Abstract
Pharmacodynamic modeling of sunscreens was performed using a new concept of Skin UV Index (SUI) on the exposed skin as a parameter to evaluate the potential effectiveness of sunscreens against sun damage. The SUI predicts the UV heat intensity on the skin surface in terms of the solar UV Index at the time of the study and is calculated by solar UV Index/sunscreen’s SPF. SUI numbers for sunscreen with SPF ranging from 2 to 100 under a solar UV Index of 10 was used for illustration. Based on guidelines from WHO, Australia and New Zealand, sunscreens yielding SUI < 3 are assumed to be effective against sun damage such as sunburn and melanoma. Based on the above assumption, sunscreens with SPF > 4 were found to be effective when sunscreens were evenly applied at 2 mg/cm2. Review of numerous studies suggests that missing applications may represent a major, seemingly unavoidable, SPF-independent factor causing unintended sunburns for sunbathers in the US and other countries with a temperate climate. This might in turn become a major factor for causing exponential increase in melanoma incidence rates observed in the last few decades. For example, in an SPF 30 sunscreen study all 25 participants suffered unintended sunburns after one week of sunbathing. Also, a mean missing application of 20% of the total exposed area and a mean missing of about 50% of the time were reported in two separate studies. Simulations were also performed with under-applications of 50% and 75%. The present simulations may provide a rationale of why routine use of a low SPF 8 sunscreen was reported to be effective against melanoma in a 2018 Australian study. Based on model simulations it is proposed that in the US, SPF 8 sunscreen and SPF 2 to 6 sunscreen may be adequate for routine, unintentional use for sun-sensitive populations and non-sun-sensitive populations, respectively.
Author Contributions
Academic Editor: Bayat A, Department of Perioperative Medicine, Clinical Center, National Institutes of Health, USA.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Win L. Chiou
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
Winlind Skincare LLC : As president of this practically one-person (WLC), residence-based family company
Citation:
Introduction
Apparently based on a sun avoidance policy, broad-spectrum sunscreens have been recommended in the United States (US) as an adjunct to help prevent sunburns, skin cancers and premature aging (i.e., photoaging) for persons older than 6 months, even on cloudy days 1. In view of reports that daily exposure to mild or moderate sunlight may not have noticeable long-term adverse effects on skin aging 2, skin aging may be mainly caused by the intrinsic nutritional factor 2, and such an exposure may also provide numerous potentially important health benefits 3, 4, 5, 6, 7, Chiou 8 recently suggested that in our daily lives we may not need to use sunscreen and other sun protection methods, such as seeking shade, wearing long-sleeved shirts, long pants and broad-brimmed hats unless one is to be exposed to potentially sunburn-causing sunlight. In this regard it is of interest to note that subtropical Australia and New Zealand, with the highest melanoma incidence rates in the world, are probably the only two countries to date to adopt the World Health Organization (WHO) guidelines on a sun protection program that recommend use of sunscreens only when the solar UV Index is ≥ 3 8, 9, 10. It appears that the clinical justification of this one-size-fits-all recommendation has not been fully discussed.
Sunscreen products with SPF numbers ≥ 15 1 are currently required for marketing in the US. This was apparently based on an earlier Australian clinical study 11 showing that regular use of sunscreens with SPF numbers ≥ 15 resulted in better protection against melanoma, the most lethal form of skin cancer, than the uncontrolled use of products with SPF numbers < 15. The potential shortcomings of this study, including lack of statistical significance 4, 12, difference in use pattern 12, 13 between the US (mainly for intentional, intermittent sun exposure) and Australia (mainly for regular, non-intentional sun exposure), as well as inconsistencies in site 14 between sunscreen application (only to the face and upper extremities) and melanoma-occurring sites (over the whole body), have been discussed. It was reported that for the efficacy evaluation of sunscreens, the gold standard of double-blind, randomly controlled clinical studies cannot be carried out because of ethical concerns 4. Obviously, high rarity and the time period (years) to form visible melanoma may also be problematic 14. Interestingly the SPF 15 sunscreen was found to be ineffective in reducing melanoma in a 2016 population-based cohort study in Norway 13. On the other hand, SPF 8 sunscreen was reported to be effective against melanoma in Australia in a 2018 study 15. It appears that to date potential reasons of the apparent difference in conclusion between these two studies 13, 15 have not been considered. In a highly respected commentary published in 2019 14, it was stated that “The effect of sunscreen on melanoma prevention is also unclear “.
To date, results of meta-analyses 16, 17, 18 have often shown no association between sunscreen use and the expected protection against melanoma. Paradoxically, sunscreens have been frequently reported or suspected to cause more sunburns and/or melanomas 4. 16. Various reasons 14, 19, 20, 21, 22, 23, 24, 25, 26, 27 such as a false feeling of security, under-applications by about 50% to 75%, uneven application, lack of reapplication, missing applications, prolonged sun exposure, low SPF strengths (such as below 15], and skin sensitivity have been postulated to account for observed therapeutic failures or increased incidences of sunburn and/or melanoma. In order to overcome the under-application and/or uneven-application problems, higher strengths of sunscreen have been introduced. Many sunscreens with SPFs ≥ 50 (regarded as high SPF) or 100 (regarded as very high SPF) from different manufacturers are now commercially available. There seems to be an emerging notion that the higher the SPF the better the protection against sun damage 28, 29, 30, 31. It appears that to date there are no theoretical pharmacodynamic modeling studies published to address the dose (in terms of SPF number)/effect relationship of sunscreens and to explore its potential significance. Understanding of such a relationship may provide valuable insights into potential limitations of current evaluation methods and into appropriate sunscreen doses in terms of SPF numbers that may be needed to achieve adequate sun protection. The present study attempts to achieve some of the above goals and hopes to stimulate further studies and debates on this important, complex and often controversial health subject.
Methods
Ultraviolet (UV) index , ranging from zero to 11+, is a quantitative measure of solar UV heat intensity 32 and the SPF is a measure of 1/fraction of UVB light unfiltered by the sunscreen when an amount of 2 mg/cm2 of sunscreen is evenly applied to human skin in a laboratory setting 1. In the present simul ation a solar UV Index of 10, considered to be a very high-intensity sunlight 32 that may occur, for example, between 10 am and 2 pm in the summer 33 of Los Angeles, is used for simulation. Theoretical relationships between use of sunscreens with SPF values ranging from 2 to 100 evenly applied to the skin at 2 mg/cm2, and the fraction (F) of sunlight unfiltered by each sunscreen ( estimated by 1/SPF), and the resulting sunlight intensity (Skin UV Index) in terms of UV Index reaching the skin (estimated by solar UV Index/SPF, or 10/SPF for the present simulation) were obtained. Because sunlight with a UV Index of 3 may be potentially harmful and requires sun protection measures 9, 10, therefore, it seems that in the present preliminary study one may use the estimated Skin UV Index (SUI) as a parameter to evaluate the efficacy of a sunscreen. If the calculated SUI is less than 3, then one may assume that the sunscreen is effective against sunburn and melanoma. On the other hand, if the calculated SUI is ≥ 3, then one may assume that the sunscreen used is ineffective against sunburn, melanoma and perhaps other types of skin damage. Simulations were also carried out using Beer’s law 34 when only 50% and 25% of the labeled amount were applied. The calculated SPF or experimentally determined SPF has been commonly referred to as Effective SPF 34. When only 50% of the labeled amount was applied, the Effective SPF was estimated by SPF½. When only 25% was applied, the Effective SPF was estimated by SPF1/334. When under-application occurs, the SUI can be calculated by solar UV Index/Effective SPF.
Results
Results of the above three preliminary simulations are shown in Figure 1, Figure 2, Figure 3 and their details are summarized in Supplements. Figure 1 indicates that when a sunscreen is applied in full compliance with the package instruction, namely, evenly at 2 mg per cm2 on all sun-exposed skin area, the resulting SUIs are all below 3 for sunscreens with SPF ≥ 4 when a person is exposed to very strong sunlight with a UV Index of 10. For the SPF 4 and 100 sunscreens only 25% and 1% of the incoming UVB rays are unfiltered or unblocked and their resulting SUIs are only 2.5 and 0.1, respectively. These apparently weak UV rays should be generally considered safe with minimum damage to the skin 8, 32 and minimum potential to cause sunburn and melanoma. As shown in Figure 2, when only 50% of the sunscreen is applied, the Effective SPFs of the two sunscreens will be reduced to 2 and 10, respectively, and their corresponding SUI values will decrease to 5 and 1, respectively. When only 25% is applied (Figure 3), the corresponding Effective SPF values become 1.4 and 3.2, a difference of only 2.3 folds compared toa difference of 25 folds in SPF (4 vs 100). Also, their corresponding SUI values are 7.1 and 3.1 with the same 2.3-fold difference.
Figure 1. Theorectical relationship between sunscreen SPF and estimated Skin UV Index when sunscreen is applied at 2 mg/cm2 and solar intensity is UV Index 10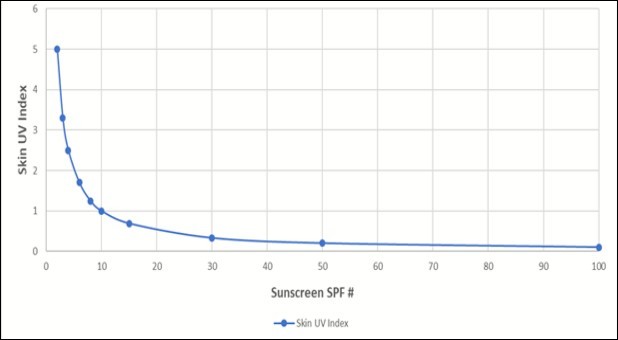
Figure 2. Theorectical relationship between sunscreen SPF, Effective SPF and estimated Skin UV Index when sunscreen is applied at 1 mg/cm2 and solar intensity is UV Index 10
Figure 3. Theorectical relationship between sunscreen SPF, Effective SPF and estimated Skin UV Index when sunscreen is applied at 0.5 mg/cm2 and solar intensity is UV Index 10
Discussion
Skin UV Index Concept
It appears that this may be the first study to date to use the concept of Skin UV Index to evaluate the potential efficacy of a sunscreen. Based on the WHO’s sun policy guidelines 32 that have been adopted by Australia and New Zealand 10, one may consider that all sunscreens with SPF ≥ 4 should generally offer effective protection against sunburn and melanoma. This is because the estimated SUI values (Figure 1) are all below 3 when sunscreens are applied in full compliance with the product instruction. In other words, incidences of sunburn or solar radiation-initiated melanoma after sunscreen use may not be used to evaluate their intrinsic sunscreen activities because these incidences may only largely reflect relative degrees of non-compliance with the application instruction under certain givenconditions. Therefore, the present work may provide a rationale of why an SPF 8 sunscreen may be effective against melanoma in the recent Australian study (15; more discussion later). Also, it appears that our consumers have been routinely warned to avoid sun exposure during the peak sun hours from 10 am to 2 pm without considering the UV Index for that day. For example, if the solar UV Index is only 3 or 5, rather than 10 as used in the present simulation, an SPF 4 sunscreen would yield a SUI of only 0.75 and 1.25, respectively, which probably should be considered as generally very safe. Also, in different places or on different days the peak solar UV Indexes could be less than 2 or 3 which generally may not cause a long-term harm to our skin 2, 8.
SPF-Independent Missing Applications as a Potential Major Cause of Sunburn and Melanoma
It is well recognized that in the real world, full compliance with product instruction is probably very rare. Regardless of sunscreen strength or sunscreen brand, the most serious problem is probably the missing application, especially in the back of the trunk, on the legs, around the ears and on the eyelid area 18, 19, 25, 35, 36, 37. It is very likely that sunburn would occur on these missed areas when exposed to intense burning sunlight 19, 20, 25, 26, 35, 36, 37; the sunburn is a known major risk factor for melanoma incidence. This is consistent with observations that melanoma occurred most often in the back of trunk in men where it is usually covered with clothes except during sunbathing 35. According to a telephone survey of 100 British adults, less than half of the people questioned would always apply sunscreen to all uncovered areas 19. In an elegant Danish study 25, it was found that the sunscreen was applied to only 80% of the total available exposed skin; in other words, a total of 20% of the exposed area did not have any sunscreen applied. Therefore, it is not surprising to find a report showing that after one week of a sunbathing vacation at a subtropical resort all Danish participants (N = 25) suffered unintended sunburn 38; in this study a broad-spectrum SPF 30 sunscreen was applied and a term “sunburn holiday” was used to describe such a holiday 38. Also, in one study involving 1,360 children from Sweden 39 sunscreen use was determined to be an independent risk factor for causing sunburn. In a study from Austria 40, sunscreen use was found to triple melanoma risk. Interestingly, sunscreen use was found to increase in Norwegian women between 1997 and 2007 but this increase was not accompanied by a decrease in sunburn 13, 41, as well as by a reduction in melanoma incidences in later years 42.
Recently in the US, results from two randomized, double-blind, split-face studies 29, 30 seemed to show superiority of SPF 100+ sunscreen over SPF 50+ sunscreen in preventing sunburn. For example, in a one-day study 5% of participants using SPF 100+ developed sunburn while 55% of participants using SPF 50+ developed sunburn 29. Most likely, the outcome might be quite different if the studies were conducted at a beach for sunbathing for one or several days. In another study 30 using an SPF 100 sunscreen on 7 body sites (back of the trunk not included) for sunbathing at a beach 25% of the participants developed sunburn. Likewise, the sunburn rate might be much higher if more days and the back of the trunk were included in the study. In a recent large-scale comprehensive novel study 43, sun-sensitive and non-sun-sensitive sunscreen users without employing other sun protection measures were associated with 64% and 26.2% of sunburn incidences, respectively. For sun-sensitive users use of sunscreen with all other protective measures such as seeking shade, wearing long sleeves and hats still yielded a 26.2% probability of getting sunburned 43.
The above limited review of the literature may suggest that using sunscreen to totally prevent sunburn in the real world may be virtually impossible and the possibility of incurring unintended sunburn especially after repeated sunbathing at a beach with high solar heat intensity would be very high or almost a certainty. It is not surprising that sunburn did indeed happen to his patients in the US who had applied the sunscreen diligently after being advised by their dermatologist 28.
Since in the US and many Northern European countries, sunscreens have been mainly used intermittently for intentional purposes 12, 13 such as at beaches with high or very high UV Indexes, the chances of suffering from unintended sunburn and hence unintended melanoma might be quite high. Therefore, one may hypothesize that sunscreen use may be considered as a major contributing risk factor for the exponential increase of melanoma incidences observed globally in the last few decades 42. The above hypothesis seems consistent with the known steady increase of global sunscreen sale in the last few decades apparently due to repeated advice from health professions and aggressive marketing campaign by the sunscreen industry. This view is also consistent with results from an extensive meta-analysis showing that sunscreen use was positively associated with melanoma incidences in countries of higher latitudes such as the US and Norway 16. The reported efficacy of using SPF 15 or greater for reducing melanoma incidences in Norway 13 may thus appear to be inconsistent with the present reasoning. It is noted in that study 13 sunscreen users reported significantly more sunburns than nonusers which is consistent with the present work. On the other hand, regular, daily, non-intentional use of sunscreen should be protective against sunburn, melanoma and other sunlight-related skin damage in lower-latitude, subtropical countries such as Australia, where the whole population is exposed to high ambient radiation 10, 15. It appears that the benefits from daily non-intentional use of sunscreens should also be attainable for those people residing in temperate climates.
Potential Limitation of the Present Modeling Study
The above simulations assume that an SUI of 3 may cause sunburn especially for sun-sensitive Caucasians or the white population in the US. Most of residents in the US may probably be able to tolerate a higher SUI for the following reasons. First, there does not seem to have had noticeable adverse reports related to the new Australian sun policy in the last several years 10, 44 since its implementation. Second, it seems well accepted that daily exposure to mild or moderate (UV Index 3 to 5?) sunlight may be protective against sunburn and melanoma 4, 8. Third, contrary to classical concepts that photoaging contributes up to 80% or 90% of skin aging, it was recently reported that generally skin aging may be mainly caused by the intrinsic nutritional factor 2, 8. Fourth, regular weekend exposure to sunlight without sunburn was found to be protective against melanoma in a British study 45. Although the solar UV Indexes in England were not reported in the study 45, they were probably expected to be about 4 to 6 in summer months 46. For non-white populations in the US their skin may be expected to tolerate even much stronger sunlight with the SUI probably approaching about 6 to 8 for one hour without incurring sunburn (8; more studies needed). In this regard the melanoma rate for blacks was reported to be about 20 to 30 times less than for whites 47. Moreover, there was no evidence to support the association of solar UV exposure and melanoma incidence in black or Hispanic population 47 and the major locations of their melanomas were often in relatively non-sun-exposed areas, such as the soles of feet, the palms of hands, toenails and oral gums 47, 48, 49. It seems that there is a great need for research to be conducted relative to the use of sunscreens in non-white populations because of its rapidly increasing share of the total population in the US.
Additional Discussion on the Efficacy of SPF 8 Sunscreen in Australia
When only 50% or 25% of the SPF 8 sunscreen is applied as this might occur in the real world, it is expected to yield a SUI of 3.6 or 5.9 (Figure 2 and Figure 3). However, when the decrease in solar UV intensity with a reduction of applied amount is estimated by a linear method 50, 51, the SUI would decrease to 3.1 or 5.0. In view of the discussion in the above section, it is likely that most residents in Australia can partially or fully benefit from the low SPF sunscreen especially when the applied amount is about 50% or more. Also, the SUI would decrease considerably if skin exposure to peak sun light is avoided, that may in turn enhance considerably the efficacy of the sunscreen.
Recommended use of Low or Very Low SPF Sunscreens in the US
In view of the above simulations and discussion it is proposed that an SPF 8 sunscreen may be adequate for sun-sensitive, light-skinned white populations. For non-sun-sensitive, darker-skinned, non-white populations in the US, sunscreens with very low SPF numbers such as 2 to 6 may be adequate. Support of this suggestion may be evident from the following example. If a person who can tolerates a UV Index of 7 without incurring a sunburn is regularly exposed to a sunlight with a UV Index of 8 while wearing an SPF 2 sunscreen, then the estimated Skin UV Indexes will be 4, 5.7 and 6.7 when full, 50% and 25% compliance in the amount are applied, respectively. Sin these Skin UV Indexes are all below 7, therefore, that person may not be expected to develop sunburn and is then safe to be exposed to that sunlight (footnote). Potential variability in sun sensitivity among different ethnical groups in non-white populations in the US may remain to be explored. Among some two dozen active sunscreen ingredients approved today for marketing, only two natural minerals, namely, zinc oxide and titanium dioxide, are regarded by the US Food and Drug Administration as safe and effective 1. For various reasons such as their extremely high chemical stability, non-absorption into the body 1, 52 and apparently proven safety track record in the last several decades of worldwide use, they should probably be considered as preferred active ingredients (detailed discussion being beyond the scope of this work).
Potential Applications of the Recent Nutrition-Based Aging/Anti-Aging Theory
In addition to providing a new perspective on skin aging and skin anti-aging as briefly mentioned above, the recent nutrition-based aging/anti-aging theory of Chiou 2 has also been successfully applied to develop a very simple, safe, quick method for regeneration of diverse tissues such as hairs, nails, skin and gums in humans by topical application of a high concentration of propylene glycol, a nutrient, apparently through rejuvenation of a tissue’s stem/progenitor cells 53, 54. This theory 2 could also provide a rationale of why a dramatic age-reversing, potentially age-prolonging, systemic effect could be observed after a simple rejuvenation of hearts in old rats 8, 55. It is also of interest to note that high concentrations of propylene glycol can also serve as an extremely effective, safe, universal topical microbicide 56, 57 with highly desirable moisturizing and absorption-enhancing properties.
Footnote: (This Footnote will be Deleted if Recommended)
** It may be useful to report an accidental observation below: A long-acting (lasting about 12 hours) moisturizer containing about 50% of glycerin 58 and determined to have an SPF of about 2 was used by one Taiwanese female before hiking in the summer while her sister did not wear any cosmetic or sunscreen. At the end of hiking the sister without applying the moisturizer got sunburned while the other sister did not get sunburned. The sun protection effect of this moisturizer is probably due to the moisturizing property of glycerin and water as well as the firming property 58 of glycerin through apparent rejuvenation of stem/progenitor cells in the skin 53.