
Intestinal Malrotation in a Suspected Celiac Disease Patient: A Case Report
- Open Access
- Peer Reviewed
- Similarity Checked
- CC BY 4.0
Abstract
Intestinal malrotation is the incomplete rotation of the midgut during embryogenesis. The reported prevalence is 1 in 500 live births, however some studies report a prevalence as high as 1% of the population1, 2. Traditionally it is though as a disease of the pediatric population presenting as bilious emesis during the first year of life but can present with different symptoms even in adulthood.
Presentation in older populations tends to be atypical, chronic abdominal pain, nausea and diarrhea being the most commonly reported symptoms 3. However, as these symptoms accompany almost all-gastrointestinal pathology it is difficult to determine if abnormalities of rotation and fixation of the intestine are the cause for the symptoms in a given patient given its relative rarity. It therefore is important to have a high index of suspicion in patients with non-specific gastrointestinal symptoms. We report laparoscopic management of a patient with abnormal rotation/fixation who was treated for many years as celiac disease (CD). Celiac disease is an immune mediated systemic disorder elicited by gluten in genetically susceptible individuals4. It can present as chronic abdominal pain, chronic diarrhea, failure to thrive, weight loss, stunted growth, distention and fatigue. His symptoms immediately resolved after surgery.
Article Information
- Received
- Accepted
- Published
Academic Editor: MariaGiovanna Cantone, IRCCS Centro Neurolesi Bonino Pulejo, Via Provinciale Palermo, Contrada Casazza, 98124 Messina, Italy.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Gustavo Romero-Velez, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Sathya Prasad Burjonrappa, Department of pediatric surgery, Children’s Hospital at Montefiore —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Background
Intestinal malrotation is the incomplete rotation of the midgut during embryogenesis. The reported prevalence is 1 in 500 live births, however some studies report a prevalence as high as 1% of the population1,2. Traditionally it is though as a disease of the pediatric population presenting as bilious emesis during the first year of life but can present with different symptoms even in adulthood.
Presentation in older populations tends to be atypical, chronic abdominal pain, nausea and diarrhea being the most commonly reported symptoms3. However, as these symptoms accompany almost all gastrointestinal pathology it is difficult to determine if abnormalities of rotation and fixation of the intestine are the cause for the symptoms in a given patient given its relative rarity. It therefore is important to have a high index of suspicion in patients with non-specific gastrointestinal symptoms. We report laparoscopic management of a patient with abnormal rotation/fixation who was treated for many years for celiac disease (CD). Celiac disease is an immune mediated systemic disorder elicited by gluten in genetically susceptible individuals4. It can present as chronic abdominal pain, chronic diarrhea, failure to thrive, weight loss, stunted growth, distention and fatigue. His symptoms immediately resolved after surgery.
Case Presentation
A 16 year old male was referred to the gastroenterologist for evaluation of poor weight gain and short stature (weight and height bellow the third percentile). Prior evaluation by the pediatric endocrinologist including thyroid function panel was noted to be within normal limits.
Upon presentation to gastroenterology, he reported no other associated symptoms other than stool frequency. However, on detailed questioning he mentioned that he had been unable to eat a full meal for as long as he could remember. On exam it was noted to be a thin adolescent with an otherwise normal physical exam. Blood work including CBC, BMP, LFTs all were unremarkable. Inflammatory bowel disease was ruled out having normal iron profile, CRP, albumin and stool calprotectin.
Upper endoscopy and colonoscopy were performed with no abnormal findings. Duodenal biopsy showed mild increased intraepithelial lymphocytes with normal villous architecture concerning of celiac disease, however anti tissue transglutaminase (TTG) and deamidated forms of gliadin peptides (DGP) were negative. At this time a trial of gluten free diet was attempted with mild improvement in his weight.
As part of the workup, an enterography magnetic resonance imaging (MRI) was done and showed non-rotation with the small bowel and colon in the right and left abdomen, respectively (Figure 1). A complementary upper gastrointestinal series (UGIS) was requested and the duodenal jejunal junction was abnormally located confirming malrotation (Figure 2).
Figure 1. MRI showing non rotation
Download figure
Figure 2. UGIS showing malrotation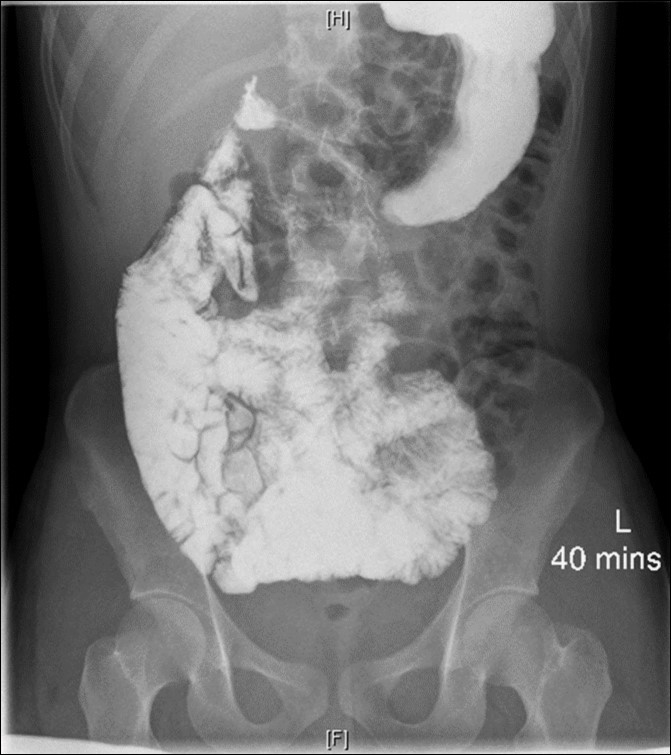
Download figure
The patient was then referred to the pediatric surgery clinic, where upon further questioning he endorsed to have early satiety for as long as he could remember. Surgical intervention was discussed with the patient and his family.
Method
A diagnostic laparoscopy was done showing malrotation with Ladd’s bands constricting the duodenum. Laparoscopic Ladd’s procedure was performed (Figure 3). A three port technique was used. Harmonic scalpel ™ (Ethicon Endosurgery) was used as the energy source to divide the bands. The appendix/cecum that was located in the midline suprapubic area was mobilized by continuing to divide abnormal mesenteric attachments and appendectomy was performed. At completion, small bowel was positioned to the right and large bowel positioned to the left. The duration of surgery was around 100 minutes. Patient had uneventful postoperative course and was discharged on postoperative day 2
Figure 3. a) diagnostic laparoscopy showing Ladd’s bands b) liberation of the duodenum after the Ladd’s procedure with the small bowel to the right of the abdomen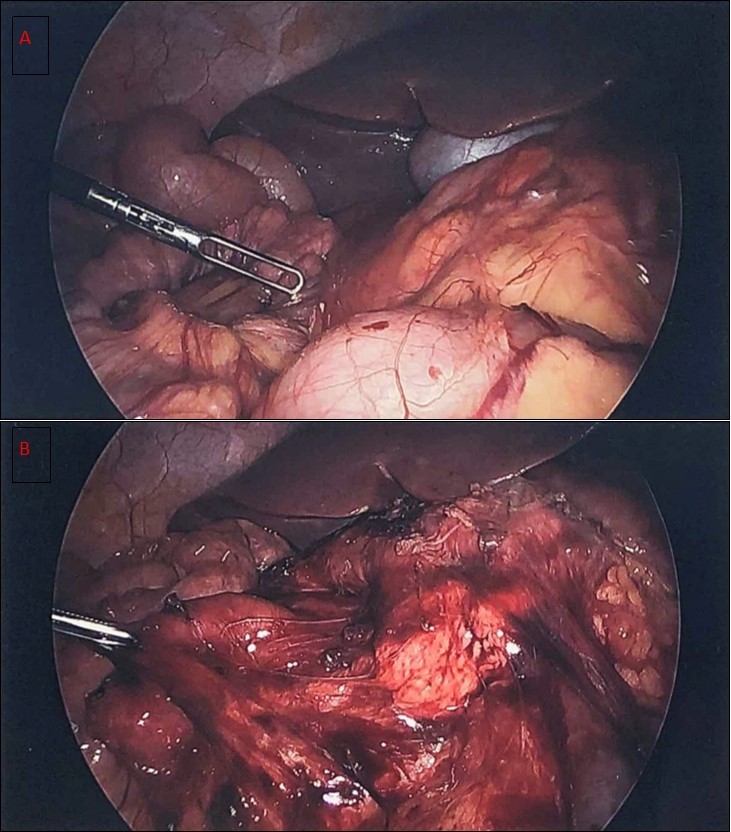
Download figure
Results
He was seen two weeks after and reported improve food tolerance. At three months follow up he has shown a weight gain of nearly 10 pounds. His early satiety and poor weight gain and short stature could be attributed to the delayed diagnosis of his malrotation.
Discussion
During fetal development the midgut rotates 270 degrees counterclockwise around the superior mesenteric artery (SMA), giving place to normal rotation5. This results in the duodenal-jejunal junction to the left of the spine, the duodenum posterior to the SMA, the mesentery of the small bowel going from the left upper quadrant to the right lower quadrant and the cecum fixed to the right lower quadrant. Malrotation encompasses a spectrum of conditions from non-rotation, atypical malrotation to true malrotation with a narrow mesentery6.
A typical rotation is defined as the ligament of Treitz at or to the left of the midline and below the level of the pylorus with or without a mobile or high-riding cecum. Typical malrotation is that in which the ligament of Treitz is absent or to the right of the midline1. Symptoms are usually produced by the duodenal compression by Ladd’s bands, associated duodenal atresia or volvulus secondary to a narrow mesentery.
It is estimated that up to 1% of the population is affected with some degree of the condition2. Traditionally it is thought that the majority of the cases are diagnosed during the first year of life. A retrospective study of intestinal malrotation showed that 69% of the patients were older than 1 year of life, with 48% older than 18 years old3.
The classic symptom of the newborn is bilious emesis, present in 93% of the cases3. As the presence of volvulus can potentially lead to death it has to be assumed that bilious emesis in a newborn is malrotation until proven otherwise. In older population emesis is not as common and most of the patients present with chronic abdominal pain.
Other reported symptoms are diarrhea, occult gastrointestinal bleeding, protein-losing enteropathy, abdominal distention, early satiety, failure to thrive or malnutrition7. Symptoms can be vague and present for years before a diagnosis is made. Nowadays, malrotation is also increasingly being diagnosed in asymptomatic patients1.
Our case shows an atypical presentation of malrotation with nonspecific symptoms of failure to thrive and stool frequency. Given the presence of intraepithelial lymphocytes on the duodenal biopsy pathology, it was suspected to have CD. However, the TTG and DPG antibodies were negative which have a reported sensitivity of more than 95%4. It is important to consider surgical intervention even in patients diagnosed with ‘non rotation’ as their symptoms may be attributable to abnormal bands.
The diagnosis is usually pointed out in radiologic studies. The absence of the colon on the right lower quadrant can suggest the diagnosis, however plain radiographs are not sensitive nor specific for the diagnosis of malrotation. Inversion of the SMV/SMA can be found on ultrasound but these have not been proven to be superior to an UGIS1. UGIS is still considered to be the gold standard for the diagnosis of malrotation. In our case, MRI suggested a non-rotation that was later proven to be malrotation on UGIS and confirmed by intraoperative findings. A retrospective study that included 145 patients who underwent UGIS and MRI showed a sensitivity of 100% and specificity of 92% for abnormal rotation when read by a pediatric radiologist8.
The treatment for malrotation was described by William Ladd in 1938. The Ladd’s procedure includes detorsion of the volvulus in case is present, lysis of the Ladd’s bands from the cecum to the right abdominal wall, widening of the small bowel mesentery to prevent volvulus, appendectomy and placing the small bowel to the right and colon to the left leaving the bowel on non-rotation9.
Multiple retrospective studies have showed the safety of laparoscopic Ladd’s procedure. This technique has improved pain, earlier full enteral feeds, shorter hospital stay and decreased number of postoperative small bowel obstructions compared to the traditional open approach10. The main pitfall of the laparoscopic approach is the increased number of volvulus post procedure which has been explained by the lack of adhesions formed during a minimal invasive approach. One should also have in mind that the reported conversion rate is 25%.
Conclusion
Malrotation can be seen more commonly than expected. Even though it has traditionally been thought as a disease of the infants, it can present later in life and tends to have non-specific gastrointestinal symptoms. Clinicians need a high index of suspicion when assessing patients with these symptoms. The gold standard for its diagnosis is the UGIS and the treatment of choice is the Ladd’s procedure which can be safely performed laparoscopically.
References
- 1.Graziano K, Islam S, Dasgupta R.(2015,Oct) Asymptomatic malrotation: Diagnosis and surgical management: An American Pediatric Surgical Association outcomes and evidence based practice committee systematic review. , J Pediatr Surg 50(10), 1783-90.
- 2.Garg A, Sudhanthar S.Okeafor C (2017,Dec) A 13 year old boy with abdominal pain and diarrhea. , Pediatr Rev 38(12), 572.
- 3.AM Nehra D Goldstein.(2011,Mar) Intestinal malrotation: varied clinical presentation from infancy through adulthood. , Surgery 149(3), 386-93.
- 4.Husby S, Koletzko S, Korponay-Szabó I R.(2012,Jan) European Sociey for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease.JPediatrGastroenterolNutr;54(1):. 136-60.
- 5.Kotobi H, Tan V, Lefèvre J, Duramé F, Audry G.Parc Y (2017,Jun) Total midgut volvulus in adults with intestinal malrotation. Report of eleven patients. , J Visc Surg 154(3), 175-183.
- 6.Morris G.Kennedy A Jr., Cochran W (2016,Apr) Small Bowel Congenital Anomalies: a Review and Update. , Curr Gastroenterol Rep 18(4), 16.
- 7.Langer J C.(2017,Feb) Intestinal Rotation Abnormalities and Midgut Volvulus. , Surg Clin North Am 97(1), 147-159.
- 8.Fay J S, Chernyak V.Taragin BH (2017,Oct) Identifying intestinal malrotation on magnetic resonance examinations ordered for unrelated indications. , Pediatr Radiol 47(11), 1477-1482.