Abstract
The prevalence of young adults endorsing depressive symptomatology is thought to peak during late adolescence. While there has been a wealth of research assessing the relationship between decline of the prefrontal cortex and how this process impacts depression and therapy in older adults, very little is known about the relationship on the younger end of the continuum. The current study sought to explore whether there is also a significant relationship between executive functioning and depression in younger adults. In addition, different types of executive dysfunction were assessed to better understand the possible implications for therapy in younger adults with depressive symptomatology. Data from 1,730 college-aged participants were collected on measures of depression (Center for Epidemiological Studies-Depression, CES-D) and executive dysfunction (Dysexecutive Questionnaire, DEX). In addition, three factors of the DEX were assessed; Executive cognition (EC), emotional/ behavioral control (EMO), and metacognition (MC). Correlations between CES-D scores and the full DEX survey were statistically significant (R = .45, p < .001) as were correlations between CES-D scores and scores on each individual factor (p< .001). A multiple linear regression was run to demonstrate the predictive value of each individual DEX factor as a function of CES-D scores (p < .001). Results suggested that there was a clear relationship between depressive symptoms and executive dysfunction and that all factors of the DEX appeared to be affected by depressive symptoms in this population. The implications of these results for therapy, particularly the use of problem-solving therapy or complimentary executive functioning training are discussed.
Author Contributions
Academic Editor: Chi-Un Pae, The Catholic University of Korea
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Deana B Davalos et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
The relationship between executive functioning (EF) and depression, both in terms of the etiology of the disorder and the efficacy of treatment, has been a topic of growing interest to researchers. There has been a wealth of studies over the past two decades stressing the importance of understanding the role of (EF) in treatment of older adults with depression.1, 2, 3, 4 EF is a complex construct, but generally thought to encompass higher-order cognitive processes that are necessary for successful everyday activities.5 The role of EF in older adults is of particular interest due to the relationship between EF and the frontal lobes, specifically the prefrontal cortex (PFC). For decades, researchers have noted changes in the PFC of older adults that suggest greater decline than other brain regions.6, 7, 8, 9, 10 The motivation for studies assessing the relationship between EF and depression is clear, without optimal EF skills, therapies relying more heavily on EF skills may be less effective than those that do not.1, 11, 12 Studies comparing types of therapies in this population find clear preferences in terms of alleviation of symptoms and in terms of outcome measures.1, 13, 14In addition, certain EF skills appear particularly useful in predicting the course of depression and response to interventions. Specifically, tasks indicating impaired initiation and perseveration have been associated with poorer response to antidepressant medication.1, 14 These studies suggest that understanding the EF profile may provide clinicians with greater insight in to more efficacious interventions.In contrast to the wealth of literature exploring EF and depression in older adults, there is relatively little research in younger adults, who have similar characteristics that make their relationship between mood and EF relevant for therapeutic interventions. Similar to older adults who have a unique relationship between EF and depression due to the decline in the PFC, younger adults also have a unique relationship between their PFC and EF. Young adults are thought to have maturing PFC, suggesting that for some, there may be less than ideal performance on measures assessing the PFC. 15, 16, 17, 18In addition, young adulthood is considered to be the greatest risk period for the initial emergence of a variety of psychiatric disorders.19, 20 Understanding the relationship between EF and depression in young adults could potentially be even more useful than for older adults. For example, young adults may be navigating many firsts in their lives (e.g. college, full time jobs, making romantic relationships, decisions about their future) that require higher level cognitive functioning. And the limited research that does exist with younger adults suggests that EF dysfunction can in fact be a barrier to treatment.21, 22 Therefore, we sought to explore whether there is a significant relationship between EF and depression in younger adults, specifically non-clinical depressed college students. In addition, based on previous research in the older adult literature, we examined what types of executive dysfunction are most notably related to depression in this population to better understand what the possible implications may be in terms of providing efficacious therapy to younger adults with depressive symptomatology.
Methods
Participants
A survey screening for depression and Dysexecutive Syndrome was administered to undergraduate, introductory level psychology students (N = 1,539; N=1079 females) at a large university. The mean age of the participants was 19.5 years, standard deviation 2.3 years.
The participants identified as roughly 81% Caucasian, 9% were of Hispanic decent, 4% Asian/Pacific, 3% Alaskan, 2% Black, and 1% were of Native American decent. Depressive symptomatology was analyzed using the Center for Epidemiologic Studies Depression scale (CES-D).23 DYSEXECUTIVE syndrome was analyzed using the Dysexecutive Questionnaire (DEX)23 and all items were self-reported. Both questionnaires were a part of a larger screening survey that also included questions regarding basic demographic information, substance use, and general medical history. Participation was voluntary and anonymous and participants were treated in accordance with the "Ethical Principles of Psychologists and Code of Conduct”24. Participants received extra credit for participation. All participants provided consent that was approved by the institutional review board.
CES-Depression Scale
The CES-D is a 20 item questionnaire that may be used as a screening tool for depressive symptoms. The range of scores is 1 to 53 with a mean of 13.35 (SD = 8.68). The internal consistency reliability score is .91.22 All questions were coded in occurrence with the standard scoring guide.22 Responses were recorded on a 4-point Likert scale where 0 referred to “rarely or none of the time,” 1 referred to “some of/a little of the time,” 2 referred to “occasionally or a moderate amount of time,” and 3 referred to “all of the time.” Only questions 4,8,12, and 16 were reverse coded.
DEX Questionnaire
The DEX Questionnaire can be used as a screening tool to examine behavioral deficits associated with Dysexecutive Syndrome. There are 20 items on the DEX and responses are measured on a 5-point Likert scale, where higher scores correlate with more behavioral and cognitive problems. Responses were coded from 0 to 4 where 0 referred to “never” and a score of 4 referred to “very often.” The highest possible score on the DEX is 80 and the lowest possible score is 0.
There have been various studies that have divided the DEX into various numbers of components. Simblett and Bateman25 built off the Rasch analysis and organized the DEX into 3 components. For purposes of the present study, the DEX was divided into those 3 factors to potentially identify areas of dysfunction of higher-order processes: Executive cognition (EC), emotional/behavioral control (EMO), and metacognition (MC). Factor 1 (EC) executive cognition (total possible score = 16) evaluated abstract thinking, planning, temporal sequencing, and distractibility (items 1, 4, 6, and 18, respectively). Factor 2 (EMO) emotional/behavioral control (total possible score = 36) evaluated confabulation, lack of insight, apathy, disinhibition, variable motivation, lack of concern, perseveration, restlessness, and knowing-doing dissociation (items: 3, 7, 8, 9, 10, 13, 14, 15, and 17, respectively). Factor 3 (MC) metacognition (total possible score = 20) evaluated impulsivity, euphoria, aggression, inability to inhibit response, and no concern for social rules (items: 2, 5, 12, 16, and 20, respectively).
Results
All calculations were completed in Microsoft Excel and R. To identify outliers, all data points were transformed into z-scores. In the Full DEX, 43 values exceed the +/- 2.5 outlier mark. Outliers were removed from Full DEX and CES-D scores, then each factor of DEX and 1539 values were left. In Factor 1 (EC) 27 values were identified as outliers. Factor 2 (EMO) had 12 and Factor 3 (MC) had 28. Scatterplot representations of the data after outliers were removed are presented in Figure 1.
Figure 1. (A) CES-D Score compared to Average total Dex scores (Highest possible score = 80), Executive Function (EF) (Highest possible score = 16), Emotional/Behavioral Control (EC) (Highest possible score = 36), and Metacognition (MC) (Highest possible score = 20). (B) Scatterplot of All Scores of Depression Correlated with DexFull (C) Scatterplot of All Scores of Depression Correlated with Factor 1 (EC) of Dex (D) Scatterplot of All Scores of Depression Correlated with Factor 2 (EMO) of DEX (E) Scatterplot of All Scores of Depression Correlated with Factor 3 (MC) of DEX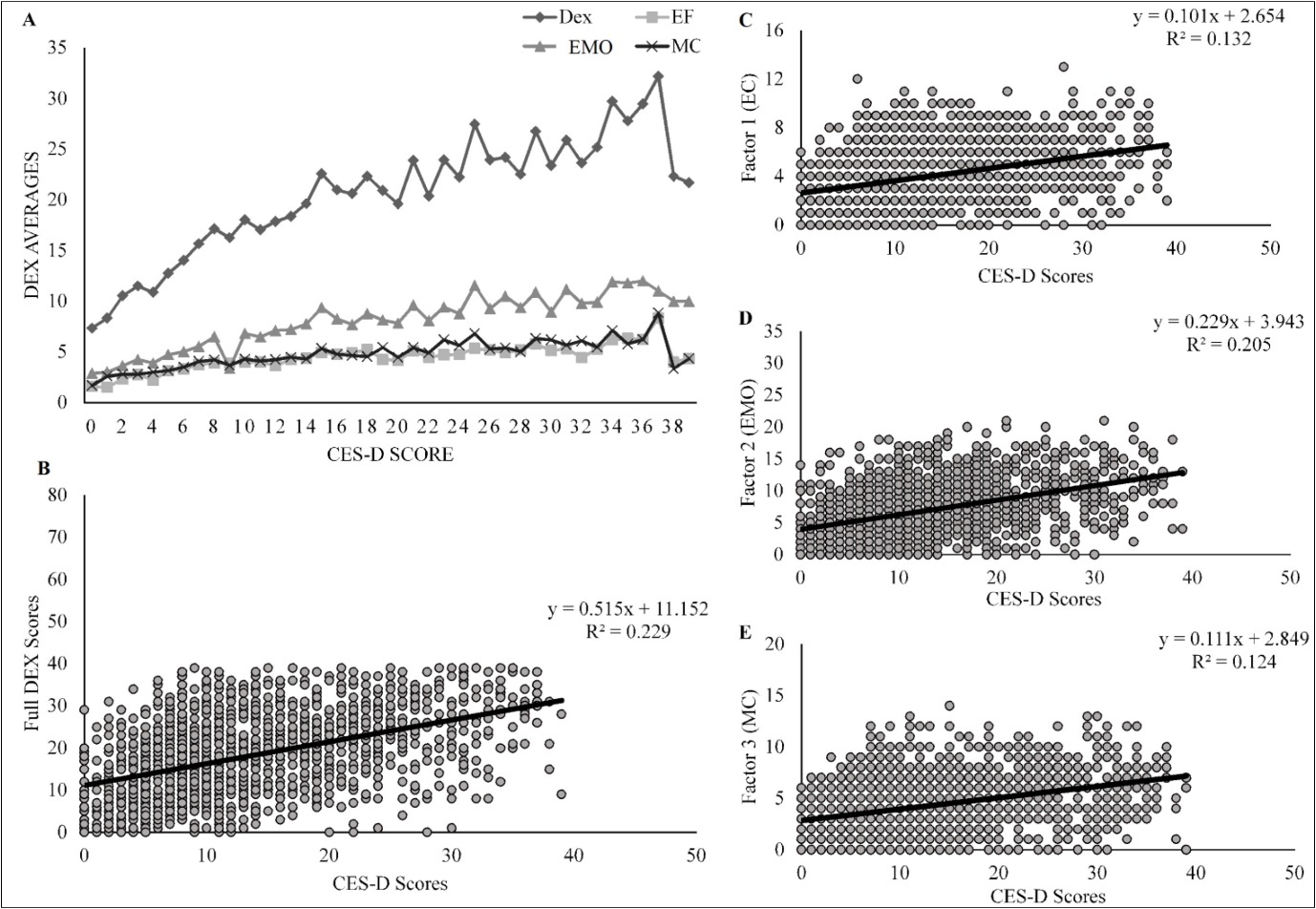
The overall mean score on the CES-D was 13.3 (SD =8.68) and on the DEX was 18.00 (SD = 9.42) (see Table 1). The minimum score for all full surveys and survey factors was 0. The maximum score for CES-D was 35 and DEXFull was 41. The max scores for each of the factors (1-3) were 14, 22, and 15, respectively. Initial correlations using Pearson’s R were conducted to demonstrate if any relationship existed between CES-D scores and the full DEX survey (R = .478, p < .001). Correlations were also examined between CES-D scores and scores on each individual factor (see Table 1). In an attempt to minimize the inflation of Type 1 error, the alpha level was set to p < .01. All correlations were significant at the .001 level. A multiple linear regression was run to demonstrate the predictive value of each individual DEX factor as a function of CES-D scores (F(3, 1535) = 125.10, p < .001) (see Table 2).
Table 1. Descriptive Statistics for CES-D by DEX Factors| Survey | N | Mean | SD | Pearson’s R |
| CES-D | 1539 | 13.35 | 8.68 | -- |
| DEXfull | 1539 | 18 | 9.42 | 0.45*** |
| Factor 1 (EC) | 1539 | 3.99 | 2.39 | 0.34*** |
| Factor 2 (EMO) | 1539 | 7 | 4.43 | 0.43*** |
| Factor 3 (MC) | 1539 | 4.29 | 2.67 | 0.34*** |
| b | SE(b) | t | |
| Intercept | 6.44 | 0.4 | 16.01*** |
| Factor 1 (EC) | 0.32 | 0.11 | 2.94* |
| Factor 2 (EMO) | 0.62 | 0.07 | 9.64*** |
| Factor 3 (MC) | 0.23 | 0.1 | 2.33* |
A hierarchical regression analysis was used to assess the relationship between each factor of DEX and CES-D score and to account for biological sex of the participants. Sex was significantly related to CES-D (F(1, 1529) = 31.65, p < .001, R2 = .02). While holding sex constant, the factors accounted for 11 times the amount of variance in the model (F(4, 1526) = 110.7, p < .001, R2= .22). Sex explained 2% of the total 22% variance explained by the final hierarchical regression (see Table 3).
Table 3. Coefficients for DEX Factors Regressed on Depression holding constant Sex| b | SE(b) | t | |
| Intercept | 4.11 | 0.5 | 8.21*** |
| Sex | 3.18 | 0.41 | 7.83*** |
| Factor 1 (EC) | 0.27 | 0.11 | 2.50* |
| Factor 2 (EMO) | 0.66 | 0.07 | 10.39*** |
| Factor 3 (MC) | 0.24 | 0.1 | 2.44* |
Discussion
In the current study, we sought to explore the relationship between depressive symptomatology and dysexecutive symptoms in college-aged young adults. The primary goal of the study was to establish (1) whether dysexecutive symptoms were related to depressive symptoms, which have been established in older adults, and (2) whether there were certain EF skills that appeared to be compromised to a greater degree than others. The present study assessed young adults who did not meet criteria for a diagnosis of clinical depression, but simply endorsed depressive symptomatology on a well-established measure of depression. Thus, findings suggested existence of a relationship based on a population of young adults who would be viewed as high-functioning by societal standards, but self-reported enough symptoms, such that these individuals may be at-risk of further development of depression.
Results suggested that there was a clear relationship between depressive symptoms and executive dysfunction. Specifically, the greater degree of depression endorsed was associated with higher levels of dysexecutive symptoms. One meaningful finding was that all facets of the dysexecutive syndrome questionnaire appeared to be affected by depressive symptoms in this population. In past studies assessing depression in young adults, there were generally limited cognitive factors that appeared to be affected (e.g. perseveration, set shifting) while the majority of other cognitive factors appeared to be intact (e.g. fluency, alternating attention, working memory).26, 27, 28 There are a variety of reasons that may explain the wide range of difficulties associated with DEX factors. First, the DEX is a self-report measure rather than a neuropsychological battery of tests. The DEX was selected in the current study due to the ease of administration to participants (i.e. could be administered to a large number of participants via an online survey). Furthermore, the questionnaire is viewed as an ecologically valid measure of executive functioning.24 Additionally, studies assessing non-neurological based populations described as having potentially reduced executive dysfunction, have found that questionnaires like the DEX were able to detect more subtle executive problems in everyday life more accurately than traditional neuropsychological batteries.29, 30, 31 Given that our population included a heterogeneous population in terms of depressive symptoms, the DEX was selected as it may be more sensitive to detecting slight executive dysfunction in individuals endorsing more subtle depressive symptoms.
The findings suggested that, similar to older adults, executive dysfunction may play a large role in everyday difficulties that young adults with depression may experience. While past research using the DEX and CES-D in older adults31 has suggested a relationship between these two measures, the current study suggested that the DEX and CES-D may also be used to measure this relationship in younger adults. In addition, previous studies with different young adult clinical populations (e.g. mild TBI) which have utilized the DEX suggested only limited factors of executive dysfunction; however, the current study reinforced findings of widespread trends in dysexecutive dysfunction in young adults with depressive symptomatology.32 These results also suggested that, similar to older adults, consideration has to be given to the types of therapies that may be best suited for young adults with depressive symptomatology. As Paelecke-Habermann and colleagues33 argue, while antidepressant therapy and other traditional therapies, such as CBT, may be effective methods of targeting depression, additional deficits in EF should also be addressed. The specific method for addressing EF deficits can be integrated into the talk therapy itself, as is the case with problem solving therapy (PST) or via the use of additional executive function training as a complementary treatment for depression.33 In the case of PST, the therapy tends to focus on the development of problem-solving skills and approaches applicable to every-day crises where as other types of talk therapy tend to focus on symptoms and symptom alleviation.34 In addition, PST has been shown to be effective in young adults with major depression35as well as in individuals diagnosed with what are often viewed as core dysexecutive syndromes, such as schizophrenia.36 In addition, PST appears to be effective over a wide range of depressive symptoms and across various types of executive dysfunction.33 Lastly, PST has been shown to be effective across a variety of types of administration, including internet based therapy. Internet based therapy has been shown to be more cost-efficient, easier to access, and less stigmatizing than traditional in-person treatments.37, 38 Kleiboer and colleagues39 found that brief internet-delivered PST effectively treated both depression and anxiety symptoms (compared to a wait list control). Those in the internet-based PST experienced a statistically significant reduction in anxiety and depressive symptoms following only five sessions of self-help internet based modules with relatively little time from a therapist or support coach. It should be noted that while the current study sought to provide an initial exploration of the role of executive dysfunction in depression in young adults, there are still limitations that need to be addressed for future research. The current study utilized a cross-sectional approach to examine the association between depression and executive dysfunction. Given the cross sectional design, however, it is not possible to determine the direction of the relationship (e.g. does executive dysfunction lead to depression or does depression lead to executive dysfunction). In addition, the current study utilized self-ratings to establish the presence of depressive symptoms and to measure facets of executive functioning, rather than structured clinical interviews and more traditional neuropsychological measures of executive functioning. While the measures were chosen due to their utility and ease of assessment, we cannot rule out that there may be other factors that are associated with the described relationship that led to a significant finding such as response bias or the negative interpretation bias that has been described in previous studies.40. Future research assessing the relationship between traditional methods of assessment and the self-report measures used in the current study would be helpful to determine whether these two types of assessment can be used interchangeably.
It should also be noted that there is limited research assessing the utility of the DEX in non-clinical or sub-clinical populations. The current study utilized the original three factors developed by the authors of the DEX41. However, since the DEX was published, there have been alternative models that utilize different questions and factors in the DEX. Factor analysis did not confirm the Wilson 3-factor solution with this population, suggesting that future research might be better suited comparing the current factors with the 15 item DEX-R proposed by Shaw and colleagues42
Conclusion
Previous trends coupled with present study results further emphasize the need to identify and address EF deficits in young adults with depression and raise clinicians’ awareness of effective and cost-efficient treatments that not only address depressive symptomatology, but also improve EF skills in young adults with depression.