Abstract
Right atrial thrombi are a remarkable phenomenon especially when witnessed live on the monitor during echocardiographic study. They represent a clot en passant caught in the middle of travel to final destination in the pulmonary vasculature. In this paper we present two cases that show us the ambivalent nature of these clots, the challenges faced during their management and the possible outcome for the patient. The first case with fatal outcome is narrated in present tense because the outcome is fatal and the second is narrated in past tense because the patient survived and the clot became a past incidental encounter
Author Contributions
Academic Editor: Thawatchai Akaraviputh, Faculty of Medicine Siriraj Hospital, Mahidol University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Mukhamad Sami Valid, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Right heart thrombi in the absence of structural heart disease, atrial fibrillation or catheter located in the heart are rare and usually represent a traveling clot from the venous system to the lung, known as right heart thrombi-in-transit. These are different from thrombi that can develop on pacemaker wires 1. They may be detected incidentally on routine echocardiogram with normal sinus rhythm and normal right ventricular (RV) function 2. Asymptomatic clots that move into pulmonary vasculature without undermining the hemodynamic status of the patient have been reported 3. In other cases, the patient may destabilize rapidly with massive pulmonary embolism leading to death 4, 5. Thrombolytic therapy or operative thrombectomy can be considered in patients with these clots 5, 6.
Based on the European Working Group on Echocardiography (1989) definition three patterns of right heart thrombi are named 7. Type A thrombi are highly mobile, serpiginous, arise from deep vein thrombosis and most often lead to pulmonary embolism (thrombi-in-transit). Type B thrombi are nonmobile, form in situ in association with underlying cardiac abnormalities. Type C thrombi are very rare, highly mobile and share a similar appearance to a myxoma.
Case 1
73 year old male, African-American is brought to the emergency room accompanied by his wife because of shortness of breath worsening over the last week especially on exertion. The patient has history of hypertension, coronary artery disease, congestive heart failure, gout and alcohol abuse. Electrocardiograph shows sinus tachycardia at 102 beats per minute without ST segment changes. Chest x-ray shows cardiomegaly without evidence of pulmonary vascular congestion, infiltrates or pleural effusions. Laboratory analyses show white blood cell count of 6,000, hemoglobin 12.8, hematocrit 39, platelets 314,000, INR 1.26, glucose 105, BUN 25, creatinine 1.5, sodium 134, potassium 4.6, chloride 100, CO2 22, Ca 8.4, total protein 7.4, albumin 3.1, aspartate aminotransferase (AST) 103, alkaline phosphatase 93, total bilirubin 1.4, alanine aminotransferase (ALT) 62, CK-MB 1.1, cardiac troponin I (CTNI) 0.02, naturietic peptide type B 3969, and normal cholesterol, triglycerides and high and low density lipoprotein.
Echocardiogram shows: 1. Severely decreased LV ejection fraction. 2. Large, mobile thrombus in the right atrial cavity (Figure 1). 3. Moderately dilated right atrium. 4. Mild aortic regurgitation. 5. Mild concentric left ventricular hypertrophy. 6. The left ventricular size is mild to moderately increased. 7. Mild thickening of the anterior and posterior mitral valve leaflets. 8. Ischemic cardiomyopathy. 9. Mild aortic valve sclerosis without stenosis. 10. Mild mitral valve regurgitation. 11. Mildly elevated pulmonary artery systolic pressure. 12. Moderately enlarged right ventricle. 13. Moderately reduced RV systolic function.
Figure 1. Echographic image of Case 1 of the large, mobile thrombus in the right atrial cavity.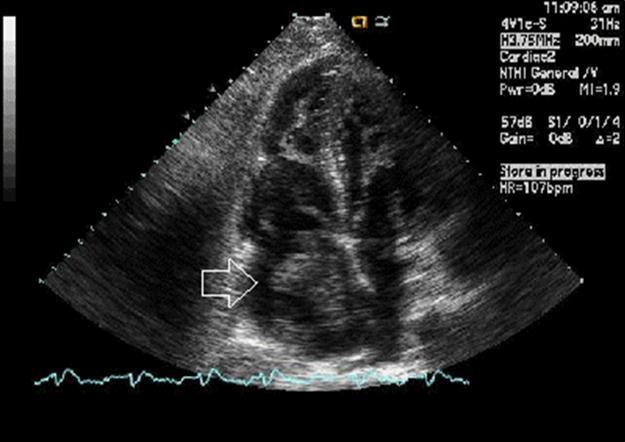
Arterial blood gas testing shows pH 7.47, pCO2 27, pO2 93, bicarbonate 19.7, total CO2 20.5, base deficit 2.7, oxygen saturation 98% at FiO2 40% nasal cannula. After two days the patient develops atrial fibrillation at 174 beats per minute. After discussion with the cardiologist and intensivist, thrombolysis therapy is considered. The risks and benefits of thrombolysis are explained to the patient and his wife and they consent for the treatment. Aspirin and heparin drip are stopped and the coagulation values before initiation of thrombolysis are PT 15.3, INR 1.45 and PTT 32. Alteplase (tPA) 100 mg in 100 ml solution is to run in 2 hours. Thus, tPA is initiated with a bolus then an infusion. The patient deteriorates and codes after an hour and 45 minutes, 15 minutes before the end of the tPA infusion. Resuscitation efforts are unsuccessful and patient unfortunately expires.
Case 2
87 year old female from nursing home was admitted to Coronary Care Unit (CCU) because of atrial fibrillation with rapid ventricular rate. Heart rate was controlled with digoxin and metoprolol and continued on warfarin. Echocardiogram showed a highly mobile right atrial thrombus (Figure 2), left ventricular ejection fraction 40-45%. Six days later, echo and magnetic resonance imaging (MRI) did not show the thrombus; however, CT of the chest showed emboli in the pulmonary arterial branches of the right middle and right lower lobes. Venous duplex showed acute deep venous thrombosis in the right leg. No ABG was done. Blood analyses showed glucose 99, BUN/Cr 15/0.5, Na 137, K 3.4, Ci 107, bicarbonate 24, Ca 8.4, albumin 2.2, three sets of cardiac enzymes (CKMB & CTNI) within normal limits, WBC 7.6, hemoglobin 9.2, hematocrit 27, platelets 134, fecal occult blood negative. Inferior vena cava (IVC) filter was placed under fluoroscopic guidance before discharging the patient on digoxin and warfarin.
Figure 2. Echographic image of Case 2 of the large, mobile thrombus in the right atrial cavity.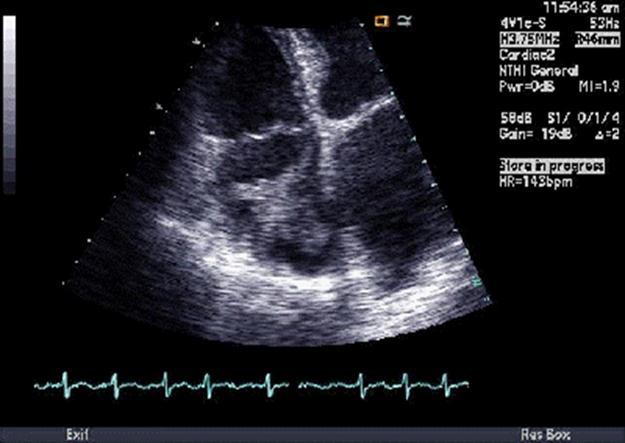
Here, we present 2 cases of large right atrial thrombus with 2 different outcomes. This entity should be born in mind when encountering high risk patients. Thrombolysis or surgical intervention may or may be lifesaving and each case should be considered individually.