Abstract
The objective of this first part of our study was to investigate associations of road traffic noise, socioeconomic and -demographic risk factors, and health access on depression on borough level.
We investigated in a large metropolis associations between prevalence rates of depression per borough (n = 67 boroughs) in all age groups (excluding the age group of 0–17 years) using health claims data (year 2011) and the variables “social deprivation” and “number of family members”, which were obtained from a previously conducted principal component analysis, and by using multivariate regression model. Additionally, the proportion of borough area affected by noise > 65 db(A) and physician density used as a surrogate parameter for health access were considered as potentially associated factors for depression.
The results demonstrated that depression might be associated with increasing social borough deprivation. Additionally, the number of family members used as a proxy measure for positive family support showed decreasing prevalence rates the more family members were present. Furthermore, proportions of borough areas affected by noise > 65 db(A) was positively associated with depression.
Our ecological study design has the advantage that a large number of large-scale, population-based aggregated data could easily be obtained and analysed and first potential associations could be found and discussed. To improve our findings, future studies will use data from a survey and data from the Hamburg City Health Study, a local follow-up health study, to better elucidate the individual risk factors together with environmental living and working conditions.
Author Contributions
Academic Editor: Roberto Maniglio, University of Salento, Lecce, Italy
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Anne Caroline Krefis, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Worldwide, major mental and behavioural disorders are increasing and account for approximately 7.5 % of disability-adjusted life years (DALYs) with major depressive disorder having the highest impact with 2.5 % within this group 1. In Germany, where this study was conducted, major depressive disorder is the seventh most frequent cause for loss of healthy years of life among men and the third frequent cause for DALYs among women 1, 2.
Environmental noise in urban areas is suggested to be one of the major risk factors for adverse health effects and several studies mainly investigated and showed the link between different noise sources and cardiovascular outcomes such as hypertension 3–5. However, fewer is known about the relationship between traffic noise 6, 7 or aircraft noise 8 and different mental disorders such as depression. Results from the Heinz Nixdorf Recall Study showed a relative risk (RR) of 1.29 (95 % confidence interval 1.03, 1.62) for participants classified as having high depressive symptoms for exposure to road traffic noise > 55 dB(A) compared to ≤ 55 dB(A) 6.
Furthermore, it is suggested that health access as well as social services might be associated with mental health outcomes and that there is a gradient of social and health services from urban to rural areas 9, 10.
Likewise, positive support from family was identified as a potential protective factor for the onset or the level of depressive symptoms. A follow-up study conducted in the USA revealed that patients recovered from depression by the time of the follow-up assessment reported higher perceived emotional support from family at baseline 11.
Additionally, a lower socioeconomic background is considered to be an important risk factor for poor mental health. Many studies investigated and showed the relationship between individual, educational and occupational background or income and different mental disorders such as depression and anxiety 12–15. Weich and Lewis 15 for instance investigated in a cohort study associations between poverty, unemployment and common mental disorders and showed that the duration of episodes of common mental disorders but not the likelihood of their onset were associated with unemployment and poverty, even after adjustment for other individual indices such as educational background or marital status 15. However, the use of single variables as potential risk indicators may lead to false conclusions because they only reflect parts of the general view.
Other studies have shown that local environmental and borough conditions may play an important role in the prevalence of psychiatric disorders as it has been investigated for instance in two studies conducted by Kirkbride et al. 16 in East London, United Kingdom and by Rejneveld and Schene 14 in the city of Amsterdam, the Netherlands.
Experimental Procedure
The aim of this first part of the study was to investigate associations between road traffic noise, socioeconomic and -demographic factors, and physician density on depressive disorder on borough level in the city of Hamburg. Particularly, by using the multivariate analysis of covariance (ANCOVA) model we assessed potential associations between prevalence rates of depression per borough in all age groups (excluding the age group of 0–17 years of age) and divided by sex using health claims data (year 2011) and the variables “social deprivation” and “number of family members”, which were obtained from a previously conducted principal component analysis (PCA). Furthermore, the proportion of borough area affected by noise > 65 db(A) and physician density used as a proxy measure for health access were considered as potentially associated factors for depression and entered the final model.
Material and Methods
Study area
This study was accomplished in the city of Hamburg, northern Germany, which is the second largest city in Germany, with approximately 1.8 million inhabitants (census data 2013) 17. Even though Hamburg in general can be described as a prosperous city, great heterogeneity considering socioeconomic and sociodemographic indicators between the 104 boroughs can be found (data 2013) (Figure 1) 17. Due to low prevalence in some of the boroughs in Hamburg some of the adjacent boroughs with similar socioeconomic and -demographic background information were combined and from the former 104 urban boroughs, 67 were received and used for all analyses. No data were available for the borough “Hafencity” 18.
Figure 1. Map depicting the city of Hamburg. Detailed information about the boroughs can be obtained from Table 1 (Own depiction, according to 1718).
| ID | borough | ID | borough |
| 1 | Allermöhe and Bergedorf | 35 | Jenfeld |
| 2 | Alsterdorf | 36 | Langenhorn |
| 3 | Altona-Altstadt | 37 | Lohbrügge |
| 4 | Altona-Nord and Sternschanze | 38 | Lokstedt |
| 5 | Bahrenfeld | 39 | Lurup |
| 6 | Barmbek-Nord | 40 | Marienthal |
| 7 | Barmbek-Süd | 41 | Neuallermöhe |
| 8 | Bergstedt and Wohldorf-Ohlstedt | 42 | Neugraben-Fischbek |
| 9 | Billstedt | 43 | Niendorf |
| 10 | Blankenese | 44 | Nienstedten and Othmarschen |
| 11 | Borgfelde and St. Georg | 45 | Ohlsdorf |
| 12 | Bramfeld | 46 | Osdorf |
| 13 | Dulsberg | 47 | Ottensen |
| 14 | Duvenstedt and Lemsahl-Mellingstedt | 48 | Poppenbüttel |
| 15 | Eidelstedt | 49 | Rahlstedt |
| 16 | Eilbek | 50 | Rissen |
| 17 | Eimsbüttel | 51 | Rotherbaum |
| 18 | Eißendorf | 52 | Sasel |
| 19 | Eppendorf and Hoheluft-Ost | 53 | Schnelsen |
| 20 | Farmsen-Berne | 54 | St. Pauli |
| 21 | Fuhlsbüttel and Groß Borstel | 55 | Borough cluster around Kirchwerder (Kirchwerder, Altengamme, Billwerder, Curslack, Moorfleet, Neuengamme, Ochsenwerder, Reitbrook, Spadenland, Tatenberg) |
| 22 | Groß Flottbek | 56 | Borough cluster around Marmstorf (Marmstorf, Langenbek, Neuland and Gut Moor, Rönneburg, Sinstorf) |
| 23 | Hafencity* | 57 | Borough cluster around Neuenfelde (Neuenfelde, Cranz, Francop, Moorburg and Altenwerder) |
| 24 | Hamburg-Altstadt and -Neustadt | 58 | Borough cluster around Rothenburgsort (Rothenburgsort, Billbrook, Hammerbrook) |
| 25 | Hamm | 59 | Borough cluster around Wilhelmsburg (Wilhelmsburg, Kleiner Grasbrook and Steinwerder, Veddel) |
| 26 | Harburg | 60 | Steilshoop |
| 27 | Harvestehude | 61 | Stellingen |
| 28 | Hausbruch | 62 | Tonndorf |
| 29 | Heimfeld | 63 | Volksdorf |
| 30 | Hoheluft-West | 64 | Waltershof and Finkenwerder |
| 31 | Hohenfelde and Uhlenhorst | 65 | Wandsbek |
| 32 | Horn | 66 | Wellingsbüttel |
| 33 | Hummelsbüttel | 67 | Wilstorf |
| 34 | Iserbrook and Sülldorf | 68 | Winterhude |
Prevalence rates of depression
Prevalence rates per borough for depression from the year 2011, which cover the 67 urban boroughs of Hamburg described above, were provided by the Ministry for Health and Consumer Protection of the Free and Hanseatic City of Hamburg considering the care claims data from the public health care system of all statutory health insured patients with at least one contact to a contract physician working in the ambulatory sector, including psychotherapists as the population (n = 203,172) 18.
The following ICD-10 codes were used for the health outcome: F32 depressive episode ("Depressive Episode"), F33 recurrent depressive disorder ("Rezidivierende depressive Störung") and F34.1 persistent depressive disorder ("Dysthymia"). Prevalence rates were divided by borough and sex and grouped by age (five groups: 0–17, 18–64, 65–79, 80+, and total) 18. Due to very low depression prevalence rates in the age group of 0–17 in both sex and hence, possible biased results, we excluded this age group and used the respective borough prevalence rates for the remaining summarized age groups.
Mapping (grid width: 10 m x 10 m; immission height: 4 m above ground level) depicting the noise level of Lden (Level day-evening-night) > 65 db(A) as a threshold for high exposure to noise was performed and obtained from the State Ministry for Urban Development and the Environment by using the software Predictor-LimA, version 11.1 19, 20. Additionally, population census data (data from 2013) were obtained from the Statistical Office for Hamburg and Schleswig-Holstein 17 and the road traffic noise map was overlayed with the population map by using the Geographical Information System ArcGIS 10.3.1. Afterwards, the resulting fractions were subsequently transferred to the number of potentially affected residents per building block by multiplying the area fraction with the total amount of inhabitants. Finally, the population data and the number of potentially affected residents by Lden> 65 db(A) were aggregated to the 67 boroughs, scaled in % per borough and used for further analysis.
Socioeconomic and sociodemographic borough characteristics
Information on social indicators on borough level were provided by the Statistical Office for Hamburg and Schleswig-Holstein 17. To classify a borough's economic and demographic situation, several socioeconomic and -demographic variables were considered to enter a PCA, which was previously conducted by Erhart et al. 18, 21. The following data (data from 2012) indicating the socioeconomic and -demographic borough characteristics were considered in the PCA (Table 2 on Page 34).
Table 2. Indicators considered for the Principal Component Analysis| Item | unit | year |
| SGB II benefit recipients | Proportion of the total population (%) | 2012 |
| SGB II benefit recipients below 15 years of age | Proportion of the population below 15 years of age (%) | 2012 |
| Households receiving benefits | Proportion of all households (%) | 2012 |
| Average income in € | Per taxable person | 2007 |
| High school students | Proportion of all school students (%) | 2012/2013 |
| Employees | Proportion of all working age population (15 to 64 years of age ) (%) | 2012 |
| Unemployed | Proportion of all working age population (15 to 64 years of age) (%) | 2012 |
| Younger unemployed (15 to < 25 years of age) | Proportion of the younger working age population (15 to < 25 years of age) (%) | 2012 |
| Older unemployed (55 to < 65 years of age) | Proportion of the older working age population (55 to < 65 years of age) (%) | 2012 |
| Unemployed under the SGB II | Proportion of all working age population (15 to 64 years of age) (%) | 2012 |
| Premature deaths | Per 1,000 inhabitants | 2012 |
| Children and adolescents < 18 years of age | Proportion of the total population (%) | 2012 |
| Inhabitants > 64 years of age | Proportion of the total population (%) | 2012 |
| Foreign inhabitants | Proportion of the total population (%) | 2012 |
| Inhabitants with migration background | Proportion of the total population | 2012 |
| Children and adolescents < 18 years of age with migration background | Proportion of the total population < 18 years of age | 2012 |
| Mean number of people | Per household | 2012 |
| Single-person household | Proportion of all households (%) | 2012 |
| Households with children | Proportion of all households (%) | 2012 |
| Households with single-parents | Proportion of all households (%) | 2012 |
| Human population density | Per km2 | 2012 |
| In-migrations beyond the border of the city | In total | 2012 |
| Out-migrations beyond the border of the city | In total | 2012 |
| Difference between the in- and out-migrations | In total | 2012 |
| Living space | Per inhabitant per m2 | 2012 |
| Social housing | Proportion of all flats (%) | 2012 |
The first factor of the PCA was used as the indicator, which might adequately describe the social deprivation of a borough and interpreted and titled as “social deprivation”. The respective factor scores were categorized in subgroups where the lowest 25 % of the boroughs pursuant to the social deprivation were classified as low social deprivation, the median 50 % as average social deprivation and the upper 25 % of the boroughs as high social deprivation.
The second factor which was identified by the PCA described the household size and number of children per family. This variable “number of family members” was used as a proxy measure for family support where high number of family members were interpreted as high positive family support and low number of family members as low positive family support. Likewise, the respective factor scores were categorized in subgroups where the lowest 25 % of all boroughs were classified as low number of family members, the highest 25 % as high number of family members, and the rest as average number of family members 18, 21.
Additionally, data about the physician density (general practitioner) per 1,000 inhabitants per borough used as a surrogate parameter for health access for people diagnosed with mental disorder were obtained from the Statistical Office for Hamburg and Schleswig-Holstein 17 and were considered as a further potential co-factor for the statistical analysis.
Statistical Modelling
All analyses were conducted using a borough´s respective overall prevalence rate for depression excluding the age group of 0–17 years of age and for both sex, separately. A multivariate ANCOVA (Analysis of Covariance) model was applied to quantitatively assess the associations between the socioeconomic and sociodemographic factors, as well as noise and physician density, and the borough prevalence rates of depression, using IBM SPSS Statistics, version 23. The independent variables “proportion of borough area affected by noise > 65 db(A)” and “physician density” were analysed as continuous variables and scaled at a unit of per 5 % increase in borough area. For the categorical variables “social deprivation” and “number of family members” a scaling unit of three groups (low, average, and high) was used, respectively. The covariates in the ANCOVA model were examined for interactions, but none could be confirmed.
Criterion for significance and therefore inclusion of an independent determinant in the final model was p ≤ 0.05. The measure of association between a co-variable and the respective depression prevalence rate was defined as the regression coefficient (B) adjusted for all other co-variables. All estimates of the regression coefficient were complemented by a 95 % confidence interval (CI) and a p value. The adjusted R-squared (R2) was provided as a measure of overall goodness-of-fit of the estimated statistical model.
Results
Prevalence rates of depression
The overall treatment prevalence rates of depression (year 2011), excluding the age group of 0–17 years of age, varied from 7.8 % to 18.5 % among males and from 16.8 % to 26.1 % among females (data not shown). The median value among females nearly doubled compared to males (21.7 and 12.6, respectively) (data not shown). Figure 2 illustrates the considered overall prevalence for depression per urban borough and showed highest prevalence rates in the boroughs clustered within the Hamburg-Mitte district and in some urban boroughs in the Wandsbek district. Lowest prevalence rates for depression could be detected in the outer parts of Hamburg. No major sex-specific differences could be detected.
Figure 2. Prevalence rates of depression and spatial distribution of the variables “social deprivation” and “number of family members” per borough, Hamburg, Germany, 2011. Overall treatment prevalence, excluding the age group of 0–17 years of age, both sex. Population are all statutory health insured patients with at least one contact to a contract physician working in the ambulatory sector, including psychotherapists per year. Classification of prevalence rates was conducted using quantiles. The variables “social deprivation” and “number of family members” were obtained from a previously conducted PCA 1721.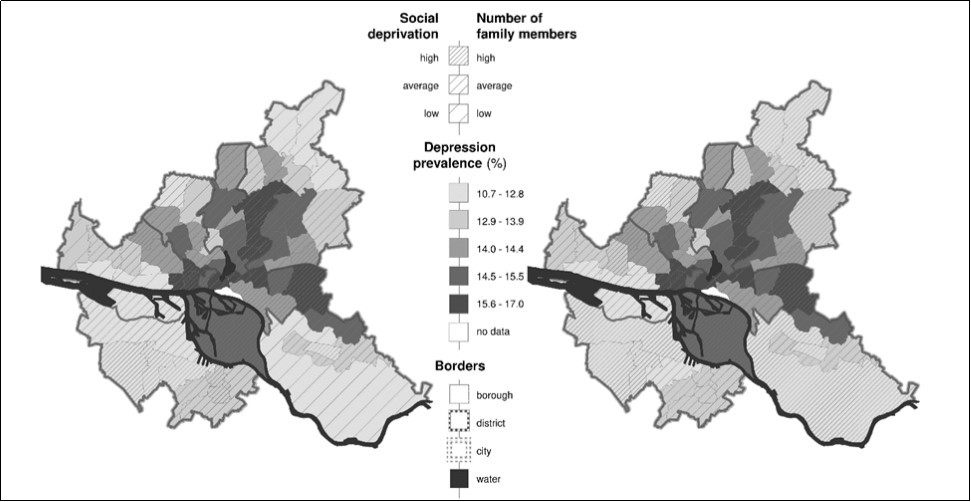
Socioeconomic and sociodemographic borough characteristics
Mapping of the spatial results of the social deprivation per urban borough, which was obtained from the PCA showed mainly comparable patterns to the depression prevalence rates and depicted for instance also highest social deprivation in the district of Hamburg-Mitte. This factor is characterised by indicators showing high positive correlations on the proportion of unemployment and the proportion of SGB II benefit recipients (SGB II: Social Security Code Sozialgesetzbuch Buch II). Accordingly, these boroughs record high unemployment rates and a high proportion of SGB II benefit recipients. On contrary, boroughs with the lowest social deprivation and hence, amongst others, low unemployment rates, were located in the most north-eastern boroughs and in the most western boroughs of Hamburg (Figure 2Figure 2). This pattern again predominantly coincided with low prevalence rates of depression. The second factor which was used as a surrogate parameter for positive family support had highest values in the peripheral boroughs. Smallest household sizes and hence, lowest positive family support could be found in the centrally located boroughs. Again spatially similarities to a borough´s depression prevalence rate could be mainly found (Figure 2).
Physician density
Physician density considering all general practitioners ranged from 0.2 physicians per 1,000 inhabitants in most borough-clusters in the southern parts of Hamburg to 10.4 physicians per 1,000 inhabitants in the centrally located boroughs of Hamburg (data not shown).
Proportion of road traffic noise > 65 db(A)
Additionally, the centrally located boroughs showed the lowest percentage of borough area affected by noise > 65 db(A) with 0.7 %. Highest percentage of borough area affected by road traffic noise level > 65 db(A) with up to 10.1 % could be found within the highly industrialised borough-cluster in Hamburg-Mitte (data not shown).
Multivariate regression analyses
The results of our analysis (Table 3) showed a significantly higher association of depression prevalence rates with an environment characterised by a fractional area increase (5 %) of road traffic noise > 65 db(A) per borough (males 2.38 %; 95 % CI 1.39, 3.36; females 1.44 %; 95 % CI 0.22, 2.65), but no significant results for the considered variable “physician density” (males 0.48; 95 % CI -0.48, 1.43; females 0.80; 95 % CI -0.38, 1.98). The prevalence rate for depression per borough was significantly associated with social deprivation showing an increase from low social deprivation to high social deprivation with 2.21 % (95 % CI 1.10, 3.31) among males. Living in a deprived borough was associated with higher depression rates of 1.41 % (95 % CI 0.06, 2.77) among females. Additionally, the variable “number of family members” used as a proxy measure for positive family support showed a significant decrease in depression from low positive family support to high positive family support with -1.29 % (95 % CI -2.49, -0.10) among men and with -2.39 % (95 % CI -3.86, 0.92) among women. However, an overall model fit of R2= 0.46 (males) and R2= 0.31 (females) indicates that more than 50 % of the variation of the observed prevalence rates cannot be explained by the independent variables of the model.
Table 3. Associations of determinants on depression, Hamburg, Germanya822325635952500| Depression male | Depression female | |||||
| Determinant | Coefficient Bb | 95 % CI | p value | Coefficient Bb | 95 % CI | p value |
| Physician densityc,d | 0.48 | -0.48,1.43 | 0.324 | 0.8 | -0.38,1.98 | 0.18 |
| Proportion of borough area affected by noise > 65 dB(A)c | 2.38 | 1.39,3.36 | <0.0001 | 1.44 | 0.22,2.65 | 0.021 |
| Low social deprivatione | NA | NA | NA | NA | NA | NA |
| Average social deprivatione | 0.7 | -0.24,1.63 | 0.141 | 0.14 | -1.01,1.29 | 0.809 |
| High social deprivatione | 2.21 | 1.10,3.31 | <0.0001 | 1.41 | 0.06,2.77 | 0.041 |
| Low number of family membersf | NA | NA | NA | NA | NA | NA |
| Average number of family membersf | -0.31 | -1.28,0.65 | 0.519 | -0.94 | -2.13,0.25 | 0.119 |
| High number of family membersf | -1.29 | -2.49,0.10 | 0.034 | -2.39 | -3.84,-0.92 | 0.002 |
Discussion
The current study was conducted in order to get insight into the potential association of depression with environmental and socioeconomic and sociodemographic factors. This topic is of particular importance since there is a marked increase in depression among the German population 2. This increase has led to a significantly increasing volume of health care expenses and still rising losses of productivity, both resulting in high direct and indirect costs 22. The first results of our study indicate that factors related to the socioeconomic and sociodemographic borough background as well as road traffic noise may be associated with the occurrence of depression in the city of Hamburg. Highest prevalence for depression could be found in most deprived areas, compared to boroughs with low social deprivation. Additionally, the proportion of depression was lower in boroughs where more family members, interpreted as positive family support, were present. Another independent factor was road traffic noise, showing higher prevalence rates of depression in boroughs with higher percentage of borough areas affected by noise > 65 db(A). Physician density used as a surrogate parameter for health access did not show any significant effect on depression rates on borough level.
Several studies have shown that local environmental conditions may play an important role in the prevalence of psychiatric disorders 12, 14, 16, 23. For instance, a study conducted in the city of Maastricht, the Netherlands, found significantly higher incidences and severity of psychiatric disorders in deprived neighbourhoods 24.
A PCA is a multivariate statistical technique used to reduce the complexity and dimensionality of correlated variables to one or more uncorrelated single indicator variables. Interpretation and comparison across settings such as urban boroughs as provided herein in this study are easier. On the other hand, the principal components are artificially constructed indices and the number of selected variables included and the number of components is arbitrary 25. However, the indicators which entered the PCA and were used in our study should be reliable and hence, should approximately reflect the socioeconomic and -demographic background of a borough.
Nevertheless, single socioeconomic indicators such as unemployment or income have also been shown to potentially be associated with mental disorder and many studies, reviews or meta-analyses have been published investigating or summarizing the socioeconomic effects on mental health such as depression or anxiety 13, 15, 26.
Number of family members, used as a proxy measure for positive family support, was an independent factor on depression. These results are consistent with other studies, investigating objective and subjective aspects of support from family 11 27–29. However, even though we used a high number of family members as a surrogate parameter for positive family support, it could contrarily have a negative effect on depression when for instance family conflicts are present 28, 29. Therefore, our results have to be interpreted with caution.
Furthermore, the proportion of borough areas affected by road traffic noise > 65 db(A) indicated associations with depression prevalence rates. Likewise, an impact of residential road traffic noise > 55 db(A) on high depressive symptoms has been suggested from the Heinz Nixdorf Recall study, conducted in three adjacent cities in western Germany 6. Same results could be found in a study conducted in the city of Tokyo showing associations between road traffic noise above a threshold of > 65 db(A) with sleep disturbance and depression 7. Nevertheless, a limitation of our study is that road traffic noise was transferred to the number of potentially affected residents per building block. Certainly this does not reflect the real environment or covers the real circumstances of noise exposure. Instead, other individual co-factors describing location of rooms, subjective noise annoyance or duration of residence should be taken into consideration 7, 8, 30, 31. Additionally, noise at workplace 32, 33 or other sources of noise such as aircraft or industrial noise 8, 31, 34 are suggested to affect psychological disorders. Additionally, exposure to gaseous and particulate air pollutants, which is generally higher in cities than in non-urban areas, has been associated with depression 31 or anxiety 35. However, no data on further noise sources or air pollutants in the city of Hamburg were available and so far, could not be considered in our study.
Physician density applied as a surrogate parameter for health access did not show any significant association with depression. Only data from general practitioners and not from psychotherapists were used to calculate the physician density per 1,000 inhabitants. In the German health care system people potentially suffering from mental disorder first have to see a general physician or practitioner for referrals to a specialist such as psychologists. Hence, only using the physician density as a proxy measure for health access for people diagnosed with several mental diseases should mostly represent the health care for mental disorder. However, in general people do not always seek medical care adjacent to their home-address. Instead, they seek help at a general practitioner or even specialist in a borough further away or go directly to the hospital. Hence, depression prevalence rates might be underdiagnosed and skewed in some particular groups of the population due to differences in seeking health care behaviour.
Another limitation of our study is, that only data from statutory health insurance patients with at least one contact to a contract physician working in the ambulatory sector, including psychotherapists were available. Data regarding the amount and distribution of privately insured patients or data from private practice were not available. However, it is suggested that roughly 10 to 20 % of all inhabitants in Hamburg are privately insured 18, 21, therefore the prevalence rates used here in our analyses should cover the largest proportion of diagnosed cases. Nevertheless, due to the high costs of the private insurance, mostly people above a certain income level can afford this status. Hence, our results might be skewed in low deprived boroughs due to the lack of data from the privately insured individuals.
Furthermore, it is suggested, that the insurance status might be associated with the treatment and hence, the health outcomes of individuals. For instance, two studies in the USA investigated the influence of insurance status on the access to mental health care. Both studies found associations between the insurance status and unmet need for mental health care or the acceptance rates 36, 37. Additionally, a higher number of unreported cases might not be considered in our study, because not all people showing depressive symptoms do seek help at a psychotherapist. Additionally, differences in motivation for psychotherapy and illness beliefs might be one reason for underestimation of cases as shown in a study conducted among Turkish Immigrant inpatients in Germany 38. Furthermore, not all ICD-codes for depressive disorders such as F48.0 describing Neurasthenia or F92.0 describing depressive conduct disorder, were considered for our health outcome depression. Therefore, the data used in our study only capture a fraction of the estimated prevalence and hence, might have an underestimation bias in their acquisition.
Due to very low borough prevalence rates among the age group of 0 to 17 years of age in both sex (approximately 0–2 %) and hence, a possible false estimation of the respective effects, we excluded this group in the final model. Prevalence rates among the remaining age groups were approximately evenly distributed (among males range between approximately 10–20 %, among females range between approximately 15–25 %) and were chosen as one group for the analysis. Nevertheless, to check stability of the observed results, we repeated the ANCOVA model with the age group 0 to 17 years of age included. “Number of family members” as well as “social deprivation” had somewhat higher significant estimates of the coefficient B, instead “proportion of borough area affected by noise > 65 db(A)” indicated a halving of the depression prevalence (data not shown). Reversely, this result might underline the possible association of long-term effects of noise above a certain threshold and additionally the importance of duration of residence on mental disorder.
An advantage of our cross-sectional ecological study design is, that a number of large-scaled, population-based data could easily be obtained for the city of Hamburg and first theoretical associations might be analysed and discussed. Our results obtained here on borough level show similar association as demonstrated in other studies underlying the potential importance of social depravity of a borough in relation to specific disease outcomes, even though the study design used so far makes the results of this study difficult to interpret and potentially misleading.
In a next step we will conduct a case-control study with hypertensive patients as cases to get a better insight into the potential individual risk factors together with environmental living and working conditions. Participants from the Hamburg City Health Study (HCHS), the largest local follow-up health study, which just started spring 2016 and with follow-ups for the next 12 years will be matched and used as a control group. Additionally, data about noise (traffic noise, aircraft noise as well as industrial noise) and data about air pollution will be selectively collected close to the residents of participants and considered in the upcoming studies to account for the above discussed limitations and hence, to better analyse and understand potential individual and environmental co-factors of depression.
Conclusion
Our first results presented herein suggest that the socioeconomic and sociodemographic background of an urban borough could have a considerable effect on depressive disorder. A significantly higher prevalence for depression was detected for highly deprived boroughs. Furthermore, road traffic noise > 65 db(A) indicated a significant association with depression in the city of Hamburg. Our results suggest that large-scale socioeconomic and -demographic borough data together with noise, which could easily be obtained might be useful to pose potential associations between a borough´s socioeconomic and sociodemographic background, noise and different health outcomes such as depression. However, to regard the limitations of our study future studies will focus on collecting information on individual level and the environmental living and working conditions together with data on noise and air pollution in the near living environments of participants. These are prerequisites to assess the validity of our model and to develop strategies to reduce the increasing prevalence of depressive disorder.
Acknowledgements
This contribution is based on the work of the research project “Cities in Change – Development of a multi-sectoral urban-development-impact model (UrbMod)”, a joint project of University of Hamburg, Hamburg University of Technology, University Medical Center Hamburg-Eppendorf, Institute of Coastal Research at Helmholtz Center Geesthacht, Max-Planck-Institute for Meteorology, and Hafencity University, funded by the State of Hamburg.
We thank the Ministry for Health and Consumer Protection of the Free and Hanseatic City of Hamburg for providing the health data and the Central research institute of ambulatory health care in Germany (Zentralinstitut für die kassenärztliche Versorgung in der Bundesrepublik Deutschland) for the provided disease prevalence rates and the results, which were obtained from Principal Component Analysis. Additionally, we would like to thank the Statistical Office for Hamburg and Schleswig-Holstein for the socioeconomic and sociodemographic data on borough level. The authors wish to thank Marie Christine Duval, Sara Tiedemann and Mario Gehoff as part of the scientific communications team of the IVDP for copy editing. Finally, we thank the State Ministry for Urban Development and the Environment for the maps depicting noise.