Abstract
Patients suffering treatment resistant Parkinson´s disease (PD) are potential candidates for deep brain stimulation (DBS). Commonly most implanted electrodes have a cylindrical shape with quadripolar electrode contacts and generate a symmetrical stimulation field around the lead. To reduce side effects through activation of neighboring fibers a new electrode design with segmented contacts was developed and enables a better adaption of the field of stimulation as well as a multi-target stimulation to improve therapeutic benefits.
We report about a 51-year-old male patient with a 15-year history of treatment-refractory PD, who was implanted with bilateral segmented electrodes in the subthalamic nucleus (STN) with St. Jude Medical Infinity™ DBS System (Abbott/St. Jude Medical, Saint Paul, Minnesota, USA). Despite a clear mood-enhancing effect, stimulation with ring electrodes caused motor side effects including rigor and speech disorder. With segmented electrodes an effective and gentle stimulation was achieved. The stimulation of the anterior segments in the central position of the electrode in the STN showed no side-effects and allowed a reduction of initial symptoms in an low stimulation amplitude.
Despite precise preoperatively planning and intraoperative trial stimulation, side effects of STN stimulation are very common. The application of segmented electrodes permits more options to reduce side effects rather than using ring electrodes. Studies with larger sample sizes are needed to establish the optional DBS electrode.
Author Contributions
Academic Editor: Esra Dogru Huzmeli, Mustafa Kemal University School of Physical Therapy And Rehabilitation, Turkey.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright 2019 Frank P. Schwarm, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Deep brain stimulation (DBS) is a reversible neuromodulative “last-resort option” for medically refractory Parkinson’s disease (PD) in order to control movement problems and essential tremor1,2,3. The subthalamic nucleus (STN) and globus pallidus pars interna (GPi) are well accepted targets in the therapy of PD. STN stimulation is seen superior to GPi for medication reduction 4. DBS permits focal adjustment of the STN, which resulted only in 41% reduction of initial symptoms in all patients and caused more side effects5. The percentage of responders with long-term reduction of their symptoms varies from 10-61.5%6,7.
The discrepancy in the results may be at least partially related to the differences in anatomical targeting, the stimulation protocol, and electrode design8.
Most implanted electrodes have a cylindrical shape with quadripolar electrode contacts and generate a symmetrical stimulation field 9. To reduce side effects through activation of neighboring fibers, a new electrode design with segmented contacts was developed which enables a better adaption of the field of stimulation as well as multi-target stimulation 10,11,12. Promising stimulation effects, a reduction of side effects, an improvement of the postoperative management, and the possibility to widen the therapeutic window were shown in the last few years 13,14,15,16,17.
Here, we report our first clinical experience of directional DBS with the fully implantable segmented DBS system (Abbott/St. Jude Medical, Saint Paul, Minnesota, USA) for STN stimulation in PD.
Clinical Presentation
History and Examination
A 51-year-old male presented with a 15-year history of medication-refractory, tremor predominant PD and an impulse control disorders (ICD) under dopamine agonist therapy.
Initial diagnosis was made in 2011 clinically and with DaTSCAN. Initial clinical symptoms occured in 2002 showing lower extremity rigor. Daily activities and work as a heart surgeon had not been severely affected at this time. In 2013 the patient developed an ICD with pathological gambling and compulsive shopping under dopamin agonist therapy. An optimization of the medical therapy was conducted. Because of motor fluctuations under L-dopa therapy, an apomorphin therapy was started. In 2015 an acute deterioration was seen with worsening of rigor and tremor. Further the patient developted a difficulty in speaking. There was distinct rigidity, bradykinesia, and akinesia. After discussing treatment options, interdisciplinary decision was made to perform STN DBS. Patient’s informed consent was obtained.
Surgery
MRI sequences with T1- and T2-FLAIR-weighted scans as well as a CT navigation scan were performed. BrainLab’s iPlan Stereotaxy 3.0 software (BrainLAB Inc., Feldkirchen, Germany) was used to target STN bilaterally. Prior the CT-investigation, the stereotactic head ring was applied. After aquisition and fusion of MRI and CT scans STN was measured in relation to the anterior commissure/ posterior commissure (AC-PC) line. Final coordinates in X-, Y-, Z-directions were calculated. The prior calculated coordinates of the electrode were applied to the stereotactic ZD frame (Inomed, Emmendingen, Germany). After applying the coordinates to the stereotactic verification phantom, accurate needle positioning was ensured. The stereotactic frame was applied to the patient. Burr hole craniotomy was done under local anesthesia and sedation with dexmedetomidine (Dexdor®, Orion Corporation, Espoo, Finland).
Microelectrode mapping was done with three electrodes. Test stimulation was performed to verify correct placement and define the therapeutic window (TW). Once desired position depth was reached at the central part of the STN, the stylets were replaced with segmented DBS electrodes The right STN stimulation was started at -5mm from the target point. At -4mm anterior and central a sufficient stimulation effect was seen. Sufficient stimulation could be continued till +1.5mm. At the target point sufficient stimulation was seen in all three microelectrodes. A sufficient reduction of rigor and tremor in the neurological examination was seen with 2mA. The segmented electrode tip (2 and 3), (Figure 1) was positioned at +1.5mm over the target point.
Figure 1. This model shows the segmented electrode with its segmented middle segments and multiple, activatable contact panels for adjusted stimulation.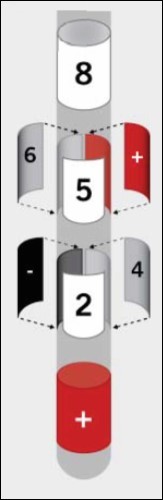
Microelectrode mapping at the left STN was performed in the exact same manner. The segmented electrode tip was positioned at +1 mm over the target point. The anterior electrode showed the best effect with an immediate improvement of tremor and dysdiadochokinesia at both sides. Once all segments around the circumference of the lead were simultaneously activated, stimulation was less effective. For intraopertive imaging, fluoroscopy was used. After bilateral implantation, connection to a subclavicular 2-channel pulse generator was done.
Postoperative Course
The procedure was performed without any complications. Postoperative cranial CT imaging revealed proper placement of both electrodes in the central part of STN (Figure 2). After fusion with the preoperative stereotactic plan, both electrodes were seen in the correct position of the STN (Figure 2). Electrodes were postoperatively activated bilaterally for continous stimulation with the wireless iOS mobile programming platform (Table 1). The patient experienced strong improvement of bradykinesia and rigidity under stimulation of the anterior segmented electrode (130Hz, 0.5mA). He was able to speak and walk without any problems. The apomorphin medication was stopped. L-dopa medication was reduced. Simultaneous activation of all segments around the circumference of the electrode caused the patient to suffer dysarthria and motor symptoms.
Figure 2. Pre- and postoperative computertomography merge showing tips of electrodes fused to bilateral trajectories of planned STNDBS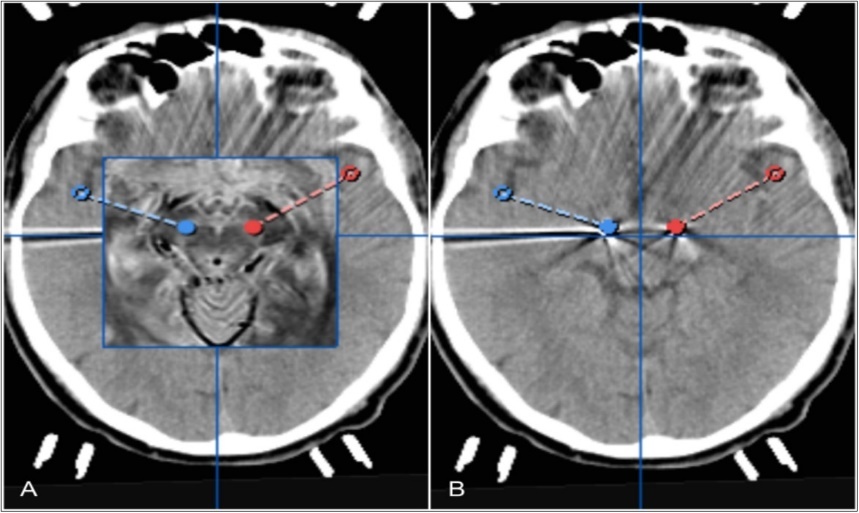
| left STN | right STN | |
| electrode type | Infinity 1-3-3-1 (1.27 x 0.5 mm) | Infinity 1-3-3-1 (1.27 x 0.5 mm) |
| amplitude | 1.0 mA | 0.9 mA |
| pulse width | 60 μs | 60 μs |
| frequency | 110 Hz | 130 Hz |
Discussion
Deep brain stimulation is an effective and reversible form of PD treatment1,2,3. This case illustrates that segmented electrodes can reduce most side effects because of individual circumferential stimulation of middle segments. This innovative and effective form of DBS allows optimization of the stimulation even though the electrode is optimal localized
Our first experience with segmented electrodes for DBS showed postoperatively a nearly complete regression of the motor symptoms without any side-effects.
Due to multiple, activatable contact panels of the segmented electrode it is possible to create a volume of tissue activated in different direction and expansion. Side effects thus could be reduced especially if the electrode is not optimally positioned or the patient developed side effects after stimulation18. Due to sufficient reduction of rigor and tremor in the reported case with low amplitude also power consumption is reduced12,19,20,16,21. Zhang et al. described enormous patient expectations and individual differences as the most important reasons for stimulation malfunction and a not satisfactory conventional stimulation in PD patients. DBS can not alleviate all of PD symptoms, only the apparent symptoms are treated and with the conventional stimulation good covered18. Further the size and anatomical position of STN and maybe unsatisfactory electrode position could play an important role for insufficient stimulation18. The circular contact of the electrode could also affect other nearby structurs during circular stimulation18.
Dysarthria as a DBS side effect, which is caused due to STN stimulation on the left side and could be reduced using bipolar stimulation with interleaving and low frequenzy stimulation 18,22. As our case demonstrated, segmented electrodes could lead to a reduction of dysarthria as well.
To reduce the side effects with convential electrodes Ramirez-Zamora et al. used to alleviate stimulation of STN, which induced choreoathetoid dyskinesia and incomplete Parkinson disease control22. This finding reasons the use of segmented electrodes in the case of our patient.
Further the wireless iOS mobile programming platform enables an easy and non-invasive therapy optimation. An improvement of the quality of life could be achieved.
Limitations of our case report are the lack of long-term clinical follow-up data, and the early postoperative time period.
Conclusions
We showed advantages and feasibility of using a fully implantable neurostimulation device with segmented electrodes. Despite precise preoperative planning and intraoperative trial stimulation, side effects of STN stimulation are common and may be reduced by segmented stimulation. Well-controlled studies with larger samples sizes are needed to establish this optional DBS electrode.