
Evaluation of Co-morbidities among Different Chronic Obstructive Pulmonary Disease Phenotypes
- Open Access
- Peer Reviewed
- Similarity Checked
- CC BY 4.0
Abstract
Background:
Co-morbidities are associated with increasing risk of mortality, hospitalizations and costs of treatment in Chronic Obstructive Pulmonary Disease patients. Identification of Co- morbidities related to COPD phenotypes may guide individualized therapies and achieve better prognosis.
Methods:
A prospective study of one hundred ten patients of confirmed COPD diagnosis were carried out and divided into five different phenotypes with related co-morbidities. History taking, clinical examination, Chest X-ray, Computed chest Tomography, laboratory investigations, arterial blood gas, Echocardiography and Electrocardiography were done for all patients. St. George’s Respiratory Questionnaire, COPD assessment test (CAT score) and BODEx (BMI, FEV1, dyspnea and exacerbations) were used for assessment of disease impact on quality of life, severity, and exacerbation respectively.
Results:
Emphysema group were 31% among all cases with mean age 61.8±9.1, frequent exacerbator group and Chronic bronchitis phenotype were 18% with mean age 64.4±11.3, and 48.8±9 respectively. COPD with bronchiectasis group were 19% with mean age 60.3±6 and Asthma COPD Overlap Syndrome (ACOS) were 12% with mean age 62.8±15.8. There was significant difference as regards age between different group of phenotypes P- value <0.001. There was significance difference in BODEx index and in (CAT) score among different COPD phenotypes P-value 0.020, 0.001 respectively. There was significant difference in all items of SGRQ among different COPD phenotypes P–value 0.001. Diabetes was commonly presented in 50 % ACOS cases, Ischemic heart disease was present more in Emphysema 22.9%, Osteoporosis was more in COPD with bronchiectasis 28.6%, Cor-pulmonale was more present in frequent excerbator 65%, and Anemia more common in COPD with bronchiectasis 23.8%. Depression was more common in frequent excerbator phenotype (45.0 %). Gastro-esophageal reflux was the most common co-morbidities (58 %) then cor-pulmonale 41.8%, systemic hypertension 40 % and pulmonary hypertension 28%.
Conclusion:
The presence of significant co-morbidities is important modifying risk factors for severity in COPD. They contribute to the overall severity in individual patients, have a major impact on quality of life, and major causes of hospitalization. Co-morbidities can be associated with any clinical phenotype.
Article Information
- Received
- Accepted
- Published
Academic Editor: Mohammad Reza, Pharmaceutical Research Center and Department of Physiology, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 M. Sh. Badawy,et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Correspondence: Mohamed Shahat Badawy, Department of Chest Diseases, South Valley University, Qena, Egypt. Phone: +20 11 1545 4856 —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Chronic obstructive pulmonary disease (COPD) is a common disease that severely threatens human health. As World Health Organization (WHO) has predicted, social and economic burden of COPD will rise to the fifth and COPD will become the third leading cause of death worldwide by 2030.1 COPD is a complex syndrome with pulmonary and extra-pulmonary manifestations. In the recent years, clinicians also proved that the heterogeneity of COPD is associated with different clinical outcomes including symptoms, exacerbations, responses to recommended therapy, decline of lung function and death.2
Generally, phenotype is any observed quality of an organism, like its morphology, development or behavior, as opposed to its genotype, which is the inherited instructions it carries, which may or may not be expressed.3However, only phenotypes associatedwith symptoms, prognosis, progressionand response to therapy are relevant in clinical practice. So, the term clinical phenotype in the field of COPD is defined as “a single or combination of disease attributes that describe differences between individuals with COPD as they relate to clinically meaningful outcomes symptoms, exacerbations, response to treatment, speed of progression of the disease or death.3
Adding to lung involvement, a lot of “co-morbidities” may present in patients with COPD such as cardiovascular disease, metabolic dysfunctions, and depressive disorders are more commonly present. A number of potential mechanisms linking COPD and co-morbidities have been hypothesis: The pro-inflammatory cascade,4,5,6 increased oxidative stress,7 increased arterial stiffness,8,9 catabolic state,10 and sedentary lifestyle.11 Patients with COPD are often “multi-system diseased patients,” presenting with different clinical pictures, with a poorer quality of life and outcomes,12 and a high disease-related burden.13,14 Therefore, the phenotype should be able to classify the patients into subgroups with a prognostic value that allow for determining the best therapy in order to achieve better clinical results.
Patients and Methods
This prospective study of phenotypes of chronic obstructive pulmonary disease and its co-morbidities was carried out on 110 patients (74 males and 36 females) with mean age (59.8±11.3), they were admitted to chest department of Qena university hospital from our outpatient clinic and emergency room during the period from January 2016 to December 2016.
Inclusion Criteria
1-Patients were diagnosed to have COPD after assessing the presence of chronic cough, sputum production, dyspnea or history of exposure to risk factors as smoking and fumes (post-bronchodilator ratio (FEV1/FVC<0.70).
2- Their age ≥ 40 years.
3-Patients presented with one or more co-morbidities diagnosed previously or on current medical therapy. Co-morbidity was confirmed by the physician through a detailed examination and investigations and medications or therapy specific to any disease. Self-reported diagnoses were not considered.
Exclusion Criteria
1-Patients presented with bronchial asthma with reversible airway obstruction or other lung diseases.
2-Young aged patients < 40 years.
All Patients in the Study Investigated Thorough
Medical History Including
Age, sex, occupation, residence.
Smoking history , type of smoking , smoking index.
History of exposure to biomass fuel, and other special habits .
History of chronic cough.
History of exertional dyspnea using (mMRC) dyspnea scale (Modified Medical Research Council) Questionnaire for Assessing the Severity of breathlessness.
History of other symptoms orthopnea, chest pain, fever, heamptosis, wheezes, palpation, epigastric pain, cyanosis, anorexia, loss of weight, muscle and bone pain.
Family history.
History of exacerbation, previous hospitalization and ICU admission and classification of exacerbation severity according to the intensity of the medical intervention required to control the patient's symptoms :-
Mild (treated with short acting bronchodilators only, SABDs)
Moderate (treated with short acting bronchodilators plus antibiotics and/or corticosteroids).
Severe (patients require hospitalization or visit emergency room) may be also associated with acute respiratory failure .
Quality of life determined using the St. George’s Respiratory
Questionnaire for COPD patients (SGRQ).15Using simple Arabic version of SGRQ-C translated and validated by (Mohamed MA, 2008).16 It is a standardized, self administered questionnaire for measuring impaired health and perceived quality of life in airways disease (COPD and asthma). It consists of 50 items divided into three domains: Symptoms, Activity and Impacts. A score is calculated for each domain and a total score, including all items, is also calculated. Low scores indicate a better quality of life.
BODEx index (BMI, FEV1, dyspnea and exacerbations) for assessment the COPD severity and predicts mortality, hospitalization, and exacerbation frequency .
CAT score (COPD assessment test also for assessment of COPD severity.
Thorough Clinical Examination Including
General examination (pulse, Blood pressure, temperature, respirtratory rate, JVP, lower limb edema, lymph node)
Chest examination (inspection, palpation, percussion and auscultation).
Investigations Including
Chest x ray (postero-anterior) .
Abdominal ultrasonography.
Pulmonary Function Tests (PFT):- Using spirometer (Microlab)
Micro lab spirometer pre and post-bronchodilation were performed in all study subjects and forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, peak expiratory flow (PEF), forced expiratory flow (FEF) 25, 50 and 75 values were recorded. Post-bronchodilator values (15 minutes after the administration of 400 μg salbutamol) were used for diagnosis of COPD (post-bronchodilator test FEV1/FVC<0.70). 17
Arterial blood gases (ABG):- is a test that measures the partial pressure of arterial oxygen (PaO2) and carbon dioxide (PaCO2), oxygen saturation (SO2) and acidity (PH) in arterial blood. (ABL800) .
Electrocardiography (ECG), and Echocardiography.
Laboratory investigations:- complete blood count (white blood cells ,red blood cells, hemoglobin, haematocrite and platelets), liver function tests alanine aminotransferase (ALT), aspartate aminotransferase (AST) and serum albumin), renal function tests (serum creatinine , urea), blood sugar, prothrombin time and concentration and serum electrolytes (potassium, sodium and calcium).
Computerized tomography (CT) scan for chest.
Statistical Analysis
Analysis of data was done by IBM computer using SPSS (statistical program for social science version 24.0) as follows:
Description of quantitative variables as mean, SD and range.
Description of qualitative variables as number and percentage. The Student’s t-test was used to compare the mean of continuous variables among different subsets of patients. Significant P<0.05 and highly significant P<0.01.
Results
In our study 110 COPD patients (74 males and 36 females), with mean age 59.8±11.3 divided into 5 different COPD phenotypes; (ACOS) were 12%, (Chronic bronchitis) 18%, (COPD with bronchiectasis) 19%, (Emphysema) 31% and (Frequent exacerbator) phenotype 18%. There was significant difference in age and sex between different phenotypes. The frequent exacerbator and ACOS were older than other phenotypes. Most of COPD phenotypes were prevalent in male but only (COPD with bronchiectasis) phenotype was prevalent more in female. There was significance difference in smoking status between COPD phenotypes. Current smokers were prevalent in Chronic bronchitis phenotype as shown in Table 1.
Table 1. Demographic data of different COPD phenotypes| Phenotypes | P. value | |||||||||||||
| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | ||||||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | |||||
| No. of cases | 14 | 20 | 21 | 35 | 20 | |||||||||
| Age | ||||||||||||||
| Mean ±SD | 62.8±15.8 | 48.8±9 | 60.3±6 | 61.8±9.1 | 64.4±11.3 | <0.001** | ||||||||
| Male | 12 | 85.7 | 18 | 90.0 | 5 | 23.8 | 28 | 80.0 | 11 | 55.0 | <0.001** | |||
| Female | 2 | 14.3 | 2 | 10.0 | 16 | 76.2 | 7 | 20.0 | 9 | 45.0 | ||||
| Smoking status | ||||||||||||||
| Current smoker | 7 | 50.0 | 17 | 85.0 | 3 | 14.3 | 17 | 48.6 | 9 | 45.0 | <0.001** | |||
| Ex-smoker | 5 | 35.7 | 1 | 5.0 | 0 | 0.0 | 11 | 31.4 | 6 | 30.0 | ||||
| Passive smoker | 2 | 14.3 | 0 | 0.0 | 12 | 57.1 | 5 | 14.3 | 4 | 20.0 | ||||
| Nonsmoker | 0 | 0.0 | 2 | 10.0 | 6 | 28.6 | 2 | 5.7 | 1 | 5.0 | ||||
| Special habits | ||||||||||||||
| Biomass fuel exposure | 1 | 7.1 | 0 | 0.0 | 11 | 52.4 | 4 | 11.4 | 5 | 25.0 | ||||
| Bird reader | 1 | 7.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||||
| Car fuels exposure | 0 | 0.0 | 2 | 10.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||||
| Drinker | 1 | 7.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | ||||
| Dust, fumes exposure | 0 | 0.0 | 0 | 0.0 | 1 | 4.8 | 0 | 0.0 | 1 | 5.0 | ||||
| Hashish smoker | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 5.0 | ||||
| Drugs | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 2.9 | 0 | 0.0 | ||||
| No | 11 | 78.6 | 18 | 90.0 | 9 | 42.9 | 30 | 85.7 | 13 | 65.0 | ||||
As regards pulmonary function tests of different COPD phenotypes, there was significance difference in all values except in FEF 25-75. The lowest parameters were recorded in frequent exacerbator followed by COPD with Bronchiectasis phenotypes as shown in Table 2.
Table 2. Spirometry in different COPD phenotypes| Phenotype | P. value | |||||
| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | ||
| Mean ±SD | (Mean ±SD) | (Mean ±SD) | Mean ±SD | (Mean ±SD) | ||
| FEV1 | 43.1±16.4 | 91.5±25.3 | 38.7±17.1 | 41.8±14.8 | 38.1±11.8 | <0.001** |
| FVC | 59.8±20.8 | 87.2±34.4 | 48.6±21.6 | 55.4±17 | 49±17.1 | <0.001** |
| PEF | 30.6±10.6 | 55.2±26 | 26.3±13.4 | 29±11.8 | 27.6±10.3 | <0.001** |
| FEVI/FVC | 58±5.6 | 79.5±12.5 | 58.9±9.9 | 59.6±11.5 | 59±7 | <0.001** |
| FEF25 | 1.7±0.8 | 3.8±2.6 | 1.4±0.9 | 1.7±0.9 | 1.7±0.8 | <0.001** |
| FEF50 | 1±0.6 | 3±2.2 | 0.9±0.5 | 1.2±0.7 | 1±0.5 | <0.001** |
| FEF75 | 0.6±0.5 | 1.6±1.3 | 0.7±0.4 | 0.7±0.4 | 0.6±0.4 | <0.001** |
| FEF25-75 | 0.9±0.5 | 2.4±2 | 2.2±6.2 | 1±0.6 | 1±0.5 | 0.248 |
| MVV | 57.6±19.1 | 101.4±65.9 | 43.8±24.7 | 59.3±24.6 | 49.9±17.6 | <0.001** |
There was significance difference in all items of St. George’s Respiratory Questionnaire of different COPD phenotypes. Symptoms score it was highest in (ACOS) followed by (Frequent exacerbator). Activity score, impact and total scores were highest in (Frequent exacerbator) then (COPD with bronchiectasis ) as shown in Table 3.
Table 3. St. George’s Respiratory Questionnaire of different COPD phenotypes| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | P. value | |
| Symptoms Score | 81.43±10.51 | 53.5±8.65 | 68.77±10.07 | 62.2±15 | 72.59±7.32 | <0.001** |
| Activity score | 51.53±5.22 | 0±0 | 89.59±10.67 | 78.2±17.89 | 93.98±8.63 | <0.001** |
| Impacts score | 60.4±6.52 | 10.72±5.25 | 63.09±17.24 | 52.44±22.4 | 75.36±19.95 | <0.001** |
| Total score | 60.78±4.04 | 14.57±3.23 | 71.99±11.77 | 61.7±17.47 | 80.88±13.17 | <0.001** |
There was significance difference in BODEx index (BMI, FEV1,dyspnea and exacerbations) and CAT score of different COPD phenotypes P-value 0.020 and <0.001 respectively. As shown in Figure 1, Figure 2
Figure 1. BODEX index of different COPD phenotypes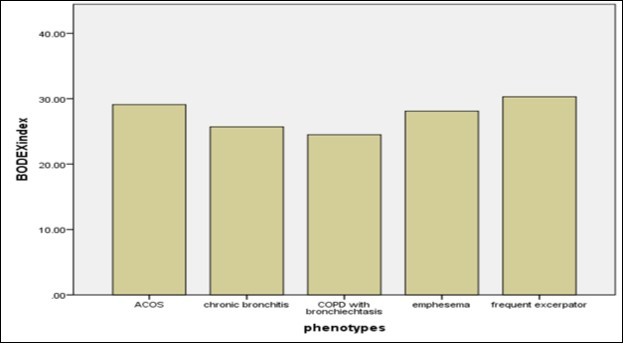
Download figure
Figure 2. CAT score of different COPD phenotypes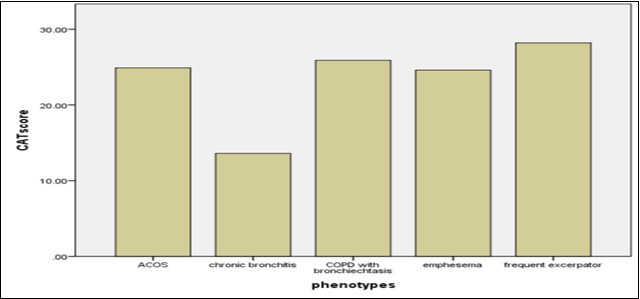
Download figure
The most common co-morbidities in all studied subjects was gastritis 58.2% of studied subjects, followed by cor-pulmonale 41.8%, Systemic hypertension 40.0 %, depression 25.5%, pulmonary hypertension 28.2%, and Diabetes Mellitus 19.1% as shown in Figure 3.
Figure 3. Co morbidities of all studied cases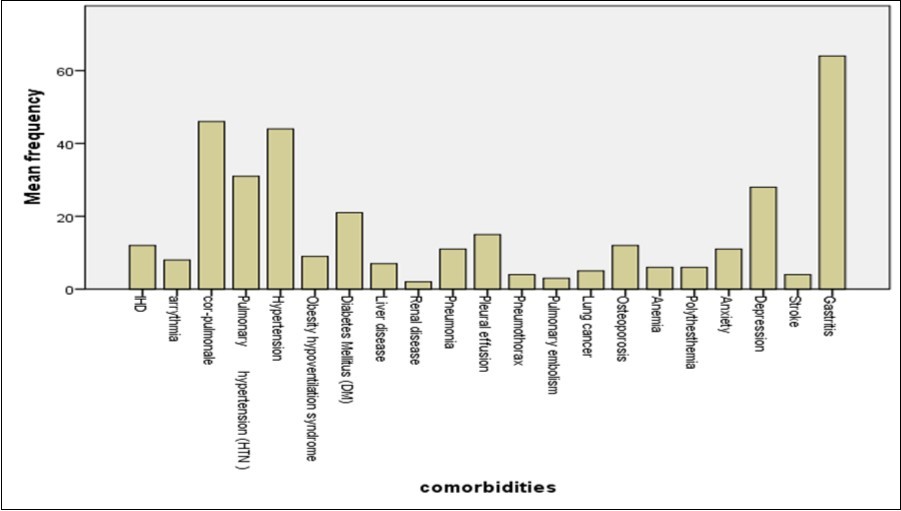
Download figure
More cases developed exacerbation in the last years, sever form of excerbation and ICU admission was related to frequent exacerbator phenotype with significant difference between phenotypes as regards one or two previous hospitalization and sever excerbation as shown in Table 4.
Table 4. Exacerbation frequency and previous hospitalization in last year of different COPD phenotypes| Phenotype | P. value | ||||||||||
| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | |||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | ||
| No. of exacerbation in last year | 11 | 78.6 | 18 | 90.0 | 15 | 71.4 | 32 | 91.4 | 20 | 100.0 | 0.054 |
| Mild to moderate | 7 | 50.0 | 8 | 40.0 | 9 | 42.9 | 16 | 45.7 | 2 | 10.0 | 0.071 |
| Severe | 4 | 28.6 | 3 | 15.0 | 4 | 19.0 | 14 | 40.0 | 17 | 85.0 | <0.001** |
| No of previous hospitalization | |||||||||||
| 1 | 7 | 50.0 | 8 | 40.0 | 9 | 42.9 | 16 | 45.7 | 2 | 10.0 | 0.002** |
| 2 or more | 4 | 28.6 | 3 | 15.0 | 4 | 19.0 | 14 | 40.0 | 17 | 85.0 | |
| ICU admission | 2 | 14.0 | 0 | 0.0 | 1 | 5.0 | 3 | 8.6 | 5 | 25.0 | 0.084 |
As regards evaluation of co-morbidities in different COPD phenotypes, there was significance difference in IHD (ischemic heart disease) it was more present in (Emphysema) 22.9 %, but less in other phenotypes. .Also there was significance difference in Cor-pulmonale, founded more in (Frequent exacerbator) 65.0 %, less in (ACOS) 4.3%. There was significance difference in diabeties mellitus, it was present in 50% of (ACOS), and 5.7 % in (Emphysema) cases.
There was significance difference in Osteoporosis co-morbidity, presented more in (Emphysema) 11.4 %, it was rare in (ACOS) and (Chronic bronchitis) There was significance difference in anemia, it was more in (COPD with Bronchiectasis) 23.8 %, and it was rare in (ACOS), (Chronic bronchitis) and (Frequent exacerbator). There was significance difference in depression co-morbidity, it was more in (Frequent exacerbator) 45.0%, less in both (Chronic bronchitis) and (ACOS). There was no significance difference in Arrhythmia, Pulmonary HTN, systemic hypertension, Obesity hypoventilation syndrome, Liver disease, Renal disease, pulmonary co-morbidities (Pneumonia, Pleural effusion, Pneumothorax, Pulmonary embolism, Lung cancer), Polythesthemia, Anxiety, Stroke and gastritis co-morbidities between phenotypes as shown in Table 5.
Table 5. Comorbidity in different COPD phenotypes| Phenotype | P. value | ||||||||||
| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | |||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | ||
| IHD (Ischemic heart disease ) | 0 | 0.0 | 1 | 5.0 | 0 | 0.0 | 8 | 22.9 | 3 | 15.0 | 0.033* |
| Arrhythmia | 0 | 0.0 | 0 | 0.0 | 1 | 4.8 | 5 | 14.3 | 2 | 10.0 | 0.228 |
| Corpulmonale | 2 | 14.3 | 4 | 20.0 | 11 | 52.4 | 16 | 45.7 | 13 | 65.0 | 0.008** |
| Pulmonary HTN | 2 | 14.3 | 3 | 15.0 | 7 | 33.3 | 10 | 28.6 | 9 | 45.0 | 0.190 |
| systemic Hypertension | 6 | 42.9 | 7 | 35.0 | 9 | 42.9 | 14 | 40.0 | 8 | 40.0 | 0.988 |
| Obesity hypoventilation syndrome | 1 | 7.1 | 3 | 15.0 | 2 | 9.5 | 0 | 0.0 | 3 | 15.0 | 0.226 |
| DM ( diabeties mellitus ) | 7 | 50.0 | 4 | 20.0 | 3 | 14.3 | 2 | 5.7 | 5 | 25.0 | 0.009** |
| Liver disease | 1 | 7.1 | 1 | 5.0 | 0 | 0.0 | 3 | 8.6 | 2 | 10.0 | 0.693 |
| Renal disease | 0 | 0.0 | 0 | 0.0 | 1 | 4.8 | 0 | 0.0 | 1 | 5.0 | 0.488 |
| Pneumonia | 2 | 14.3 | 2 | 10.0 | 2 | 9.5 | 4 | 11.4 | 1 | 5.0 | 0.921 |
| Pleural effusion | 0 | 0.0 | 3 | 15.0 | 0 | 0.0 | 8 | 22.9 | 4 | 20.0 | 0.067 |
| Pneumothorax | 0 | 0.0 | 2 | 10.0 | 1 | 4.8 | 1 | 2.9 | 0 | 0.0 | 0.444 |
| Pulmonary embolism | 0 | 0.0 | 1 | 5.0 | 0 | 0.0 | 2 | 5.7 | 0 | 0.0 | 0.540 |
| Lung cancer | 0 | 0.0 | 2 | 10.0 | 0 | 0.0 | 3 | 8.6 | 0 | 0.0 | 0.245 |
| Osteoporosis | 0 | 0.0 | 0 | 0.0 | 6 | 28.6 | 4 | 11.4 | 2 | 10.0 | 0.030* |
| Anemia | 0 | 0.0 | 0 | 0.0 | 5 | 23.8 | 1 | 2.9 | 0 | 0.0 | 0.002** |
| Polythesthemia | 1 | 7.1 | 2 | 10.0 | 0 | 0.0 | 3 | 8.6 | 0 | 0.0 | 0.404 |
| Anxiety | 0 | 0.0 | 0 | 0.0 | 4 | 19.0 | 4 | 11.4 | 3 | 15.0 | 0.187 |
| Depression | 1 | 7.1 | 2 | 10.0 | 8 | 38.1 | 8 | 22.9 | 9 | 45.0 | 0.032* |
| Stroke | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 2 | 5.7 | 2 | 10.0 | 0.315 |
| Gastritis | 9 | 64.3 | 9 | 45.0 | 15 | 71.4 | 17 | 48.6 | 14 | 70.0 | 0.275 |
As regards discharge from hospital with domcilliary oxygen was more in frequent excerbator phenotype and four cases died in emphysema phenotypes denoting the more severe form of phenotypes and more responsive phenotypes related to ACOS and chronic bronchitis as shown in Table 6.
Table 6. Discharge status of different COPD phenotypes| Phenotype | P. value | ||||||||||
| ACOS | Chronic bronchitis | COPD with bronchiectasis | Emphysema | Frequent exacerbator | |||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | ||
| Discharge status | |||||||||||
| Died | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 4 | 11.4 | 2 | 10.0 | 0.006** |
| Discharge with domiciliary O2 | 1 | 7.1 | 0 | 0.0 | 4 | 19.0 | 2 | 5.7 | 7 | 35.0 | |
| Discharge without O2 | 13 | 92.9 | 20 | 100.0 | 17 | 81.0 | 29 | 82.9 | 11 | 55.0 | |
Discussion
COPD is a major cause of chronic morbidity and mortality throughout the world; many people suffer from this disease for years, and die prematurely from it or its complications. Globally, the COPD burden is projected to increase in coming decades because of continued exposure to COPD risk factors and aging of the population.18 The classical COPD classification has been based on Forced Expiratory Volume in the first second (FEV1), but this alone is no longer accepted as a single parameter to define severity or to guide treatment (GOLD 2015) The updated Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations proposed treatment approach based on two additional parameters symptoms and exacerbations.1 So it is important to identify specific attributes in order to group the heterogeneous COPD into different phenotypes and guide treatment a patient therapeutic approach.
Several phenotypes have already been proposed but the understanding of which attributes define which groups of patient's remains challenges.19 Our study included 110 COPD patients (74 males and 36 females), with mean age 59.8±11.3 divided into 5 different COPD phenotypes 14 patients (ACOS) phenotype, 20 patients (Chronic bronchitis) phenotype, 21 patients (COPD with bronchiectasis) phenotype, 35 patients (Emphysema) phenotype and 20 patients (Frequent excerbator), it was compared with the study of (Jose´Luis et al.,)20 the authors studied 331 patients with mean age 66.3± 2.5 and were divided into 3 different COPD phenotypes only, 143 patients (Emphysema), 148 (Chronic bronchitis), 40 patients (ACOS).
In our study there was significant difference in sex between different COPD phenotypes with more prevalent in males except (COPD with bronchiectasis) phenotype was more prevalent in female this was in agreement with ( Jose´ Luis et al.,)20 stated that all phenotypes more prevalent in male. Also there was significance difference in smoking status between different COPD phenotypes. current smokers were more prevalent in (Chronic bronchitis) and (ACOS) phenotype, less prevalent in (COPD with bronchiectasis ) phenotype compared with same study there was no significance difference in smoking status among three different phenotypes this may be due to different study groups and numbers.
In our study there was significant difference in dypsnea (MMRC score) between different COPD phenotypes, most (ACOS) phenotype had Grade3 and Grade 4 50.0% , most (Chronic bronchitis) phenotype had Grade2 50.0%, most (COPD with bronchiectasis) phenotype had Grade4 47.6 % , most (Emphysema) phenotype had Grade3 48.6%, most (Frequent excerbator) phenotype had Grade4 75% and this is consistent with (Jose´ Luis et al.,) study who stated that there was significance difference in dypsnea (MMRC score), most phenotypes had Grade 2, (Emphysema) phenotype 37.8%,(Chronic bronchitis) phenotype 48% and (ACOS) phenotype 47.5% .
The most common co-morbidity present in our studied cases was gastritis followed by cor-pulmonale and hypertension and this is inconsistent with (Gianna et al.,).21 In our study there was no significance difference in number of exacerbation in last year of different COPD phenotypes, this was in agreement with ( Jose´ Luis et al.,)20
In our study there was significance difference between number of hospitalization in last year between different COPD phenotypes compared with (Jose´Luis et al.,) study there was no significance difference between number of hospitalization in last year. In our study there was no significance difference in number of ICU admission between phenotype, this was agreed with Beeh, Glaab et al., 2013)22 and ( Jose´Luis et al.,)20.
In our study there was significance difference in FEV1, FVC, FEV1\FVC ratio, FEV1, FVC values showed the lower value in (Frequent excerbator), and (COPD with Bronchiectasis) phenotype, FEVI/FVC ratio values showed the lower value in (COPD with Bronchiectasis), then (ACOS) phenotype. This in agreement with (Jose´Luis et al.,) study there was significance difference in FEV1 values, the (Emphysema) phenotype showed lower FEV1 values, in (Chronic bronchitis) and in (ACOS) phenotype. There was also significance difference in FEVI/FVC ratio, in (Emphysema) phenotype showed lower FEVI/FVC ratio value, in (Chronic bronchitis) phenotype, in (ACOS) phenotype, there was no significance difference in FVC.
In our study there was no significance difference in systemic hypertension between different COPD phenotypes. But there was significance difference in (Jose´Luis et al.,), it was more prevalent in (chronic bronchitis) phenotype 60.8%. In our study there was significance difference in diabeties mellitus, it was more common in (ACOS) phenotype. This was in agreement with (Jose´Luis et al.,) study there was also significance difference but it was more common in (chronic bronchitis). In our study there was significance difference in IHD (ischemic heart disease) co-morbidity between different COPD phenotypes, it was more common in (Emphysema) phenotype, Also there was significance difference in Cor-pulmonale co-morbidity, it was more common in (Frequent excerbator) phenotype 65.0 %. But in (Jose´Luis et al.,) study there was no significance difference, and it was more common in (ACOS) phenotype.
In our study there was no significance difference in (Obesity hypoventilation syndrome) co-morbidity between different COPD phenotypes. This was inconsistent with (Jose´Luis et al.,), as it was more present in (chronic bronchitis) phenotype. Our study and (Jose´Luis et al.,) study was consistent as regards no significance difference in arrhythmia and cerebrovascular disorder.
Osteoporosis was founded more in COPD with bronchiactasis, Emphysema and Frequent excerbator phenotypes with significant difference and this was in agreement with Gianna et al. 21
Our results showed that the highest association of co-morbidities is seen mostly in patients with severe COPD phenotypes. These findings were in agreement with Mahboub et al.,23 and Dal Negro et al.,24 who reported an association between the prevalence of comorbidity and COPD severity measured by a COPD assessment test score >10 or by Global Initiative on Obstructive Lung Disease stages, respectively, and disagreement with with findings of Watz et al.25
The co-morbidity related to heart dysfunction in frequent excerbator and emphysema phenotypes are particularly important predictors of increased risk of death in patients with COPD and indicate the importance of cardiovascular disease as a factor contributing to COPD mortality and this was consistent with Zielinski et al.,26
Conclusion
The presence of significant co-morbidities is one of the most important modifying risk factors for severity in COPD. They contribute to the overall severity in individual patients, have a major impact on quality of life, increase the risk of certain causes of mortality and of all-cause mortality and are major causes of hospitalization , Co-morbidities can be associated with any clinical phenotype. But we found that distribution of Co morbidities not much different between these phenotypes, gastritis was the most frequent co-morbidity in all phenotypes, then systemic hypertension and cor-pulmonale. But diabetes mellitus was more common in ACOS phenotypes, depression was more common in frequent excerbator phenotype.
References
- 1. (2017) Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis,Management and Prevention of Chronic Obstructive Pulmonary Disease ( reversied.
- 2.Han M K, Agusti A, Calverley P M, Celli B R, Criner G et al. (2010) Chronic obstructive pulmonary disease phenotypes: the future of COPD. , Am J Respir Crit Care Med 182(5), 598-604.
- 4.Agustí A, Edwards L D, Rennard S I.et al.(2012) Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Investigators. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One;7(5):e37483
- 5.Agustí A G, Noguera A, Sauleda J, Sala E, Pons J et al. (2013) Systemic effects of chronic obstructive pulmonary disease. , Eur Respir 21(2), 347-360.
- 6.Gan W Q, Man S F, Senthilselvan A, Sin D D. (2004) Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. 59(7), 574-580.
- 7.MacNee W. (2005) Pathogenesis of chronic obstructive pulmonary disease. Proc Am Thorac Soc;2(4): 258-266.
- 8.Sabit R, Bolton C E, Edwards P H. (2007) Arterial stiffness and osteoporosis in chronic obstructive pulmonary disease. , Am J Respir Crit Care Med 175(12), 1259-1265.
- 9.Maclay J D, McAllister D A, Mills N L. (2009) Vascular Dysfunction in chronic obstructive pulmonary disease. , Am J Respir Crit Care Med 180(6), 513-520.
- 10.Schols A M, Broekhuizen R, Weling-Scheepers C A, Wouters E F. (2005) Body composition and mortality in chronic obstructive pulmonary disease. , Am J Clin Nutr 82(1), 53-59.
- 11.Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó J M. (2007) Regular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease: a population-based cohort study. , Am J Respir Crit Care Med 175(5), 458-463.
- 12.Mannino D M, Higuchi K, Yu T C.(2015)Economic burden of COPD in the presence of comorbidities. , Chest 148(1), 138-150.
- 13.Gershon A S, Mecredy G C, Guan J, Victor J C, Goldstein R et al. (2015) Quantifying comorbidity in individuals with COPD: a population study. , Eur Respir J 45(1), 51-59.
- 14.Wacker M E, Jörres R A, Schulz H. (2016) for COSYCONET-consortium Direct and indirect costs of COPD and its comorbidities: results from the German COSYCONET study. , Respir Med 111, 39-46.
- 16. (1991) Questionnaire Respiratory Medicine; 85(B): 25-31.www.hrainc.net done by Mohamed mostafay Abd El Hady. MD; Professor of chest diseases. Assiut University;. , SGRQ Arabic 2008.
- 18.Lozano R, Naghavi M, Foreman K. (1990) Global and regional mortality from 235 causes of death for 20 age groups in. 2128.
- 19.Mathers C D, Loncar D. (2006) Projections of global mortality and burden of disease from2002t2030. PLoS Med ;. 3(11), 442.
- 20.Luis Jose.Lsquierdo-Alenso ,Antonio Martin et al.,(2013May) prevalence and characteristics of three clinical phenotypes of chronic obstructive pulmonary disease. , Respiratory Medicine; 107(5), 724-731.
- 21.Camiciottoli Gianna.Francesca Bigazzi, Chiara Magni,et al., (2016)Prevalence of comorbidities according to predominant phenotype and severity of chronic obstructive pulmonary disease. , Int J Chron Obstruct Pulmon Dis ; 11, 2229-2236.
- 22.Beeh K M, Glaab T, Stowasser S, Schmidt H, Fabbri L M et al. (2013) Characterization of exacerbation risk and exacerbator phenotypes in the POET-COPD trial. , Respir Res 14, 116.
- 23.Mahboub B, Alzaabi A, Iqbal M N. (2016) Co-morbidities associated with COPD in the Middle East and North Africa region: association with severity and exacerbations. , Int J Chron Obstruct Pulmon Dis 11, 273-280.
- 24.Dal Negro RW, Bonadiman L, Turco P. (2015) Prevalence of different comorbidities in COPD patients by gender and GOLD stage. , Multidiscip Respir Med 10(1), 24.