Abstract
Background
HIV causes immunosuppression, which reduces the body's immunity to diseases like COVID-19 by decreasing CD4 cells. The goal of this study is to determine whether persons living with HIV/AIDS (PLWHA) who are using anti-retroviral therapy (ART) are willing to accept the Coronavirus illness 2019 vaccination and the factors that influence their decision.
Method
From February 15 to March 15, 2022, 332 PLWHA on ART participated in this facility-based cross-sectional study. The correlation of outcome variables with predictors was investigated using binary and multivariable logistic regression.
Result
Of the 332 study participants, 110 (33.1 %) and 118 (35.5 %) had poor knowledge and a negative attitude toward the COVID-19 vaccination, respectively. Approximately 31 (9.3%) of study participants believe ART medications can also prevent COVID-19 infection. The willingness to receive the COVID-19 vaccine was 66.3 % with a 95 % confidence interval (60.9, 71.5). Knowledge, attitude, educational status, marital status, residency, duration, and monthly income were all significant predictors of willingness to receive COVID-19 vaccination.
Conclusion
Increased sensitization regarding the necessity of vaccines and the negative consequences of diseases, particularly among PLWHA, should be emphasized in the preparation of the COVID-19 immunization campaign involving prominent individuals such as health professionals and religious leaders.
Author Contributions
Academic Editor: Jean-Pierre Routy, Faculty of Medicine McGill University Health Centre (MUHC).
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2023 Abayneh Tunta, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) causes Coronavirus Disease 2019 (COVID-19), which has been affecting worldwide health since December 2019 1. The epidemic has afflicted 223 countries worldwide 2 with a total of 11, 549,072 confirmed cases and 3,756,185 life losses documented in Africa till March 02, 2022 3. The first verified case of COVID-19 in Ethiopia was announced on March 13, 20204. As of March 2, 2022, a total of 468,786 confirmed COVID-19 cases and 7,486 deaths had been reported3. Ethiopia has undertaken a variety of preventive measures to reduce the frequency and mortality rate of COVID-19 infection 5, 6. Despite the actions taken throughout the world, the impact of the pandemic is not meaningfully controlled 7. The health and financial burden of COVID-19 provoked the necessity for suitable and actual vaccine development 8. Hence, vaccination was considered as the paramount approach for halting the transmission of the infection 7.
In May 2020, the 73rd World Health Assembly delivered a resolution identifying the role of wide-ranging immunization as a global public-health goal for stopping, containing, and halting transmission of SARS-CoV-2. The vaccine has been shown to reduce infections even among individuals who are not vaccinated, through the development of herd immunity, if most of the population become vaccinated 9.
Ethiopia has planned to vaccinate about 20% of the population until the end of 2021 being high priority was given to health care professionals, elderly and patients with chronic disease above the age of 55 years old 10.
Even if every segment of population is likely to be affected by COVID-19 infection, patients with co-morbidities like hypertension, obesity and diabetes are mainly at increased risk of complicating outcomes compared to those without 11, 12, 13. The adverse effect of COVID-19 infection among people living with HIV was controversial 14, 15, 16, 17, 18, 19. HIV causes immunosuppression by depleting CD4 cells, thus reducing the capacity of the body to defend against bacterial, fungal, parasitic, and viral infections such as COVID-19 20. This vulnerability to infection is greater when the immunosuppression is severe and the patient is not on ART making the patient at risk of opportunistic infections 21, 22. The result of meta-analysis on mortality rate of people with HIV due to COVID-19 was 8.87 The existence of 1,034,640 HIV positive people in Ethiopia during this time period poses a challenge to health-care systems, necessitating vigorous preventive and treatment interventions 23. COVID-19 immunization, one of the preventative methods, produced the same level of immune response as well as no difference in adverse effects in people with HIV and people without HIV 24. As a result, it is required for programmatic objectives, optimal allocation of vaccine availability, and prioritizing of care for HIV-positive persons. The purpose of this study was to determine whether or not patients living with HIV were willing to receive the COVID-19 vaccine.
Method
Study setting and sample size
A facility-based cross-sectional study was conducted from February 15 to March 15, 2022, in Woldia comprehensive specialized hospital located in Northern Ethiopia.
Sample size and sampling technique
The sample size was calculated using a single population proportion formula, taking into account the prevalence of readiness to accept COVD-19 vaccine among persons living with HIV in Butajira, which was 59.4 percent, with a margin of error (d) of 0.05 and a 95 percent confidence range. A consecutive sampling technique was employed to recruit study participants.
Populations of the Study
The source population of the study was all people living with HIV who had visited Woldia Comprehensive Specialized Hospital ART clinic, whereas the study population was all people living with HIV on ART who had visited Woldia Comprehensive Specialized Hospital during the data collection time.
Eligibility Criteria
People living with HIV and who were under the age of 18 and those who were unable to respond owing to a severe illness were excluded from the study.
Operational definition
COVID-19 vaccine acceptance respondents who scored 1 were thought of as having willingness to accept the COVID-19 vaccine, and respondents who scored 0 were thought of as having no intention to accept the COVID-19 vaccine 25.
Good knowledge towards the COVID-19 vaccine (Respondents who scored 70% and above of knowledge questions)
Poor knowledge towards the COVID-19 vaccine (Respondents who scored less than 70% of knowledge questions)
Positive attitude towards the COVID-19 vaccine (Respondents who score greater than or equal to 70% of attitude questions)
Negative attitude towards the COVID-19 vaccine (Respondents less than 70% of attitude questions) 25.
Data Collection Procedures and quality control
The information was gathered using a pre-tested structured questionnaire based from various published articles. To maintain uniformity, the questionnaire was written in English, translated into the local language (Amharic), and then re-translated back into English. Data collectors and supervisors were trained on the purpose of the study, the clarity of the measurement tool, and ethical considerations. Three BSc nurses collected the data, and one supervisor oversaw the entire operation. A daily meeting and monitoring were also established in order to analyze difficulties that arose during data gathering.
Data processing and Analysis
Epi data 4.4.3 and IBM SPSS 25 software were used to enter the data. The variable was summarized using a descriptive summary (frequency distribution, proportion, mean, and standard deviation). To study factors related with vaccine acceptance, a binary logistic regression model was used. Variables having a p value of 0.25 in the bivariate analysis were incorporated into the multivariable analysis to compensate for potential confounder effects. To declare statistical significance, a P value of less than 0.05 was employed.
Ethical approval
Ethical approval was obtained from Woldia university ethical review committee. Permission letter was obtained from woldia comprehensive specialized hospital medical director office. Informed consent was obtained from the study participants. Confidentiality of patients’ information was kept anonymous in any process of the study.
Result
Socio-Demographic Characteristics of the Respondent
A total of 332 HIV-positive patients on ART participated, with a response rate of 89.5%. The respondent’s age range was 18–57 years. Out of 332 study participants, 61.4% were female (Table 1). The mean monthly income of the study participants was 2696.95 Birr. The minimum and maximum duration of diseases among the study participants was 1 year and 17 years respectively, with mean of 8.45 years.
Table 1. Socio-demographic related characteristics of PLWHA on ART in Woldia comprehensive specialized hospital.| Variables | Willingness to accept vaccine | Total (%) | ||
| Yes (%) | No (%) | |||
| Sex | Male | 79(23.79) | 49(14.76) | 128(38.55) |
| Female | 141(42.47) | 63(18.97) | 204(61.44) | |
| Religion | Orthodox | 138(41.56) | 71(21.38) | 209(62.95) |
| Muslim | 60(18.07) | 31(9.33) | 91(27.41) | |
| Protestant | 17(5.12) | 10(3.01) | 27(8.13) | |
| Other | 5(1.50) | 0(0) | 51.50) | |
| Marital status | Married | 37(11.14) | 8(2.41) | 45(13.55) |
| Single | 118(35.54) | 35(10.54) | 153(46.08) | |
| Widowed | 46(13.85) | 44(13.25) | 90(27.11) | |
| Divorced | 19(5.72) | 25(7.53) | 44(13.25) | |
| Educational status | Illiterate | 56(16.87) | 66(19.88) | 122(36.75) |
| in-formal | 24(7.23) | 28(8.43) | 52(15.66) | |
| Primary | 66(19.88) | 9(2.71) | 75(22.59) | |
| Secondary | 64(19.28) | 4(1.2) | 68(20.48) | |
| College and above | 10(3.01) | 5(1.5) | 15(4.52) | |
| Residence | Urban | 177(53.31) | 38(11.44) | 215(64.76) |
| Rural | 43(12.95) | 74(22.29) | 117(35.24) | |
| Occupation | House maid | 51(15.36) | 11(3.31) | 62(18.67) |
| Farmer | 66(19.88) | 36(10.84) | 102(30.72) | |
| Private | 78(23.49) | 51(15.36) | 129(38.85) | |
| Government employee | 15(4.52) | 12(3.61) | 27(8.13) | |
| Unemployed | 10(3.01) | 2(0.6) | 12(3.61) | |
COVID-19 related characteristics
One hundred and ten (33.1%) and 118(35.5%) of the study participants had poor knowledge and negative attitude about COVID-19 vaccine respectively while 31(9.3%) of the study participants perceive ART drugs can also prevent COVID-19 infection. Twenty-seven (8.1%) participants perceive COVID-19 vaccination had negative impact on HIV/AIDS progress (Table 2).
Table 2. COVID-19 related characteristics among PLWHA on ART in Woldia comprehensive specialized hospital.| Variables | Frequency | Percentage | |
| Can ART drug prevents COVID-19 | Yes | 31 | 9.3 |
| No | 301 | 90.7 | |
| COVID-19 vaccine has negative impact on diseases progress | Yes | 27 | 8.1 |
| No | 305 | 91.9 | |
| COVID-19 vaccine has negative interaction to ART drugs | Yes | 12 | 3.6 |
| No | 320 | 96.4 | |
| Any family member who get infected by COVID-19 | Yes | 81 | 24.4 |
| No | 246 | 74.1 | |
| Susceptibility to COVID-19 infection | Yes | 129 | 38.9 |
| No | 203 | 61.1 | |
| Knowledge about COVID-19 | Poor | 110 | 33.1 |
| Good | 222 | 66.9 | |
| Attitude towards COVID-19 | Negative | 118 | 35.5 |
| Positive | 214 | 64.5 | |
Two hundred and seven study participants got COVID-19 vaccine related information’s from health care workers, out of them about 85 study participants had willingness to accept COVID-19 vaccination (Figure 1).
Figure 1. Source of information about COVID-19 vaccination among PLWHA on ART in Woldia comprehensive specialized hospital.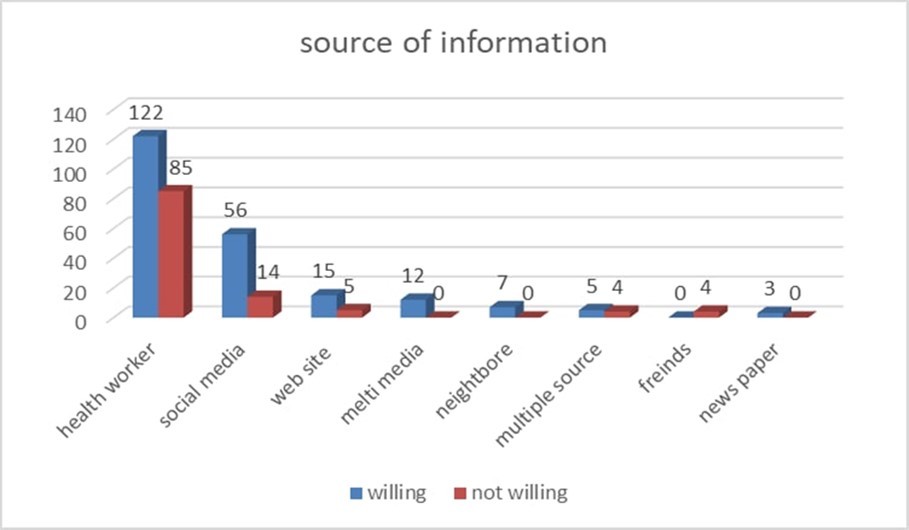
Willingness to receive COVID-19 vaccination and associated factors among people living with HIV/AIDS
Two hundred and twenty (66.3%) with 95% CI (60.9, 71.5) study participants were willing to take COVID-19 vaccination. Out of this, 141(64.1%), 177 (80.4%) and 78(35.4%) were female, urban resident and private worker. (Table 3)
Table 3. Factors associated with COVID-19 vaccination acceptance among PLWHA on ART in Woldia comprehensive specialized hospital.| Variables | No. (%) | COR(95% CI) | AOR(95% CI) | p-value | |
| Marital status | Married | 37(11.14) | Ref | - | |
| Single | 118(35.54) | 0.16(0.06,0.43) | 0.34(0.07,1.66) | 0.18 | |
| Widowed | 46(13.85) | 0.22(0.11,0.46) | 0.2(0.06,0.62) | 0.005 | |
| Divorced | 19(5.72) | 0.73(0.35,1.5) | 2.24(0.55,9.03) | 0.26 | |
| Educational status | Illiterate | 56(16.87) | Ref | - | |
| In-formal | 24(7.23) | 2.36(0.76,7.3) | 0.68(0.12,3.7) | 0.652 | |
| Primary | 66(19.88) | 2.333(0.7,7.78) | 2.94(0.42,20.68) | 0.277 | |
| Secondary | 64(19.28) | 0.273(0.07,0.98) | 0.13(0.02,0.88) | 0.036 | |
| College and above | 10(3.01) | 0125(0.03,0.55) | 0.07(0.009,0.62) | 0.017 | |
| Residency | Urban | 177(53.31) | Ref | ||
| Rural | 43(12.95) | 0.12(0.07,0.21) | 0.12(0.05,0.32) | 0.000 | |
| Knowledge | Poor | 110(33.1) | Ref | ||
| Good | 222(66.9) | 2.73(1.69,4.4) | 3.74(1.5,9.36) | 0.005 | |
| Attitude | Negative | 118(35.5) | Ref | ||
| Positive | 214(64.5) | 2.55(1.59,4.09) | 4.34(1.6,11.79) | 0.004 | |
| Monthly income (Mean±SD) | 2696.95±2353.00 | 1.00(1.00,1.00) | 1.00(1.00,1.01) | 0.007 | |
| Duration of ART (Mean±SD) | 8.45±4.16 | 0.86(0.81,0.91) | 0.80(0.71,0.90) | 0.000 | |
In multivariable analysis, refusal to be vaccinated for COVID-19 vaccine was significantly associated with poor knowledge (AOR: 2.73; 95% CI (1.69, 4.4)) and negative attitude (AOR: 2.55; 95% CI (1.59, 4.09)) compared with their counters. PLWHA on ART who live in rural area were less likely (AOR: 0.12, 95% CI (0.07, 0.21) willing to be vaccinated compared to those who live in urban area.
Discussion
Vaccination is an important approach for mitigating the COVID-19 pandemic by instilling herd immunity in the community. The effectiveness of this technique is dependent on vaccine uptake in the population. According to the most recent COVID-19 estimates, up to 60–75 percent of the population needs to be vaccinated in order to stop the disease's spread and achieve herd immunity 26.
The established risk factors for COVID-19 acquisition and consequences, such as heart disease, kidney disease, diabetes, chronic pulmonary disease, and obesity, may be more prevalent in PLWHA 27. Existing clinical data suggest that the risk of acquiring deadly COVID-19 in PLWHA was 30% higher than in those without HIV infection. All currently available vaccinations can be used safely in patients living with HIV, independent of CD4 count or viral load suppression status 28.
The prevalence and parameters associated with PLWHA's willingness to receive COVID-19 immunization were investigated in this study. As a result, 66% of PLWHA expressed desire to get the COVID-19 vaccine. This study's findings agree with those of an Ethiopian study (62.6%) 25. Reports of willingness to receive COVID-19 vaccine among PLWHA in current study was higher than findings from study in Turkey (29.2%) 29, Ethiopia (31.4%)30 and Palestine (37.8%)31, Wolayta-Ethiopia (45.5%)32, Southern Ethiopia (46.1%)33, China (57.2%)34 and south India (60%)35. And the finding of this study is lower than findings from, China (72.5)36, France (71.3%)37. This disparity could be explained by geographical heterogeneity, the methodology used, and the socio-demographic and socioeconomic features of the research populations.
The novelty of the COVID-19 disease may have contributed to the lower magnitude of vaccine adoption. As a result of the vaccine's rapid development, there may be ambiguity and misguided ideas about it, which leads to the false notion that the vaccine has not been sufficiently proven for safety and effectiveness, as well as restricted access to information, particularly in LMICs38. Furthermore, this increased vaccine hesitation could be linked to widespread misinformation about the COVID-19 vaccine on social media39. Despite the increased risk of developing COVID-19, the low rate of vaccination uptake in PLWHA provides fertile ground for exacerbating health-related side effects 40.
In our study, PLWHA with secondary and college education levels were less likely to be willing to be vaccinated with COVID 19 vaccine than non-educated participants. This is confirmed by studies from Gondar, Ethiopia, which found that participants with a university degree were less likely to receive the vaccine than those with a college diploma 10. In contrary, this study was not in-line with findings from41, (Palestine)31, USA42 which reported willingness of receiving vaccine increases as educational status of an individual increases. This might be due increased concerns about the mistrust in efficacy and efficiency of the vaccine 35. In addition, for HIV infected individuals, they may worry that the vaccine would further worsen their immune system 43.
Negative claims about vaccine effectiveness can profoundly influence vaccine uptake 44. Rumors regarding vaccination efforts being utilized for political goals, assertions that the COVID-19 vaccine was designed to reduce the global population, affect vaccination campaigns in various nations, particularly among the educated portion of the public who likely have better access to information. The odds of a participant being classified as hesitant increased by 26% for each additional source of information they mistrusted 35, 45. In this situation, stakeholders such as the federal ministry of health, the regional health bureau, and media organizations should broadcast reliable information to the population, thereby developing confidence, ensuring widespread vaccine coverage, and ultimately ending the pandemic.
In present study, participants who had good knowledge towards COVID-19 vaccine were 3.7 more likely to accept the COVID-19 vaccine when compared to respondents with poor knowledge. This was consistent with the findings from Ethiopia46, Ethiopia47, Pakistan31, Ethiopia 25, and the USA48.It might be due to having good knowledge about a COVID-19 vaccine being a prerequisite for using it.
Respondents who had a positive attitude towards the COVID-19 vaccines had a significantly higher acceptance rate of the COVID-19 vaccine (AOR=4.3) which was supported by the findings from Ethiopia47, Ethiopia46, Ethiopia49, South Africa50, Ethiopia33 worldwide51. This could be due to those who have positive attitude towards the vaccine are highly compliant towards preventive measures against the pandemic including vaccination. Therefore, information campaigns should focus on providing more information about COVID-19 vaccine safety, reassuring the population in order to maintain this positive attitude towards the intention to accept the vaccine.
Even though this study had strengths, there were some limitations. This study was cross sectional survey. Therefore the limitation of this study is temporal relationship can’t be determined. The other limitation is lack of control group (HIV negative persons)
Conclusion
Almost one-third of PLWHA on ART refused immunization. This study demonstrates the complexities of patients' imaginations regarding COVID-19 immunization and may aid physicians and other health care providers in understanding patients' perspectives on COVID-19 vaccination. Increased sensitization on the necessity of vaccines and the negative consequences of diseases, particularly among PLWHA, should be considered in the development of the COVID-19 vaccination campaign by prominent individuals such as health professionals and religious figures. Vaccination programs should be culturally appropriate and informed by people who have lived experiences in order to reach people who might otherwise be hesitant. Furthermore, the need of immunization and the negative implications of refusing the vaccine must be thoroughly explained.
Acknowledgment
Our heart full gratitude goes to the study participants and health care professionals working in Woldia comprehensive specialized hospital for their good face to conduct this work.
List of abbreviations
ART: Anti-retroviral Drug
COVID-19: Coronavirus disease 2019
HIV/AIDS: Human Immunodeficiency Virus / Acquired Immunodeficiency Syndromes
PLWHA: People living with HIV/AIDS
Declarations
Availability of data and Materials
The data set used and analyzed for the study is available from the corresponding author on reasonable request.
Funding
No funds were available to conduct this study.
Consent for publication
Not applicable.
Authors’ Contributions
AT conceptualized and designed the study, conducted data entry, cleaning and analysis, and drafted the manuscript. MS reviewed the study design and methodology, conducted data entry, cleaning and analysis, and reviewed the manuscript for substantial intellectual content. WK drafted the manuscript and reviewed the manuscript for substantial intellectual content. HM supervised the data collection process and critically reviewed the manuscript for substantial intellectual content finally authors read and approved the final manuscript.