Abstract
When a composite resin restoration is photopolymerized, a considerable amount of heat can be produced, potentially causing pulpal injury. Objective: Evaluate the influence of the type of light source and remaining dentin thickness on the temperature increase in the pulp chamber while curing composite resin restorations. Material and Methods: Ninety-six tooth fragments obtained from bovine incisors were divided into groups/subgroups (n=12), according to the light source (LED and halogen light) and remaining dentin thickness (3.5, 3, 2, and 1mm). Class I cavities were prepared and restored with a composite resin. A temperature increase was obtained during photopolymerization of the adhesive and each composite increment. Data were analyzed using ANOVA and Fisher’s Test (α=5%). Results: LED promoted higher temperature increments when compared with the halogen light. Temperature levels were the lowest for 3.5mm-thick and the highest for 1mm-thick remaining dentin. Levels registered during the photopolymerization of each composite increment were superior for LED. Conclusions: Both light sources result in temperature increases above 5.5°C. Additionally, the remaining dentin thickness of 1mm promoted the largest temperature increase.
Author Contributions
Academic Editor: Eduardo da Silva, Analytical Laboratory of Restorative Biomaterials - LABiom-R, School of Dentistry, Federal Fluminense University
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Regina Guenka Palma-Dibb, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Since the introduction of dental composite resin in clinical practice1, improvements have been made to enhance the clinical performance of this restorative material. One example of development in this area is the use of visible light-cured composite resins2. Ultraviolet light was the first light source to be employed to initiate the polymerization reaction of dental composite resins; however, this light source had a direct negative influence on the mechanical properties of composite resins3,4.
Quartz-tungsten-halogen (QTH) curing units have been widely used in the polymerization of composite resins with satisfactory results3,5. However, these curing units have some inherent limitations, such as generation of heat and degradation of the halogen bulb, reflector, and filter, all of which reduce the efficiency of the curing unit5, 6, 7.
In the 1990s, new polymerization techniques and curing units were introduced in the field of restorative dentistry, such as the use of light emitting diode (LED) curing units8. These units do not require the presence of filters to emit a wavelength in the 400 to 500 nm range, which is required to excite the camphoroquinone photoinitiators9. Therefore, LED units do not emit wavelengths in the infrared spectrum, so their operation requires less energy10, generating low amounts of heat9.
Previous studies11, 12, 13, 14have evaluated the temperature increase in the pulp chamber during photopolymerization of composite resins. When composite resins are photopolymerized, a considerable amount of heat can be produced. This is due to the light energy of the light-curing units as well as the exothermic character of the polymerization reaction15. Intrapulpal temperature changes are related to the features of the light-curing units, including wavelength, irradiance and curing time, as well as the characteristics of the composite, like shade and filler content. The restoration size and the features of the tooth, including thickness and quality of the remaining dentin also influence intrapulpal temperatures16. Possible thermal injuries are minimized by the dentin tissue, since it presents low thermal conductivity17. However, cavities containing a minimal thickness of remaining dentin are subject to a significant increase in thermal diffusion, thereby facilitating pulpal injury12,18,19.
Although intrapulpal temperature is a determinant of injury, there are few studies evaluating the extent of temperature increase that can be supported by the pulp. A classic study of Zach and Cohen20 (1965) observed that a temperature increase of 5.5ºC can lead to significant histological changes in the pulp, culminating in necrosis. Considering the high demand of composite resin restorations and the clinical importance of preventing potentially harmful temperature increases in the pulp, the purpose of this study was to evaluate the change in temperature at the roof of the pulp chamber caused by composite resin restoration by employing two light-curing units and varying the thickness of the dentin remaining in the cavities.
Materials and Methods
Experimental Design
This study had a complete block design with 12 experimental specimens per group/subgroup. The variation factors examined were light-curing unit at two levels (quartz-tungsten-halogen (QTH) light and LED) and remaining dentin thickness at four levels (3.5 mm, 3.0 mm, 2.0 mm, and 1.0 mm). The quantitative response variable was temperature increase in Celsius degrees (°C) registered at the following times: during the whole restorative procedure and during photopolymerization of each composite resin increment.
Specimen Preparation
Bovine incisors were used. These teeth were kept in distilled water at 4°C for no longer than six months and cleaned with scalpels and water/pumice slurry using dental prophylactic cups. They were then examined under 20X magnification, and those with structural defects were discarded. A total of 96 teeth were selected and their crowns and roots were separated with a cut 2.0 mm below the cement enamel junction using a water-cooled diamond saw in a precision cutting machine (Isomet1000, Buehler GmbH, 40599 Dusseldorf, Germany). The crowns were individually fixed with wax to acrylic plates and their vestibular surfaces were sectioned, in both mesio-distal and inciso-cervical directions, to obtain specimens with dimensions of 7 mm x 6 mm x 4 mm, respectively. Specimens were randomly assigned into 2 groups (halogen light and LED) and further divided into 4 subgroups according to the remaining dentin thicknesses: 3.5 mm (0.5 mm enamel and 3.0 mm dentin), 3.0 mm, 2.0 mm, and 1.0 mm, with variations in depth of ±0.1mm.
The specimens received cavity preparations (3 mm mesio-distal width and 2 mm inciso-cervical height) using #245 high-speed carbide burs under water-cooling. The depths of the cavities, as measured by a premarked digital paquimeter, were sufficient to determine the thickness of the remaining dentin. Three small orifices (one central and two laterally in relation to the cavity) were made using a # ½ low-speed carbide bur on the roof of the pulp chamber surface of each specimen, to which the thermocouples were attached.
Restorative Procedure
Before performing the restorations, each specimen was fixed to an acrylic plate containing a central opening that exposed both the cavity preparation and the roof of the pulp chamber.
Prior to applying the adhesive agent, type K thermocouples (Omega Engineering Inc., Stamford, CT, USA) were inserted into the orifices in the roof of the pulp chamber using a water-based thermal paste, in order to maintain good thermal contact between the thermocouples and the specimen. The cavities were restored according to the following protocol: 35% phosphoric acid gel (Scotch Etchand, 3M ESPE, St Paul, MN, USA) was applied for 15 seconds, water/air was sprayed for 40 seconds, and excess moisture was blot-dried using soft paper, leaving the surface visibly moist. Then, two consecutive thin layers of adhesive (Single Bond, 3M ESPE, St Paul, MN, USA) were applied and photopolymerized for 20 seconds using the light-curing unit corresponding to the study group. A microhybrid composite resin of shade A3 (Filtek Z250, 3M ESPE, St Paul, MN, USA) was inserted into the cavities in three increments, except for the 0.5-mm-deep cavities (remaining dentin thicknesses: 3.5 mm), which received one increment only. The first two increments were applied obliquely against the mesial and the distal walls, respectively. The final increment was inserted by flushing the contour of the specimen. Each resin increment was photopolymerized for 20 seconds. The characteristics of the light-curing units are presented in Table 1.
Table 1. Light-curing units used in this study.| Equipment | Manufacturer | Light source | Wavelength | Intensity |
| Ultralume LED 5 (group1) | Ultradent Products, INC. South Jordan, UT 84095, USA | LED | 370 to 500nm | 930mW/cm2 |
| Jet Lite 4000 Plus (group 2) | J.Morita USA INC 9 Mason Irvine, CA 92618 USA | Halogen | 400 to 500nm | 900mW/cm2 |
Temperature Measurements
All measurements were performed in a temperature/humidity-controlled room with a constant temperature of 21°C and 30% relative humidity. For temperature measurements, the initial temperature was recorded following temperature stabilization (21°C). For each specimen, the temperature was registered from the start of the adhesive photopolymerization until temperature stabilization after photopolymerization of the last composite resin increment.
Temperature was registered by three type K thermocouples connected to a portable USB-based data acquisition module (NI USB-9211A, National Instruments Co., Austin, TX, USA) with 4 channels of 24-bit resolution. The equipment was calibrated with 0.2°C of accuracy and a response time of 0.6 seconds. For each specimen, the mean value of the three thermocouples was considered.
Data Analysis
Data distribution was verified by Levene and Shapiro-Wilks’ tests as normal and homogeneous. Therefore, two-way Analysis of Variance (ANOVA) and Fisher LSD post-hoc test were used to determine differences in the mean temperature increase between light-curing units and among the remaining dentin thicknesses at a significance level of a=5%. All statistical procedures were performed using the software Origin 8 - data analysis and graphing software (OriginLab Co. - Northampton, MA 01060 USA).
Results
For light-curing unit factor the analysis of the data revealed that regardless of the dentin thickness, the LED light-curing unit showed significantly higher temperature increases (10.76±2.48°C) when compared with QTH (7.43±2.23°C) (p<0.05). In relation to the factor remaining dentin thickness, the lowest temperature increase was measured under a 3.5 mm-thick remaining dentin (6.44±1.56°C) and statistically significant (p<0.05), whereas the highest increase was significantly found with the 1.0 mm dentin thickness (11.00±2.68°C) (p<0.05). Differences in the mean temperature increases detected for the dentin thicknesses of 2.0 (9.77±2.62°C) and 3.0 mm (9.17±2.48°C) were not significant (p>0.05).
The interaction between the factors of light-curing unit and remaining dentin thickness is presented in Table 2. For all the remaining dentin thicknesses, LED produced significantly higher temperature increases when compared with QTH. The comparison among different remaining thicknesses in the same light-curing unit revealed that temperature increases were similar for 2 and 1 mm, and 3 and 2 mm for the LED unit, while the halogen light values were similar for 3 and 2 mm. Temperature increases were similar for LED/3.5 mm dentin thickness and halogen/3 and 2 mm dentin thickness.
Table 2. Mean values and standard deviations of temperature rise (°C) induced by the light-curing units in the different remaining dentin thicknesses.| 3.5 mm | 3 mm | 2 mm | 1 mm | |
| LED | 7.38 (0.92)b | 10.91 (2.00)d | 11.88 (1.24)d,e | 12.87 (1.09)e |
| Halogen | 5.49 (1.53)a | 7.41 (1.48)b | 7.66 (1.76)b | 9.14 (2.49)c |
*Different superscript letters indicate statistical difference at 5% level
There were no significant differences between the temperature increases achieved during photopolymerization of the adhesive with LED or QTH; however, temperature increase values registered during photopolymerization of each composite resin increment were statistically superior for the LED unit. Figure 1 depicts the behavior of temperature throughout the restorative process. LED always yielded higher temperatures than the halogen light. After curing each increment, there was a significant increase in temperature in the case of LED curing; however, this behavior was different for the halogen light as there was no significant increase after the third curing temperature.
Figure 1. Variation in the temperature recorded at each layer cured in the remaining 3.5 mm (0.5 mm enamel and 3.0 mm dentin); in 3 mm dentin; in 2 mm dentin and in 1 mm dentin. 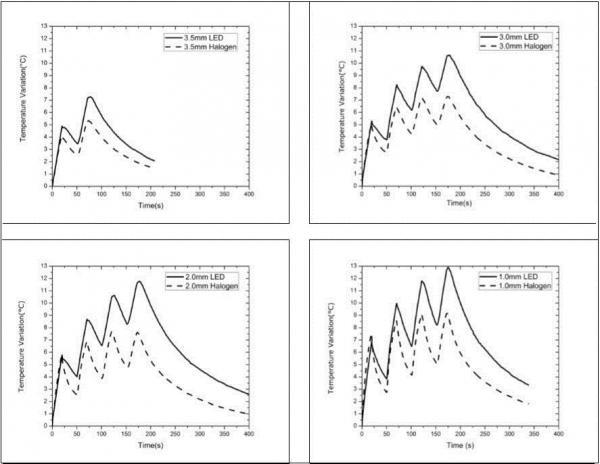
The spectral emission of the LED and Halogen lights are displayed in Figure 2. The maximum irradiance in the blue spectral region (400-500nm) for both sources is similar, around 1000 µW/cm2nm, while the halogen light has a broader emission than the LED source and an additional radiation at 600nm and 850nm.
Figure 2. Spectral irradiance of the LED and Halogen light.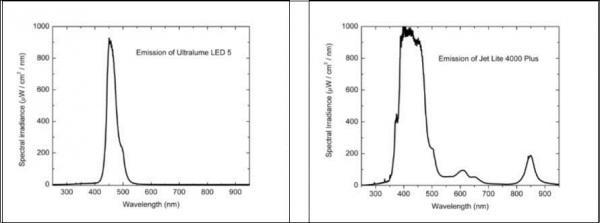
When considering the different groups studied, an increase in temperature exceeding 5.5°C was only observed during the second photopolymerization for all thicknesses except the specimens with a 1mm of thickness. However, there was a sharp increase in temperature right from the first curing for remaining 1 and 2mm, with a temperature increase of almost 13°C at the end of the procedure.
Discussion
Temperature increase within the pulp chamber can be induced by cavity preparation, exothermic reaction of cements and restorative materials, or heat generated by light-curing units. The amount of heat generated by light- curing units is related to the wavelength, power density of the emitted light and duration of thermal stimulus22.
In the present study, cavity restorations using light-activated composite resins caused a significant temperature increase as measured at the roof of the pulp chamber. This fact is the result of the energy output from the light-curing units and the exothermic chemical reaction taking place in the composite resin itself23. However, the most significant source of heat during polymerization of a light-activated composite comes from the curing unit and not from the material itself13, 24.
Another important factor observed in this present study is that, in all the studied groups, there was a considerable increase in temperature (greater than 5.5°C for most groups). This could probably affect the cells of the pulp tissue, leading to an irreversible inflammatory process or even pulpar necrosis20,while also potentially promoting dental sensitivity after treatment.
The results of the current study indicate that the temperature increase was significantly higher in the case of the LED curing unit, corroborating previous studies25, 26, 27. LED units emit more specific wavelengths, which are closer to the absorption spectrum of camphoroquinone, when compared with the conventional halogen light5,9. This result could encourage better use of energy equipment in the photoactivation of camphoroquinone27, consequently providing a higher degree of composite conversion. This curing, in turn, could occur more quickly, thus resulting in a significant temperature increase23.
According to Figure 2, both the LED and halogen lights presented similar spectral emissions in the region where camphoroquinone absorbs. The halogen light displays additional radiation near 600 and 850nm, a finding not observed for LED. 21, 28 Thus, the temperature values measured in this present study originated from two different heat sources; the first was the direct absorption of light and conversion to temperature increase, and the second was the heat generated by the exothermic reaction of composite photoactivation. Therefore, it is not possible to correlate temperature increase with spectral emission only.
The thermal variations occurring during light curing were dependent on the remaining dentin thickness, since temperature increase was inversely proportional to dentin thickness, which is due to the low thermal conductivity of this substrate17.
When analyzing the temperature reached during each photoactivation separately, the highest thermal variation was observed during the photopolymerization of the adhesive, which was the first to be performed and started without any residual heat accumulated from a previous photoactivation. Moreover, the thickness of the sample was significantly lower during the irradiation of the adhesive when compared with the situation achieved after composite resin curing.
Previous studies24,29have shown that the temperature increases is proportional to the composite thickness decreases. Thus, it might be speculated that the insertion of a small increment of composite and/or a curing unit with low light intensity should cause lower thermal stress on the pulp tissue10, indicating that the incremental technique provides for a lower temperature increase. However, the present study did not confirm this statement, as temperature values became higher after successive photoactivations, which was more evident for the LED curing unit, which resulted in a gradual increase throughout curing as more heat accumulated after each photopolymerization. Moreover, decreasing the depth of resin insertion did not avoid heat generation, regardless of the thickness of the resin increments.
Comparing the present results with the data found in the literature is difficult because most of the previous studies12,22,24,27,30,31evaluated thermal variations during composite photopolymerization in different remaining dentin thicknesses and/or composite insertions performed with only one photoactivation, which does not take heat accumulation throughout the restorative procedure into consideration, when at least two photoactivations are necessary (both adhesive and composite photopolymerizations). However, it is also necessary to consider the use of new equipment for curing, mainly due to the energy achieved by those devices. Due to the specificity of the wavelength of light emitted by LED, it is mandatory to rethink its use in a high energy density setting, since this study has shown that LEDs can generate heat increases much higher than 5.5°C. Thus, it is necessary to work with pulsed energy or even medium intensity energy for LED curing units.
Conclusions
Temperature increase is influenced by the type of light-curing unit and the thickness of the remaining dentin, with the highest temperature elevations produced by LED through 1 mm dentin. The number of photoactivations might affect temperature transmission, as an elevation in temperature was observed after every photoactivation. In all cases, there was an increase of over 5.5°C, with a maximum value of 14°C achieved with the LED curing unit, since the photoactivations generated high residual heat.
Acknowledgements
The authors are grateful to Prof. Dr. Patrícia Petromilli Nordi Sasso Garcia for allowing the use of the light-curing unit LED. This study was supported by The State of Sao Paulo Research Foundation (FAPESP) and the National Council for Scientific and Technological Development (CNPq).