
Pilot Study: Impact of a Gluten-Free Diet on Symptoms and Severity of Fibromyalgia
Abstract
Fibromyalgia (FM) is a condition of chronic and widespread pain, with several associated symptoms. Previous studies suggested that gluten could influence the severity and frequency of FM symptoms. This work aimed to assess the impact of a gluten-free diet (GFD) in the symptoms and severity of this disease. Fourteen patients with previous FM diagnosis were kept on a gluten-free diet for eight weeks (Phase 1). After that, they were held on the gluten-free diet and received capsules of isolated rice protein (placebo) for seven days, followed by capsules containing 8.4g/day vital gluten for additional seven days (Phase 2). Questionnaires evaluating the number and severity of FM symptoms, the impact of FM on daily routine as well as inflammatory blood markers were assessed in each phase. Results showed that after eight weeks of GFD, we observed a reduction in the impact of FM on daily routine and number of symptoms and sensitive points. However, a seven days challenge with 8.4g of gluten did not worsen these symptoms or the inflammatory markers compared with the placebo challenge. We concluded that the gluten-free diet was associated with the attenuation of main symptoms and improvement of life quality in FM patients. Nonetheless, gluten challenge had no impact on those parameters, suggesting that gluten is not the major dietary component responsible for these improvements. Further studies are needed to elucidate the relationship between gluten intake and fibromyalgia.
Article Information
- Received
- Accepted
- Published
Copyright © 2020 Ana Carolina Garcia de las Ballonas Campolina
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Ana Carolina Garcia de las Ballonas Campolina, Department of Biochemistry and Immunology, Biological Sciences Institute, Federal University of Minas Gerais, Belo Horizonte, MG, Brazil —
Competing Interests
The authors have no conflicts of interest to declare.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
We would like to thank Mateus Leme City Hall for all the support for providing access to the patient's cohort. We thank Professor Dr. Alessio Fasano, from Mucosal Immunology and Biology Research Center (Massachusetts General Hospital, Harvard Medical School) for the HP genotyping, analyzes of serum cytokines, and final revision of the paper.
Citation:
Introduction
Fibromyalgia (FM) is a rheumatological syndrome mainly characterized by chronic diffuse musculoskeletal pain. Its etiology has not yet been well clarified, however, involve a disturbance in the processing of pain. Moreover, these patients often report other symptoms, such as fatigue and cognitive disorders 1, 2, 3, 4, 5, 6. Several extra-intestinal symptoms of FM, such as headache, arthralgia and myalgia, cloudy mind, and depressive mood, are similar to those seen in non-celiac gluten sensitivity (NCGS) patients 7, 8. NCGS is a disorder related to gluten intake, in people whose celiac disease (CD) and wheat allergy have been excluded, and that the adoption of a gluten-free diet leads to rapid remission of the symptoms, with the return of symptoms after gluten reintroduction 7, 8.
Some studies pointed to the improvement of FM symptoms after the adoption of a gluten-free diet 9, 10, 11, which gained popularity among professionals and patients. However, scientific studies evaluating the withdrawal of gluten as well as the impact of its reintroduction in FM patients are scarce. In this context, the objective of this study was to evaluate, in individuals with a prior diagnosis of FM, the impact of the gluten-free diet followed by the reintroduction of gluten on the symptoms and severity of FM.
Material and Methods
Group Selection
It was a single-blind controlled study in which the sample cohort was determined by convenience. The study was approved by the UFMG Research Ethics Committee (COEP), register 1.269.563, and registered in ClinicalTrials.gov (NCT03129906). This study was conducted from September 2015 to October 2016. Women over 18-year-old attending the Mateus Leme Clinical Specialty Center (Minas Gerais, Brazil) with the previous diagnosis of FM, according to American College of Rheumatology of 2010 3, were invited to participate and signed a written consent form. The exclusion criteria were positive serology for celiac disease (CD) or wheat allergy, autoimmune disease or other chronic diseases, use of anti-inflammatory agents, pregnancy, or lactation.
Study Design
`The study was divided into two phases: In Phase 1 (8 weeks), we initially enrolled seven women and evaluated the effect of a gluten-free diet on the quality of life and symptoms of FM. At baseline (week 0) and week 8, we evaluated anthropometric measurements, 72h food record, blood samples, and three questionnaires: Fibromyalgia Impact Questionnaire (FIQ), Symptoms Severity scale (SSS), Widespread pain index (WPI), (Figure 1). After the confirmation of the effects of a gluten-free diet on some FM symptoms in the first participants, the second group of 7 volunteers initiated the phase 1 protocol and, after, proceeded to the challenge phase (Phase 2). Since the results of the first seven volunteers in phase 1 were similar to those of the seven last volunteers (who passed to phase 2), we presented the data of the 14 volunteers together (Figure 2).
Figure 1. Experimental study design. Volunteers were kept on a gluten-free diet during Phase 1 and Phase 2. Abbreviations: WPI, Widespread pain index; SSS, Symptom severity scale; FIQ, Fibromyalgia impact questionnaire; FFQ, Food frequency questionnaire.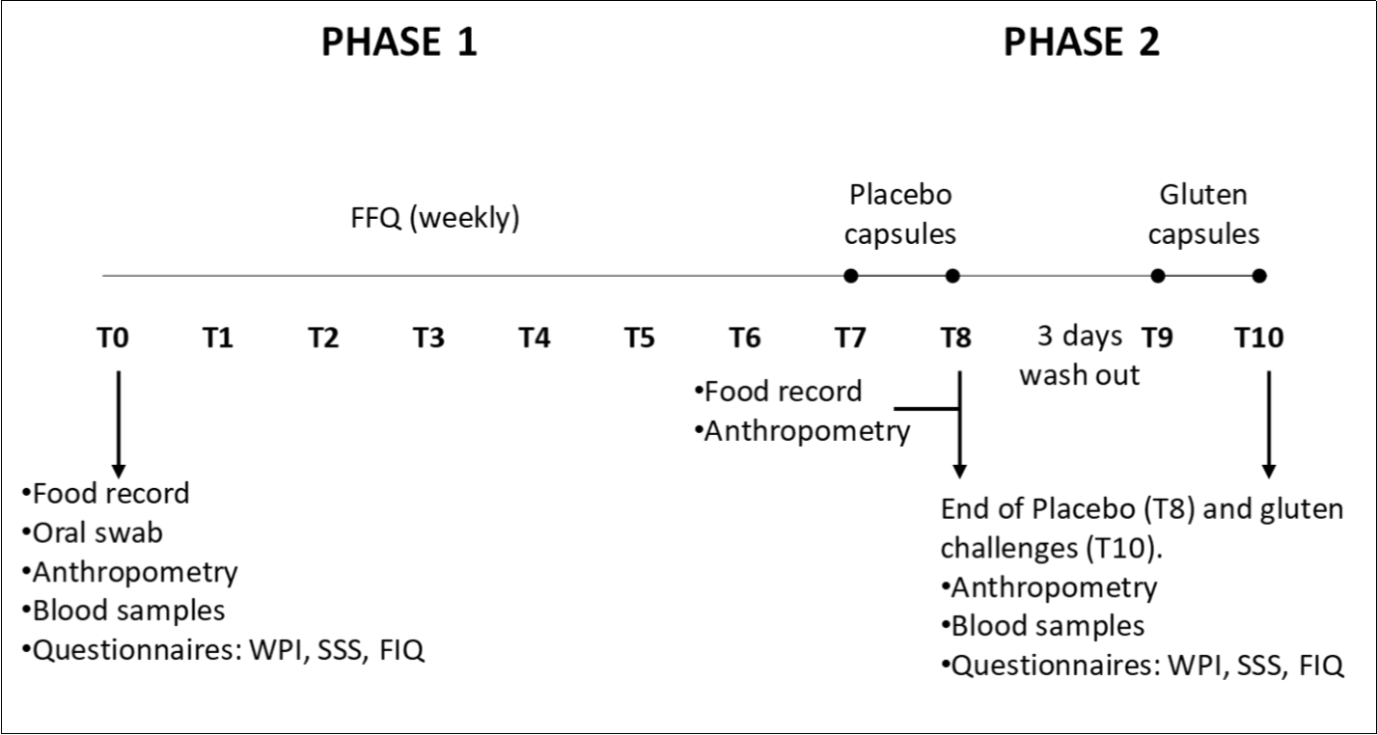
Download figure
Figure 2. Flow of patient recruitment and exclusion during the study. Abbreviations: ACR, American college of rheumatology; CD, celiac disease. Phase 1: Gluten-free period; Phase 2: Food challenge.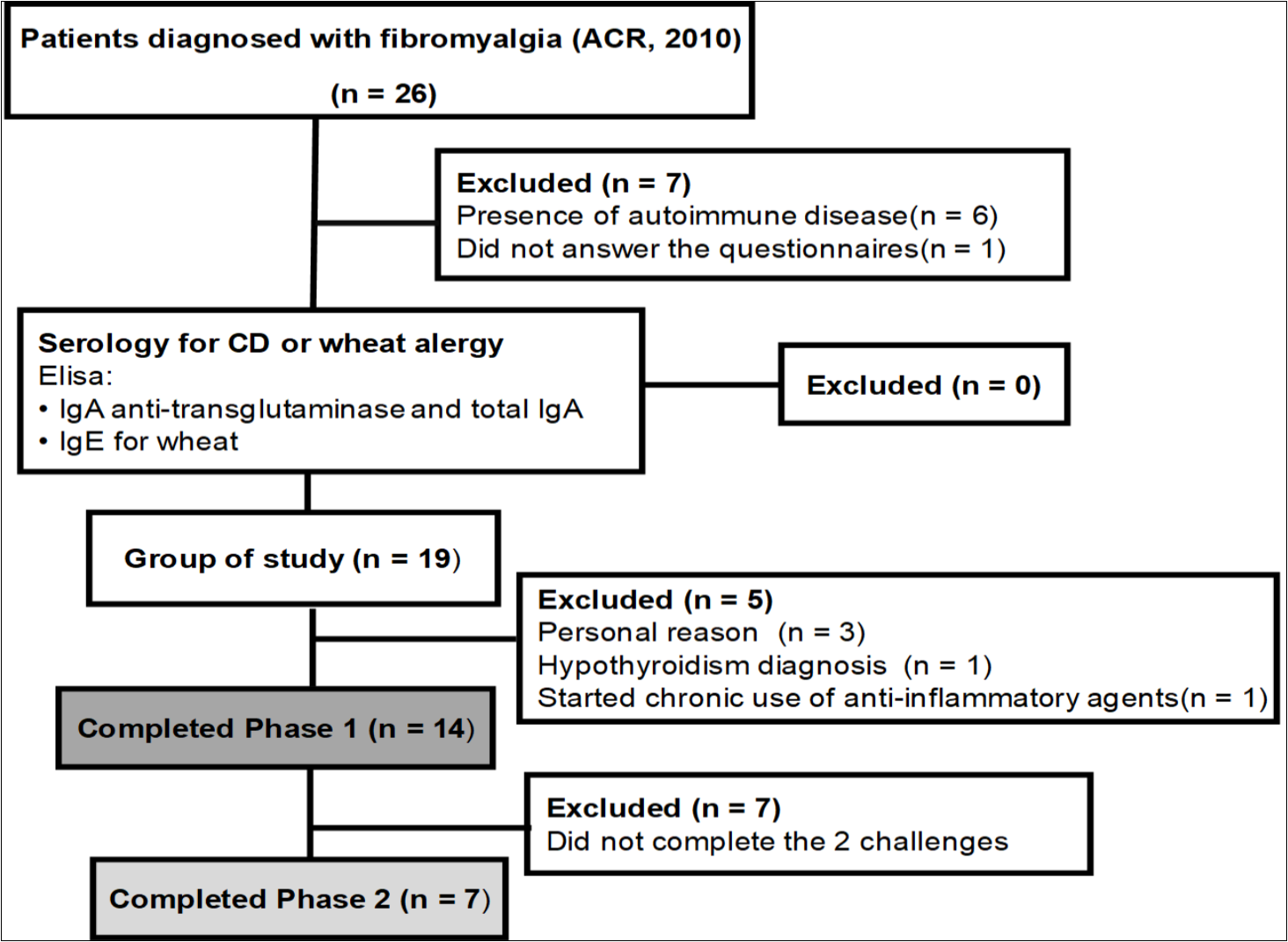
Download figure
In Phase 2 (placebo and gluten challenge), the 7 participants were kept in the gluten-free diet and took 12 placebo capsules daily (containing 6,4g of isolate rice protein in total) for one week. After a three days washout period, they were submitted to the second challenge, taking 12 capsules containing a total of 8.4 g of vital gluten daily for another week. The capsules containing gluten or placebo were encoded and indistinguishable. At the end of each challenge, blood was collected and FIQ, SSS, and WPI questionnaires evaluated (Figure 1).
All questionnaires assessing FM symptoms were applied related to the last seven days from the date of application. Patients received nutritional advice regarding the implementation of a gluten-free diet. The data was collected at the Specialty Center of Mateus Leme (MG/Brazil) and by telephone calls.
Questionnaires
The FIQ evaluates the impact of fibromyalgia on the diary routine through the evaluation of 10 different items. The result was given as the average of the ten items 12.
The SSS is used to quantify the severity of the FM symptoms. The final score is obtained by the sum of the severity score of 3 symptoms: 1-fatigue, 2-waking unrefreshed, and 3-cognitive symptoms and the number of FM symptoms present at that moment 3. For both questionnaires, the high score is associated with a high severity of the disease.
The 72h food record was evaluated for three days, on alternate days, and covering one day of the weekend. The volunteers received instructions about how to record daily intake 13. Subsequently, the records were reviewed and analyzed by a trained dietitian using the Avanutri Software (Brazil).
To evaluate participants' compliance with the gluten-free diet, the weekly Food Frequency Questionnaire (FFQ) was applied by the dietitian.
Blood Analysis and Genotyping
The blood was collected after 8h fasting, between 7 to 10 am. We analyzed total IgA (Phadia Uppsala Sweden), IgE for wheat (Beckman Coulter, BreaCa, US), IgA anti-transglutaminase (Orgentec Diagnostika Gmbh, Mainz Germany), the cytokines IL1ß, IL6, IL8 (R&D System, Minneapolis, MN, US) and the cytokines IL1RA, IL4, IL10 (U-Plex Assay - Meso Scale Diagnostics, Rockville, MD, US).Haptoglobin genotyping was done with specific primers designed in exon two and exon 5 of HP1 matching to exons 2 and 7 of HP2 amplified by high Fidelity PCR System. After PCR, the amplicons were run on a 1% agarose gel and read under a UV bulb. The size difference allowed differentiation of the two genotypes (HP1:2.5 KB and HP2:5.3 kb).
Statistical Analysis
Statistical analyses were performed using the software SPSS 19 (SPSS Inc., Chicago, IL, USA). Graphs were plotted at the software GraphPad Prism 5.0. The normal distribution of the data set was evaluated using the Shapiro-Wilk test. Parametric data were analyzed by Student's paired t-test and nonparametric variables by Wilcoxon Mann–Whitney test (2 groups). The Kruskal-Wallis test was used to compare the genotypes of haptoglobin with the changes in cytokines levels, FIQ, and the number of disease symptoms after a gluten-free diet. For those variables that presented p-values lower than 0.20 (FIQ, IL10, and IL8), a regression model was used to investigate a relation with the number of alleles of pre-haptoglobin 2 (HP2).
Results
Twenty-six patients selected from Specialty Center of Mateus Leme (MG/Brazil), met the criteria of ACR, 2010. Of these, six were excluded because they had an autoimmune disease, and one did not answer the questionnaires. None of the volunteers presented positive serology for CD (IgA anti- transglutaminase and total IgA) and wheat allergy (IgE for wheat). Therefore 19 patients were enrolled in the study. Five patients withdrew the study due to: personal reasons (n=3), hypothyroidism diagnosis during phase 1 (n=1), and chronic use of anti-inflammatory agents (n=1). The remaining 14 women that completed the phase 1 period (aged 41-62) presented the following associated disorders: arterial hypertension (n=7), orthopedic problems (n=3), and labyrinthitis (n=2). Some patients were underuse of drugs at the beginning of this study. Most of them were antihypertensive, antidepressants, or hypocholesterolemic agents. All drugs and posology were kept unchanged throughout the experimental period. Analgesics (dipyrone, paracetamol, ibuprofen, tramadol) were used only sporadically during the experimental period. Volunteers were advised to avoid the use of non-steroidal anti-inflammatory drugs throughout the study. None of them were in physiotherapy, and 7 (50%) practiced physical activity: hydrogymnastics 2 to 3 times a week (4 volunteers) or walking 2 to 3 times per week (3 volunteers). We didn't ask about cognitive compartmental therapy. None of them were in use of phytotherapy. The treatment was monitored by telephone and in individual meetings. All patients adhered to the gluten-free diet, according to the analysis of FFQ.
The Gluten-Free Diet Improved FM Symptoms (Phase 1)
Anthropometric parameters, body weight, body mass index (BMI), and abdominal circumference were unaltered during Phase 1 (Table 1). Caloric, protein, and lipids intake were similar over the experimental weeks (Table 2). However, at the end of week 8, carbohydrates and fibers intake were significantly reduced compared to the beginning of the study.
Table 1. Comparison of anthropometric measurements and blood levels cytokines during Phase 1.| Parameter | Initial | Final | p# |
|---|---|---|---|
| Anthropometry1 | |||
| Weight (kg) | 74.9 (± 15.9) | 74.5 (± 16.1) | 0.404 |
| BMI (kg/m2) | 30.6 (± 6.6) | 30.4 (± 6.6) | 0.356 |
| AC (cm) | 103.0 (± 12.8) | 102.3 (± 12.2) | 0.117 |
| BloodCytokines2 | |||
| IL1RA (pg/mL) | 1209.4 (703.4 – 5495.6) | 913.4 (476.8 – 4212.6) | 0.096 |
| IL1ß (pg/mL) | 5.7 (3.8 – 30.6) | 4.9 (3.7 – 37.4) | 0.127 |
| IL6 (pg/mL) | 14.7 (10.7 – 44.6) | 13.0 (10.4 – 48.0) | 0.463 |
| IL4 (pg/mL) | 0.1 (0.1 – 0.8) | 0.1 (0.0 – 0.8) | 0.275 |
| IL10 (pg/mL) | 130.0 (0.2 – 2.0) | 125.0 (0.7 – 2.3) | 0.703 |
| Parameter | Initial | Final | P |
|---|---|---|---|
| Food Intake | |||
| kcal/day | 1439.9 (± 468.1) | 1287.6 (± 450.2) | 0.357 |
| Protein (%) | 17.7 (± 1.6) | 20.0 (± 4.0) | 0.085 |
| Lipids (%) | 27.5 (± 7.2) | 33.6 (± 5.1) | 0.089 |
| Carbohydrate (%) | 52.5 (± 9.3) | 46.3 (± 6, 6) | 0.049 |
| Fibers (g) | 13.5 (± 4.5) | 8.8 (± 2.9) | 0.012 |
| Questionnaires Scores | |||
| Score on FIQ1 | 7.2 (± 1.2) | 5.5 (± 2.6) | 0.009 |
| Score at sss2 | 9.6 (± 1.7) | 7.0 (± 4.1) | 0.100 |
| Number of symptoms | 15.0 (± 3.7) | 10.4 (± 4.7) | 0.000 |
| WPI3 | 15.0 (± 3.7) | 10.9 (±4.6) | 0.014 |
Regarding the questionnaires, we found a significant reduction in FIQ scores, the number of FM symptoms, and the number of painful body points measured by the WPI. Nonetheless, a reduction in the severity of symptoms, assessed by SSS, was not significant (Table 2). These results suggested that the gluten-free diet improved FM by reducing the restrictions imposed by the disease and several painful points and symptoms, causing a reduction in the impact of FM on quality of life.
Next, we investigated if this improvement in the FM symptoms was associated with a reduction of serum inflammatory markers such as the pro-inflammatory cytokines IL1ß, IL1RA, IL6, and IL8, and the anti-inflammatory cytokine IL10 and IL4. No changes were seen in the levels of those cytokines comparing the initial and final of Phase1 (Table 1).
The patients were genotyped for haptoglobin genes to observe the presence of the HP2 allele, which codifies zonulin (pre-haptoglobin 2) and its possible association with the response to gluten withdrawal. The distribution of the HP allele was: 16.7% of patients have no HP2 allele (HP 1-1), 58.3% have only one allele (HP 2-1), and 25% have two alleles (HP 2-2). The regression model showed an association between the number of HP2 alleles and FIQ (Figure 3). It has been found that an average reduction of 2.0814 units occurs in the FIQ with the presence of the HP2 allele (p = 0.0257). The other variables analyzed did not show a significant difference.
Figure 3. Comparison of FIQ results after a gluten-free diet and number of HP2 alleles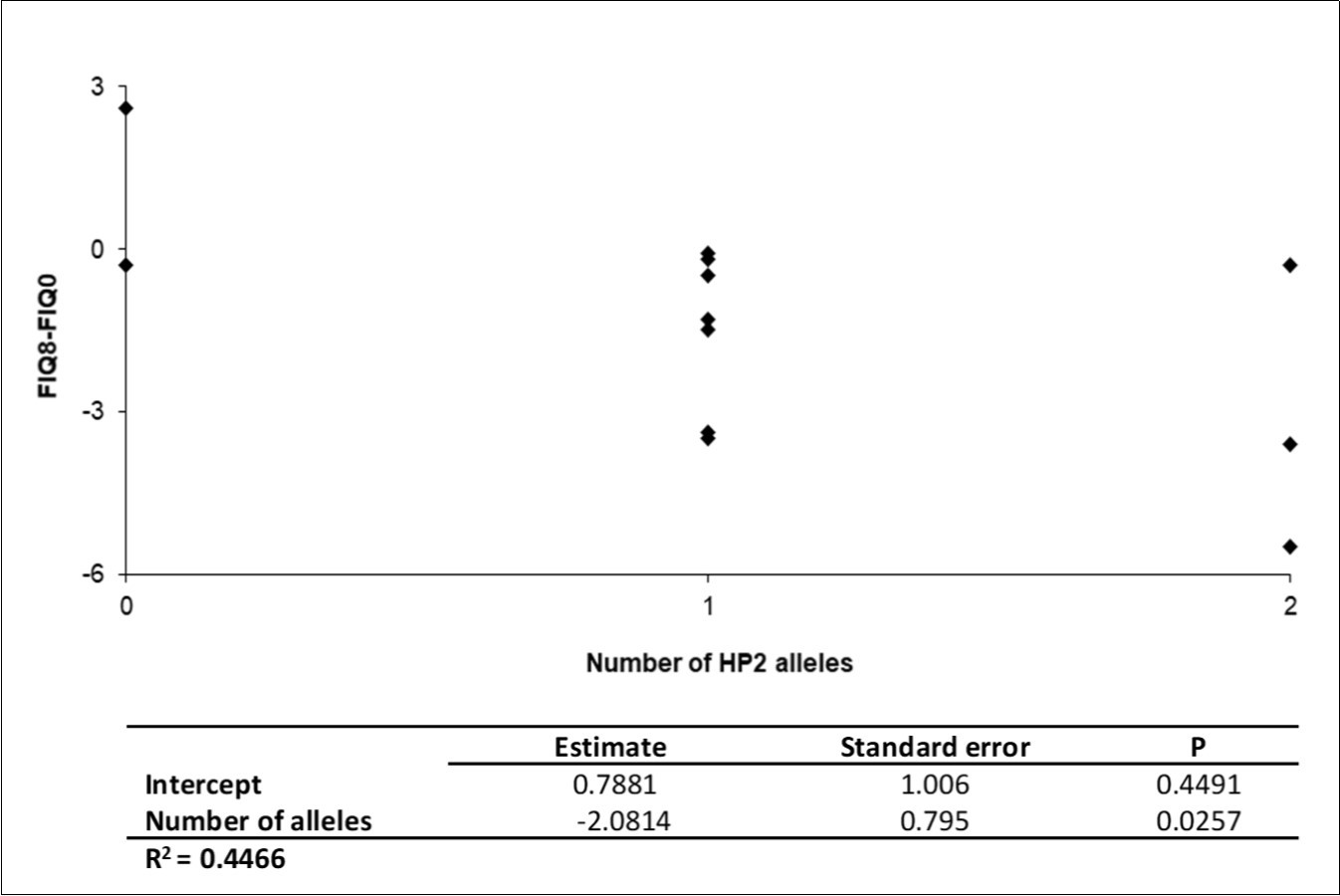
Download figure
Challenge with Placebo and Gluten Capsules did not Alter FM Symptoms (Phase 2)
Seven patients completed the two challenges of phase 2. None of the patients presented worsening of the symptoms with the reintroduction of the gluten compared to the placebo.
When the placebo was compared with the gluten challenge period, we did not find any changes in FM impact on daily routine, symptoms severity, or the number of painful body points as demonstrated by the results of FIQ, SSS, and WPI questionnaires (Table 3). Similarly, the blood level of the cytokines IL10, IL6, IL1β, IL1RA, IL4 was unaltered after one week of gluten and placebo challenge (Table 3).
Table 3. Anthropometric evaluation, fibromyalgia questionnaire results, and blood cytokines concentrations, during Phase 2 (placebo and gluten challenges)| Parameter | End of the placebo challenge | End of the challenge with gluten | p# |
| Anthropometry1 | |||
|---|---|---|---|
| Weight (kg) | 6a8 (± 10.4) | 68.8 (± 10.0) | 0.974 |
| BMI3 (Kg/m2) | 28.0 (± 3.2) | 28.0 (± 3.2) | 0.993 |
| AC4 (cm) | 97.6 (± 10.3) | 97.5 (±12.5) | 0.940 |
| Questionnaires Scores1 | |||
| Score in FIQ5 | 4.8 (± 2.5) | 4.6 (± 3.0) | 0.636 |
| Score at SSS6 | 7.0 (± 4.1) | 5.7 (± 4.0) | 0.253 |
| Number of symptoms | 10.6 (± 5.5) | 9.4 (± 4.0) | 0.231 |
| VVPI 7 | 10.9 (± 4.6) | 11.1 (± 3.9) | 0.726 |
| Blood Cytokines2 | |||
| IL 1 RA(pg/mL) | 1209.4 (703.4 - 5495.6) | 1064.2 (576.1- 3507.0) | 0.219 |
| IL1ß (pg/mL) | 5.7 (3.8 - 30.6) | 5.56 (4.0 - 27.0) | 0.688 |
| IL6 (pg/mL) | 14.7 (10.7-44.6) | 14.25 (11.0 - 20.2) | 0.813 |
| IL4 (pg/mL) | 0.1 (0.1 - 0.8) | 0.3 (0.2 - 0.6) | 0.735 |
| IL10 (pg/mL) | 1.3 (0.2 - 2.0) | 1.70 (0.8- 2.0) | 0.823 |
Discussion
The main finding of our study was that the adoption of a gluten-free diet improved FM symptoms reduced painful points, and improved the quality of life in 12 of the 14 FM patients. Two patients showed an improvement in almost all evaluated questionnaires except for FIQ score (increased in one patient) and FM symptoms (increased in another participant). Nonetheless, gluten isolate challenge had no impact on those parameters, suggesting that gluten is not the major dietary component responsible for these improvements.
Several studies have evaluated the impact of a gluten-free diet on the nutritional and metabolic status 14, 15, 16, but only a few of them were addressed to FM patients. The reduction of caloric intake, irrespective of the gluten exemption seems to exert beneficial effects on the symptoms of fibromyalgia 17, 18. However, our patients presented constant caloric intake during the experimental period, discarding a possible influence of lower caloric intake as a cause of the beneficial effects of the gluten- free diet.
The exclusion of gluten-containing foods modified the dietary pattern, reducing the intake of fibers and carbohydrates, as demonstrated by the 72h food record. The reduction of bread and pasta and several recipes containing wheat flour could lead to a decrease in carbohydrates and fiber intake. These data agree with other studies showing that gluten-free products are commonly made up of low- grained starch and flours 14, 19, 20. Although protein intake was not changed during the gluten-free period, it is important to note that gluten-containing foods are not typical sources of protein. Moreover, gluten amino acid composition is poor, making its exclusion harmless for the total balance of body protein 21.
Previous experimental studies 22, 23 showed that isogenic mice (C57BL/6) receiving a gluten- containing diet presented an increase in body weight and adiposity associated with the rise of inflammatory markers and reduction of thermogenesis. In ours and other clinical studies 18, weight loss was not observed probably due to a less controlled environment in clinical studies (especially food choices and lifestyle) and human genetic diversity compared with isogenic mice kept in a controlled diet.
Experimental studies also described a pro-inflammatory effect of the gluten or its components 24, 25, 26, 27. FM has also been associated with a proinflammatory cytokine profile 28, 29, 30. Our cytokine analysis did not show any changes during the experimental period. The increase of inflammatory cytokines in patients FM cannot be seen in blood analysis. It is possible that the inflammatory effect of gluten could not be enough to change the circulating levels of these cytokines significantly or that it does not exert, in humans, the inflammatory effects observed in mice.
The regression model suggested that the presence of the HP2 allele is associated with a better response to the gluten withdrawal. Haptoglobin encodes for two alleles, of which HP2 carries a duplication of the 3rd and 4th exons 31. The allele HP2 codifies the HP2 pre-haptoglobin (also known as zonulin). This protein is described as a physiological modulator of tight junctions 32 and is released upon gut dysbiosis and gliadin stimulus 33. These results suggest that those patients carrying the HP2 allele will present more benefits with the gluten withdrawal due to a lesser zonulin release, reducing changes on intestinal barriers caused by zonulin. Nonetheless, due to the limited number of observations, futures researches are required to confirm that association.
Our results suggested an improvement of several indicators of the severity of FM with the adoption of a gluten-free diet. However, the one-week challenge with 8.4g of vital gluten had no impact on the analyzed parameters in the patients that completed Phase 2. The amount of gluten used in the challenge phase was chosen based on the average gluten intake data in Western countries 34 and agreed with the amount seen in previous studies 35, 36. Taken together, although the limited number of patients, our data suggest that a moderate intake of gluten for seven days, is not a major dietary component related to the fibromyalgia symptoms, even in a subset of patients responsive to gluten-free diets.
Other studies in the literature suggest improvement of FM symptoms after a gluten-free diet mostly in patients with duodenal lymphocytosis 9, 10. In a study 9, patients improved FM symptoms with a gluten and lactose restricted diet (in lactose-intolerant patients). However, these beneficial effects cannot be attributed solely to gluten because other nutrients from wheat and milk components, were also excluded. In patients with FM and irritable bowel syndrome, a gluten-free diet improved the symptoms only in those with duodenal lymphocytosis, with a minimal effect on those without lymphocytosis 10. The authors suggest that a gluten-free diet would be suitable only for patients with duodenal lymphocytosis.
Our results make clear the importance of the gluten challenge to corroborate with the possible improvement of the symptoms of FM with such diets. Without the challenge phase, there could be a misguided conclusion that the gluten exemption would have been the cause of the improvement seen in the first phase of the study.
The factors responsible for the improvement of the gluten-free diet requires further investigation. It may be the consequence of more frequent and closer interaction between health professionals and patients since the study does not present a placebo group maintained without a gluten-free diet. Many symptoms are unspecific or subjective, and so frequent contacts with the professionals involved in the research may have contributed to the improvement of the symptoms. Besides, the expectation of improvement with dietary modification may have contributed to the feeling of improvement 37.
The improvement of the symptoms with the gluten-free diet could also be due to the exclusion of other components such as fermentable oligo, di, monosaccharides, and polyols (FODMAPs), short- chain carbohydrates, present in the wheat and other foods 38. Some studies have shown the improvement of symptoms of patients with FM and in patients with IBS (one of the comorbidities that is part of the FM spectrum) related to the restriction of FODMAPs 39, 40. The study of Pimentel et al. 41 demonstrated an alteration of lactulose respiratory test in all the evaluated patients with FM. One possible hypothesis would be that the FODMAPs or other components of the wheat (such as the amylase-trypsin inhibitors) could worsen an existing framework of Small intestinal bacterial overgrowth (SIBO). The imbalance of the microbiota would lead to an increase in intestinal permeability and consequently to more significant input of dietary and microbial antigens, which could lead to activation of T-cells in patients with presence of a chronic inflammation even if low intensity or with some predisposition of failures in the mechanisms of immunoregulation on intestinal mucosa 42. In our study, SIBO was no evaluated, and we suggest that future researches with gluten free- diet and FM should also analyze SIBO in volunteers.
It can also be assumed that the amount of gluten administered in the challenge is small to trigger the symptoms of FM. The choice of the amount of gluten used in the challenge (about 8.4g/day vital gluten) was calculated from the average gluten intake in the population of Western countries 34 and in agreement with some published studies 35, 36. However, the effects of gluten on FM may be caused by excessive gluten intake and not by quantities considered normal.
Among the limitations of the current study is the lack of a control group, the absence of specific markers for the transgression of the diet, and the small sample size. More studies are needed in double-blind design controlled with larger sample size.
Conclusion
The gluten-free diet was associated with the attenuation of main symptoms and improvement of quality of live in this group of FM patients evaluated. Nonetheless, gluten challenge had no impact on those parameters, suggesting that gluten is not the major dietary component responsible for these improvements.
References
- 1.Heymann R E, Paiva EdS UNIFESP, UFPR Helfenstein Junior M, UNIFESP. (2010) Brazilian consensus on the treatment of fibromyalgia. Rev Bras Reumatol. 50(1), 56-66.
- 2.Cagnie B, Coppieters I, Denecker S, Six J, Danneels L et al. (2014) Central sensitization in fibromyalgia? A systematic revion structural and functional brain MRI. Semin Arthritis Rheum. 44(1), 68-75.
- 3.Wolfe F, Clauw D J, Fitzcharles M A, Goldenberg D L, Katz R S et al. (2010) The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken). 62(5), 600-10.
- 4.Macfarlane G J, Kronisch C, Dean L E, Atzeni F, Häuser W et al. (2016) EULAR revised recommendations for the management of fibromyalgia.
- 5.Sluka K A, Clauw D J. (2016) Neurobiology of fibromyalgia and chronic widespread pain. , Neuroscience
- 6.Jensen K B, Loitoile R, Kosek E, Petzke F, Carville S et al. (2012) Patients with fibromyalgia display less functional connectivity in the brain's pain inhibitory network. Mol Pain. 8, 32.
- 7.Hill I D, Fasano A, Guandalini S, Hoffenberg E, Levy J et al. (2016) . NASPGHAN Clinical Report on the Diagnosis and Treatment of Gluten-related Disorders. J Pediatr Gastroenterol Nutr 63(1), 156-65.
- 8.Caio G, Riegler G, Patturelli M, Facchiano A, DEM L et al. (2016) Pathophysiology of non- celiac gluten sensitivity: where are we now in 2016? Minerva Gastroenterol Dietol.
- 9.Isasi C, Colmenero I, Casco F, Tejerina E, Fernandez N et al. (2014) Fibromyalgia and non-celiac gluten sensitivity: a description with remission of fibromyalgia. Rheumatol Int. 34(11), 1607-12.
- 10.Rodrigo L, Blanco I, Bobes J, de Serres FJ. (2014) Effect of one year of a gluten-free diet on the clinical evolution of irritable bowel syndrome plus fibromyalgia in patients with associated lymphocytic enteritis: a case-control study. Arthritis Res Ther. 16(4), 421.
- 11.Garcia-Leiva J M, Carrasco J L, Slim M, Calandre E P. (2015) Celiac symptoms in patients with fibromyalgia: a cross-sectional study. Rheumatol Int. 35(3), 561-7.
- 12.Marques A P, Santos AMB USP, Assumpção A USP, USP. (2006) Validation of the Brazilian version of the Fibromyalgia Impact Questionnaire (FIQ). Rev Bras Reumatol. 46(1), 24-31.
- 13.Fisberg R M, SP Universidade de São Paulo, Marchioni DML Brasil, SP Universidade de São Paulo, Brasil. (2009) Colucci ACA, Universidade Presbiteriana Mackenzie B. Assessment of food consumption and nutrient intake in clinical practice. Arq Bras Endocrinol Metab. 53(5), 617-24.
- 14.Saturni L, Ferretti G, Bacchetti T. (2010) The gluten-free diet: safety and nutritional quality. , Nutrients 2(1), 16-34.
- 15.Salazar Quero JC, Espin Jaime B, Rodriguez Martinez A, Arguelles Martin F, Garcia Jimenez R et al. (2015) [Nutritional assessment of gluten-free diet. Is gluten-free diet deficient in some nutrient?]. An Pediatr (Barc). 83(1), 33-9.
- 16.Bonder M J, Tigchelaar E F, Cai X, Trynka G, Cenit M C et al. (2016) The influence of a short-term gluten-free diet on the human gut microbiome. , Genome Med 8(1), 45.
- 17.Senna M K, Sallam R A, Ashour H S, Elarman M. (2012) Effect of weight reduction on the quality of life in obese patients with fibromyalgia syndrome: a randomized controlled trial. Clin Rheumatol. 31(11), 1591-7.
- 18.Slim M, Calandre E P, Garcia-Leiva J M, Rico-Villademoros F, Molina-Barea R et al. (2016) The Effects of a Gluten-free Diet Versus a Hypocaloric Diet Among Patients With Fibromyalgia Experiencing Gluten Sensitivity-like Symptoms: A Pilot, Open-Label Randomized Clinical Trial. J Clin Gastroenterol.
- 19.Penagini F, Dilillo D, Meneghin F, Mameli C, Fabiano V et al.Gluten-Free Diet in Children: An Approach to a Nutritionally Adequate and Balanced Diet. , Nutrients 52013, 4553-65.
- 20.Vici G, Belli L, Biondi M, Polzonetti V. (2016) Gluten free diet and nutrient deficiencies: A review. Clin Nutr.
- 21.Pires C V, UFd Viçosa, MGdA Oliveira, ViçosaV UFd, Rosa J C et al. (2006) Nutritional quality and chemical score of amino acids from different protein sources. Food Sci Technol (Campinas). 26(1), 179-87.
- 22.Soares F L, R de Oliveira Matoso, Teixeira L G, Menezes Z, Pereira S S et al.Gluten- free diet reduces adiposity, inflammation and insulin resistance associated with the induction of PPAR-alpha and PPAR-gamma expression. , J Nutr Biochem 24(6), 1105-11.
- 23.Freire R H, Fernandes L R, Silva R B, Coelho B S, de Araujo LP et al.Wheat gluten intake increases weight gain and adiposity associated with reduced thermogenesis and energy expenditure in an animal model of obesity. , Int J Obes (Lond) 40(3), 479-86.
- 24.Vilasi S, Sirangelo I, Irace G, Caputo I, Barone M V et al. (2010) Interaction of 'toxic' and 'immunogenic' A-gliadin peptides with a membrane-mimetic environment. J Mol Recognit. 23(3), 322-8.
- 25.Sodhi A, Kesherwani V. (2007) Production of TNF-alpha, IL-1beta, IL-12 and IFN-gamma in murine peritoneal macrophages on treatment with wheat germ agglutinin in vitro: involvement of tyrosine kinase pathways. Glycoconj J. 24(9), 573-82.
- 26.Kaliszewska A, Martinez V, Laparra J M. (2016) Proinflammatory responses driven by non-gluten factors are masked when they appear associated to gliadins. Food Chem Toxicol. 95, 89-95.
- 27.Lammers K M, Khandelwal S, Chaudhry F, Kryszak D, Puppa E L et al.Identification of a novel immunomodulatory gliadin peptide that causes interleukin-8 release in a chemokine receptor CXCR3-dependent manner only in patients with coeliac disease. , Immunology 132(3), 432-40.
- 28.Uceyler N, Valenza R, Stock M, Schedel R, Sprotte G et al. (2006) Reduced levels of antiinflammatory cytokines in patients with chronic widespread pain. Arthritis Rheum. 54(8), 2656-64.
- 29.Sturgill J, McGee E, Menzies V. (2014) Unique cytokine signature in the plasma of patients with fibromyalgia. J Immunol Res. 938576.
- 30.Uceyler N, Hauser W, Sommer C. (2011) Systematic review with meta-analysis: cytokines in fibromyalgia syndrome. BMC Musculoskelet Disord. 12-245.
- 31.Maeda N, Yang F, Barnett D R, Bowman B H, Smithies O. (1984) . Duplication within the haptoglobin Hp2 gene. Nature 309(5964), 131-5.
- 32.Tripathi A, Lammers K M, Goldblum S, Shea-Donohue T, Netzel-Arnett S et al. (2009) Identification of human zonulin, a physiological modulator of tight junctions, as prehaptoglobin-2. Proc Natl Acad Sci U S A 106(39), 16799-804.
- 33.Fasano A. (2011) Zonulin and its regulation of intestinal barrier function: the biological door to inflammation, autoimmunity, and cancer. Physiol Rev. 91(1), 151-75.
- 34.Catassi C, Elli L, Bonaz B, Bouma G, Carroccio A et al.Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts'. , Criteria. Nutrients 7(6), 4966-77.
- 35.Zanini B, Basche R, Ferraresi A, Ricci C, Lanzarotto F et al. (2015) Randomised clinical study: gluten challenge induces symptom recurrence in only a minority of patients who meet clinical criteria for non-coeliac gluten sensitivity. Aliment Pharmacol Ther. 42(8), 968-76.
- 36.Elli L, Tomba C, Branchi F, Roncoroni L, Lombardo V et al. (2016) Evidence for the Presence of Non-Celiac Gluten Sensitivity in Patients with Functional Gastrointestinal Symptoms: Results from a Multicenter Randomized Double-Blind Placebo-Controlled Gluten Challenge. , Nutrients 8(2), 84.
- 37.Molina-Infante J, Carroccio A. (2016) Suspected Nonceliac Gluten Sensitivity Confirmed in Few Patients After Gluten Challenge in Double-Blind, Placebo-Controlled Trials. Clin Gastroenterol Hepatol.
- 38.Barrett J S. (2013) Extending our knowledge of fermentable, short-chain carbohydrates for managing gastrointestinal symptoms. Nutr Clin Pract. 28(3), 300-6.
- 39.Biesiekierski J R, Peters S L, Newnham E D, Rosella O, Muir J G et al. (2013) No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. 145(2), 320-8.
- 40.Marum A P, Moreira C, Tomas-Carus P, Saraiva F, Guerreiro C S. (2017) A low fermentable oligo-di-mono-saccharides and polyols (FODMAP) diet is a balanced therapy for fibromyalgia with nutritional and symptomatic benefits. Nutr Hosp. 34(3), 667-74.