealth status, 40.7 percent labeled as medium and very small proportion of the respondents in better wealth status.
Majority of the respondents reported to have above 6+ children (45.8 %) followed by 4-6 (40.3 %) and 0-3 (13.9 %). About 91 percent of households were male headed while the remaining small proportions were female headed.
Women Autonomy Indicators
As described in the methods section above, we measured autonomy using a set of eight household decision making questions which are commonly used by other researches. These questions were used to form the continuous dependent variable by composing the affirmative responses. (See Table 2).
Table 2. Percentage distribution of respondents by reported participation in selected domains of household decision makings, Sidama Zone, Hawassa Zuria District, Southern Ethiopia. (n=231)| Indicators | Percentage |
|---|---|
| Decision maker on the use of wife’s money | |
| Respondent | 10 |
| Husband | 74 |
| Both jointly | 14.7 |
| Others | 1.3 |
| Decision maker on the use of husband's money | |
| Respondent | 4.8 |
| Husband | 82.7 |
| Both/ jointly | 12.5 |
| Decision maker on relatives visit | |
| Respondent | 7.4 |
| Husband | 82.3 |
| Both /jointly | 10.3 |
| Decision maker on major household sales & purchases | |
| Respondent | 11.7 |
| Husband | 79.2 |
| Both/ jointly | 9.1 |
| Decision maker on daily household needs | |
| Respondent | 16.9 |
| Husband | 64.9 |
| Both/ jointly | 17.7 |
| Other | 0.5 |
| Decision maker on pregnancy and birth time of the respondent | |
| Respondent | 6.9 |
| Husband | 66.7 |
| Both/ jointly | 26.4 |
| Decision maker on number and sex of children | |
| Husband* | 66.7 |
| Both /jointly* | 27.7 |
| Decision maker on sales of cattle and crops | |
| Respondent | 10.4 |
| Husband | 89.6 |
| Variables@ | B | Std. Error | Sig. |
| (Constant) | -1.826 | 1.955 | 0.351 |
| Age difference between spouses | -0.025 | 0.022 | 0.271 |
| Education level of the husbands | -0.047 | 0.066 | 0.478 |
| Educational status of the respondents | 1.053 | 0.362 | .004** |
| Wealth index of the households | 0.172 | 0.28 | 0.541 |
| Marital form/polygamy | -0.101 | 0.365 | 0.783 |
| Husband frequency of alcohol use | -0.332 | 0.105 | .002** |
| Age of the respondents | -0.271 | 0.491 | 0.582 |
| Household size | 0.212 | 79 | .008** |
| Household members aged 18-64 | -0.223 | 0.121 | 0.067 |
| Duration/ of stay in the area | 1.19 | 1.245 | 0.34 |
| Land size owned | 0.578 | 0.267 | .031* |
| Work status of the respondents | 0.282 | 0.302 | 0.351 |
It can be inferred from Table 2 that 74.7 percent of the respondents do not participate in the decision on the money generated by themselves while 14.7 percent reported joint decisions. Similarly 81.7 percent of the respondents have no say on the money coming from the husband. The large majority of the respondents (81.3%) reported that decisions regarding their visits to relatives are made by husbands, and only 10.4 percent of then decide jointly. Most decisions on major household sales and purchases are made by husbands (79.2 percent) and few jointly (9.1 percent).
In 64.9 percent of the households, decision maker on daily household needs are husbands, 16.9 percent by the respondent and 17 percent jointly. Husbands are also the one making most decisions regarding pregnancy and timing of next birth (See Table 2).
Predictors of Women Autonomy: Multivariate Analysis
For the multivariate analysis, we selected 12 key explanatory variables based on literature review and model building procedures to see their net effects on the outcome variable of interest using Ordinary Lest Square regression (OLS) model.
Accordingly, four out of twelve independent variables were found to have association with women autonomy at different level of significance. These are: literacy status of the respondents (p=0.004)**, husband’s frequency of alcohol use, (p=0.002)**, household size, (p=0.008)** and land size (p =0.031)*. The others ; age difference between the spouses, education level of the husband, wealth index of the households, marital form or polygamy, age of the respondent, household members aged 18-64, duration of stay in area, and respondents work statues, have shown no significant association with the outcome variable of interest.
It is indicated that a one unit change in educational status brings about 1.053 units change in the level of women autonomy. (B=1.053and P-value 0.004). Also a one unit change in husband’s frequency of alcohol use brings about a decrease in the level of autonomy by 0.332 units. Similarly, a unit change in household size brings about increase in women autonomy by 0.212 units indicating positive relationship. Finally, it is also seen that increase in household land size by one unit results in increase of women autonomy by 0.578 units.
Discussion
This study examined the level of women autonomy and the micro level factors associated with women’s decision makings in one of the most populous zones in Southern Ethiopia (the Sidama zone). The results presented in previous section are based on a representative sample of 231 women respondents taken from one of the randomly selected districts of the zone. It is understood from the analysis that quite large proportion of women experiences little or no autonomy, and do not participate in decision makings of major household affairs. If one looks at the different rates given for each autonomy indicators shown in Table 2, it appears that women’s participation in household decision makings is unacceptably low. The fact that seventy four percent of the decisions on wife’s income is made by the husband alone, suggests the prevailing low women autonomy in the study area.
We found out that the factors associated with low autonomy were related to either the women’s characteristics or household socio-economic status, or husband’s characteristics. The most important characteristics predicting autonomy was educational status. Women with more education tend to be more assertive, and thus will not settle for less in their gender relationships. This has been corroborated by similar studies in Ghana by Ami (2008). A national level study in Nepal(Dev et al, 2010) reported that highly educated women were more likely to take part in decision making in their own health care. This is mainly due to the fact that education may impart feelings of self-worth and self-confidence, which are more important features in bringing about changes in health-related behavior than exposure to relevant information (Bloom et al, 2001). Sultana (2011) documented that women's educational attainment, occupation and income were positively related to women decision-making power at household level.
In relation to the husbands’ characteristics, alcohol taking has appeared as important risk marker for low autonomy. It was observed that wives of men who do not drink alcohol are more autonomous. The alcohol taking behavior of husbands may particularly affects the decision makings on household expenditure and family visits. Population based surveys from Brazil, Cambodia, Canada, Chile, Colombia, Costa Rica, El Salvador, India, Indonesia, Nicaragua, South Africa, Spain and Venezuela also found similar relationship between a woman’s risk of suffering violence and lack of autonomy and her partner’s drinking habits (Ellsberg,2000). It is believed that alcohol operates as a situational factor, increasing the likelihood of violence by reducing inhibitions, clouding judgment and impairing an individual’s ability to interpret cues.
As far as household size is concerned, we found in this study that women living in large households are more likely to be autonomous than those women living in small household size. Previous studies in Ethiopia (eg. Desalegn, 2008) has also reached similar conclusions on the effect of household size on women autonomy. The national level study in Nepal (Dev et al, 2010) also reported a strong positive relationship between number of living children (which can be a proxy of family size) and decision-making participation, indicating that the more children women have, the more likely they participate in decision making in all domains.
This study hypothesized that women living in household with large land size are more likely to be autonomous than those living in households owning small land size. The multivariate analysis has witnessed positive associations between the two variables i.e. as land size owned by the household increases, the level of women autonomy also increases. It was reported in previous section that nearly half of the households owned 1-2 hectare of land. One possible explanation for the reported association between the two variables may be the higher prevalence of polygamous women (about 22%) who usually live in households where husbands own larger land size since such marital system has historically been based itself on adequate availability of land and cattle resources. According to the customs in such marital arrangement, husbands stay with their different wives alternatively, leaving these wives with some window of autonomy to administer household resources(such as land). Consistent to this finding, a regional level study (UN-HABITAT, 2008) reported that women who owned their own land and has land certification cards are more likely to be autonomous than those who use land with their husbands and land not certified.
Finally, there is one main drawback of this study worth mentioning. The findings of this study are based on cross-sectional data collected from women respondents, and hence, the information collected on their husbands’ characteristics might have been affected by some omissions and biases. Thus, until large scale longitudinal data collection from husband and wife is possible, this study can only be used to understand household level factors associated with the unacceptably low autonomy in decision makings from women’s perspectives. Despite such weaknesses, it is believed that this work contributes to our understanding of the problem and provides some direction to decision makers in Sidama zone, Southern Ethiopia.
Conclusions
This study has documented that women’s autonomy is unacceptably low in the study area, and women are excluded from many of the strategic household decisions. In view of the fact that education has appeared as one of the key predictors of the outcome variable, attention should be given to increasing females’ participation in formal education. Also, it is equally important to promote peer education at household and community levels for improved husband-wife communication as it is central to women's autonomy in decision making. The local government should also give attention to rural women's involvement in income generation activities; ensure women’s access to property through land ownership certificate and other economic assets.
References
- 1.ADF(African Development Forum)(2008)Action on achieving gender equality, women empowerment and ending violence against women in Africa: UN conference center,Addis Ababa,Ethiopia.
- 2.APFSU(African Partnership Forum Support Unit)(2007)Gender and economic empowerment in Africa: A paper presented to the 8th meeting of African Partnership Forum.Berlin.22-23,May2007.
- 3.Bloom S S, Wypij D, Das Gupta M. (2001) Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. , Demography 38(1), 67-78.
- 5.. CSA & Macro International (2011). Ethiopian Demographic Health Survey, (2005).CSA: Addis Ababa , Ethiopia .
- 6.Nigatu Dabere.Abebe Gebremariam, Muluemebet Abera, Tesfaye Setegn, and Kebede Deribe (2014).. Factors associated with women’s autonomy regarding maternal and child health care utilization in Bale Zone: a community based cross-sectional study. doi: 10.1186/1472-6874-14-79. , BMC Womens Health 14, 79.
- 7.Dev R Acharya, Jacqueline S Bell, Simkhada Padam, Teijlingen Edwin R Van, Pramod R Regmi. (2010) Women's autonomy in household decision-making: a demographic study in Nepal. Reproductive Health. Vol.7 15.
- 8.Ellsberg M C. (2000) Candies in hell: women’s experience of violence in. , Nicaragua. Social Science and Medicine 51, 1595-1610.
- 9.Emebet Mulugeta(2008).“negotiating poverty’: problems and coping strategies of women in five cities of Ethiopia.
- 10.ESPS(Ethiopian Society of Population Studies)(2008).Gender inequality and women empowerment:. in deep analysis of the Ethiopian Demographic & Health Survey2005,Addis Ababa,October 2008,Ethiopia .
- 11.Bekele Hirut. Ethiopia,PhD Dissertation(unpublished),Wageningen University (2010) Targeting married women in microfinance program for women empowerment:Evidence from.
- 12.Jane O Ebo. (2015) Girl Power!” The Relationship between women's autonomy and children's immunization coverage in Ethiopia.DOI: 10.1186/s41043-015-0028-7.Journal of Health. , Population and Nutrition 33, 18.
- 13.Mullany B C, Hinde M J, Becker S. (2005) Can women’s autonomy impede male involvement in pregnancy health. in Kathmandu, Nepal?doi: 10.1016/j.socscimed.2005.04.006.Social Science and Medicine.61 : .
- 14.Regassa Nigatu. (2011) Intimate partners’ violence among selected populations in Southern Ethiopia. Examining the prevalence and risk factors. , International Journal of Sociology and Anthropology 4(1), 13-22.
- 15.Zone Sidama. (2003) Finance and Economic Development Bureau/ SZFEDB.Population projection and socio economic profile of Sidama. , Magazine, Vol.2,SNNPR,Ethiopia
- 16.Sultana M Alam. (2001) Factors effect on women autonomy and decision-making power within the household in rural communities. , Journal of Applied Sciences Research,01/2011; 7, 18-22.
- 17.Tiwari M, Kumar K. (2006) . Women’s Autonomy and Utilization of Maternal and Child Health Care Services in India .
- 18.UNFP.Nations Population Fund)(2008). Ethiopian population and development indicators. Addis Ababa, Ethiopia.web address http:/www.unifw.org/gender employment.htm, accessed in Sep,2013.
- 19.Woldemicael G. (2007) Do women with higher autonomy seek more maternal and child health-care? Evidence from Ethiopia and Eritrea. Rostock Germany:MPIDR Working Paper;.
- 20.Woldemicael G.(2009);.Women's autonomy and reproductive preferences in Eritrea. , J Biosoc Sci 41(2), 161-81.
Cited by (1)
This article has been cited by 1 scholarly work according to:
Citing Articles:
Girma Teferi Mengistu, Sena Kitila, Mesfin Beharu Deme - Journal of Medicine, Physiology and Biophysics (2021) Semantic Scholar