
A Specific Case of Non-Specificity: Longitudinal Effects of Dysfunctional Attitudes on Depressive, Eating Disorder and Aggressive Symptoms in Children and Adolescents
Abstract
An important step in the validation of disorder-specific etiological models is the examination of the predictive specificity of proposed vulnerability factors. It may advance the understanding of the emergence of comorbidity and the identification of at risk-populations for mental disorders. To enhance the currently limited evidence on the specificity of Beck´s cognitive diathesis-stress model of depression, the present study investigated longitudinal effects of dysfunctional attitudes and stressful life events on the development of depressive, eating disorder and aggressive symptoms in children and adolescents. A large sample of initially asymptomatic children and adolescents completed self-report symptom measures at study entrance and again approx. 20 months later, and reported stressful life events during the study interval. Stressful life events proved to be a risk factor to all investigated symptom domains. Dysfunctional attitudes at T1 were prospectively related to depressive symptoms, aggressive behavior and weight concerns at T2. However, types of associations varied as dysfunctional attitudes showed linear associations with weight concern, but nonlinear effects on depressive and aggressive symptomatology. Findings of the current study thus suggest that dysfunctional attitudes are not uniquely related to the development of depressive symptomatology in children and adolescents, but may contribute to adverse outcomes in various symptom domains. Thus, intervention efforts based on Beck´s vulnerability - stress model of depression may turn out to be useful in reducing vulnerability to a variety of outcomes in children and adolescents.
Article Information
- Received
- Accepted
- Published
Academic Editor: Addo Boafo, Royal Institute of mental health research
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Susanne Meiser, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Susanne Meiser, University of Potsdam, Department of Psychology, Clinical Psychology | GRK 1668, Karl-Liebknecht-Straße, 24-25, 14476 Potsdam, Germany —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Beck´s prominent cognitive vulnerability - stress model posits that dysfunctional attitudes such as “My value as a person depends greatly on what others think of me” or “If I fail at work, then I am a failure as a person” increase risk for depression following the experience of stressful life events 1, 2. Empirical support for Beck´s model has been obtained in child and adolescent samples 3, 4. However, little is known regarding the specificity of the observed effects of dysfunctional attitudes to depression. Establishing the predictive specificity of a putative vulnerability factor is yet crucial for the validation of etiological models, particularly when investigating disorders with very high rates of comorbidity, such as depression 5, 6. While some studies have examined effects of dysfunctional attitudes with regard to anxiety disorders 6, 7, other symptom domains which are also highly comorbid with depression have received little attention. The current study seeks to address this shortcoming by examining associations between dysfunctional attitudes, depressive symptoms, eating disorders and externalizing problems.
Shared risk factors for depression and eating disorders have been reported 8. Preliminary evidence from cross-sectional studies using adult samples suggest that eating disorders may also be associated with elevated levels of dysfunctional attitudes 9, 10, but it remains unclear whether the obtained effects may be attributable to comorbid depressive symptoms 11. Moreover, evidence from younger samples and from longitudinal studies is still missing.
When examining the specificity of a vulnerability factor, it is also important to look at forms of psychopathology which are supposedly unrelated to the vulnerability in question 12. Aggressive behavior, for example, represents such a symptom domain. However, the only findings regarding this domain available to date are those by Hankin and colleagues 7, who did not find associations between dysfunctional attitudes and externalizing symptoms.
The Current Study
At present, evidence for Beck´s vulnerability – stress model is somewhat inconclusive in children and adolescents, which might in part be due to certain methodological aspects. First, some studies implied nonlinear effects of dysfunctional attitudes on depression indicating weak associations in the lower range, but considerably stronger effects at higher levels of dysfunctional attitudes 3, 13. Second, as Dykman and Johll 14 pointed out, effects of dysfunctional attitudes should be investigated in initially asymptomatic samples as Beck´s model was conceptualized to explain how initially asymptomatic but vulnerable individuals become depressed after experiencing stress.
The current study aims to enhance evidence on the specificity of Beck´s vulnerability – stress model to depression by investigating longitudinal effects of dysfunctional attitudes on depressive, eating disorder and aggressive symptomatology during late childhood and adolescence, a particularly crucial period for the initial development of mental disorders. To address potential sources of inconsistent findings in past research, linear and nonlinear methods will be employed using an initially asymptomatic sample, and co-occurring symptoms will be included as covariates in all statistical analyses. In line with existing research, we hypothesize dysfunctional attitudes to show vulnerability effects on future depressive and eating disorder symptoms, but not on aggressive behavior.
Materials and Methods
Participants
Participants were recruited from local schools in Potsdam and the surrounding federal state Brandenburg, Germany, and took part in a larger longitudinal project examining intrapersonal developmental risk factors in children and adolescents (PIER study). Data used for the current study was first collected in 2011/2012 and again in 2013/2014 with a mean interval between assessments of M = 20.1 months (SD = 2.94 months). Participants came from 122 different schools and from urban (46.6%), suburban (36.9%) and rural (16.4%) areas.
The initial sample consisted of 1064 children and adolescents aged between 9 and 18 years who participated at T1 and T2 and completed the stressful life events interview at T2. Of these, only participants presenting asymptomatic at T1 on either the depressive, the aggressive or the eating disorder symptom scales were selected resulting in a final sample of N = 1036 participants with a T1 mean age of 13.06 years (SD = 1.91; 49.7% female). Of the total sample, three subsamples were formed comprising individuals presenting initially asymptomatic on the depressive (n = 889), the eating disorder (n = 922) and the aggressive (n = 903) symptom scale.
Procedure
Participants completed measures of dysfunctional attitudes and depressive, eating disorder, and aggressive symptoms at T1. At T2, a stressful life events interview and again the dysfunctional attitudes and symptom measures were administered. Children and adolescents completed the assessments in standardized individual sessions in their schools after parents or participants of age had provided written informed consent. Alternatively, assessments took place at the children´s homes or on the university campus if schools were unable to provide rooms for data collection. Participants completed all questionnaires privately on a netbook or via paper and pencil, except for the stressful life events interview, which was conducted face-to-face. Questionnaires and the life events interview were administered by trained research assistants and doctoral psychology students. The procedure and instruments applied in the study were approved by the Ethics Committee of the University of Potsdam and the Ministry of Education of the German Federal state of Brandenburg.
Measures
Dysfunctional Attitudes.
To ensure age-appropriate measurement, items from two versions of the Dysfunctional Attitudes Scale (DAS) were used 15: children younger than 14 years completed a translation of the 22-item Dysfunctional Attitudes Scale for Children (DAS-C) by D´Alessandro and Burton 16, whereas participants aged 14 years and older completed the 20-item German DAS-J (“Dysfunctional Attitudes Scale for Adolescents”) 17. Both scales assess dysfunctional attitudes based on the DAS by Weissmann and Beck 15 and use a 5-point Likert scale (0 = disagree to 4 = agree).
A procedure of extracting content equivalent item pairs from the two scales and subsequently collapsing scales across age groups was applied to ensure that dysfunctional attitudes were measured in an age-appropriate manner without requiring a division of the sample: First, pairs of content equivalent items from the DAS-C and DAS-J were identified so that for each item drawn from the DAS-C, one item expressing comparable content was drawn from the DAS-J (e.g. item 13 from the DAS-C “If I disagree with other people, then they will hate me” was paired with item 5 from the DAS-J “If someone disagrees with me, it probably means that he/she doesn´t like me”). Items for which no comparable counterpart existed were excluded from subsequent analyses.
This procedure resulted in two comparable sets of 17 items. Principal components analyses of the 17 items drawn from the DAS-C and the 17 items drawn from the DAS-J showed almost identical, essentially unidimensional structures with slopes in the scree plots approaching a horizontal line after the first eigenvalue (5.017, then 1.466, 1.031, 1.055, 1.004 for the DAS-C items and 4.413, then 1.562, 1.229, 1.088 for the DAS-J items). Internal consistency of the obtained scales was α = .83 for the DAS-C items and α = .79 for the DAS-J items.
Depressive Symptoms
The Depression Test for Children, a German self-report depression inventory (18) designed for screening purposes was used to assess depressive symptoms in children and adolescents (“Depressionstest für Kinder [DTK]”). We used the two subscales “dysphoria/self-esteem” (25 items) and “tiredness/psychosomatic complaints” (14 items). The items are answered in a yes/no format and added up to a sum score representing the total number of reported depressive symptoms. The DTK has demonstrated good validity and reliability 18, 19 and has successfully been employed in depression research in child and adolescent samples 20, 21. It reached a Cronbach´s α = .84 at T1 and α = .85 at T2 in the current study.
Disordered Eating Behavior
The German version of the child Eating Disorder Examination Questionnaire (chEDE-Q) was employed to assess eating disorder symptoms 22. The chEDE-Q is a widely-used measure of eating disorder symptoms in children and adolescents and has shown good reliability and validity. Participants are asked to rate their behavior during the past four weeks on 22 items capturing symptoms on the four subscales restrained eating, eating concern, shape concern, and weight concern. Items are to be answered on a 7-point Likert scale. Internal consistency proved to be very good with Cronbach´s α = .93 at T1 and α = .94 at T2.
Aggressive Behavior
Aggressive Behavior was measured by 11 items assessing physical aggression (e.g. pushing or hitting someone), relational aggression (e.g. spreading gossip or saying nasty things about someone) and verbal aggression (insulting someone). Items were drawn from Möller and Krahé 23, Björkqvist and colleagues 24, and Archer and Coyne 25. Participants were asked to indicate how often they had shown certain behaviors during the current school year on a five-point Likert scale ranging from 0 = never to 4 = very often. This selection of items has successfully been applied in child and adolescent aggression research (20, 26) and showed satisfactory internal consistency in the present study with α = .79 at T1 and α = .76 at T2.
Stressful life events
Stressful life events were assessed via a semi-structured interview which was modelled after the Munich Event List 27 a widely used instrument assessing stressful life events via a combination of self-report checklists and face-to-face interview 28, 29. For economic reasons, only the face-to-face interview was conducted. Participants were asked if stressful events in the following categories had occurred during the past year: parents/family, school/education, leisure/friends, romantic relationships, health, and others. If an event had occurred, participants were asked to describe the event. To ensure comparability with previous studies (e.g). 3, 4, 30, the total number of stressful life events of the past year was used as stress measure for subsequent analyses, and not ratings of subjective or objective impact.
Data Analysis
Hierarchical linear and nonlinear regression analysis was used to test prospective and unique relations of dysfunctional attitudes, stressful life events and different symptom domains. Separate regression models were run for the prediction of depressive, eating disorder, and aggressive symptoms, respectively. To ensure that potential effects of dysfunctional attitudes would not be an artifact of comorbidity between the investigated symptom domains, comorbid symptoms were controlled for in all analyses.
Linear effects were tested in Steps 1 to 3 of the regression models, with T1 symptoms, T1 comorbid symptoms, age and gender entered in Step 1, dysfunctional attitudes and stressful life events entered in Step 2, and the interaction of dysfunctional attitudes and stressful life events (the diathesis - stress interaction) in Step 3. Nonlinear effects were tested by using squared and cubic values of participants’ dysfunctional attitudes scores. In Steps 4 and 5, quadratic and cubic effects of dysfunctional attitudes were entered, and interactions between squared and cubic values of dysfunctional attitudes were included in Steps 6 and 7.
To obtain initially asymptomatic samples, participants scoring above the cutoff of 14 (85th percentile in the current sample) were excluded when predicting T2 depressive symptoms 31. Because no validated cutoffs have been reported for our eating disorder and aggressive symptom measures, the 85th percentile of the respective distribution was set as cutoff so that participants exceeding this criterion were excluded from analyses predicting aggressive behavior or eating disorder symptoms, respectively.
Results
Preliminary Analyses
Descriptive statistics and bivariate correlations of the main variables for the total sample are presented in Table 1. Correlational analyses revealed intercorrelations between all symptom domains, moderate associations between dysfunctional attitudes and all symptom measures and low to moderate associations between life events and symptoms. Nearly all variables were related to participants´ age.
Table 1. Descriptive Statistics and Correlations| M (SD) | Range | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| 1. Age | 13.06 (1.91) | 9 – 18 | 0.32 | .190** | .116** | .087** | .148** | -.007 | .269** | .194** | |
| 2. DepressiveSymptoms T1 | 7.52 (6.07) | 0 – 38 | .432** | .230** | .570** | .296** | .160** | .349** | .178** | ||
| 3. Eating Disorder Symptoms T1 | 0.53 (0.72) | 0 – 5.18 | .086** | .317** | .582** | .081** | .288** | .152** | |||
| 4. AggressiveBehavior T1 | 1.40 (0.34) | 1 – 3.27 | .100** | .012 | .521** | .294** | .100** | ||||
| 5. DepressiveSymptoms T2 | 6.93 (5.98) | 0 – 34 | .469** | .247** | .231** | .249** | |||||
| 6. Eating Disorder Symptoms T2 | 0.64 (0.88) | 0 – 5.45 | .129** | .177** | .183** | ||||||
| 7. Aggressive Behavior T2 | 1.38 (0.31) | 1 – 2.91 | .205** | .105** | |||||||
| 8. Dysfunctional Attitudes T1 | 0.96 ( 0.52) | 0 – 3.18 | .094** | ||||||||
| 9. Life Events | 2.89 (2.17) | 0 – 14 |
Given these intercorrelations with age and the large age range of the current sample, the possibility of age moderating the effects of dysfunctional attitudes and life events was tested in a set of preliminary regression analyses. Age significantly moderated the effect of life events on depressive symptoms indicating a greater impact of life events among younger participants. No other moderating effects of age were detected.
Prediction of Depressive Symptoms
Results of the linear regression analysis of depressive symptoms are presented in Table 2 As the preliminary analyses had shown a significant interaction between age and life events, this interaction was included into all subsequent analyses regarding depressive symptoms in Step 2 to ensure that any interaction effect of dysfunctional attitudes and life events would relate to depressive symptoms beyond this effect. T2 depressive symptoms were, in Step 1, significantly predicted by gender and T1 depressive symptoms with a marginally significant effect of age. Step 2 revealed a significant main effect of life events and a marginally significant main effect of dysfunctional attitudes. The interaction between life events and dysfunctional attitudes was marginally significant in Step 3. Moreover, nonlinear regression revealed a significant cubic effect of dysfunctional attitudes, which is depicted in Figure 1.
Figure 1. Cubic effect of dysfunctional attitudes on change in depressive symptoms. Note that entering T1 depressive symptoms prior to other predictors into the regression model leaves residual change in symptoms to be explained by subsequent predictors (e.g. dysfunctional attitudes).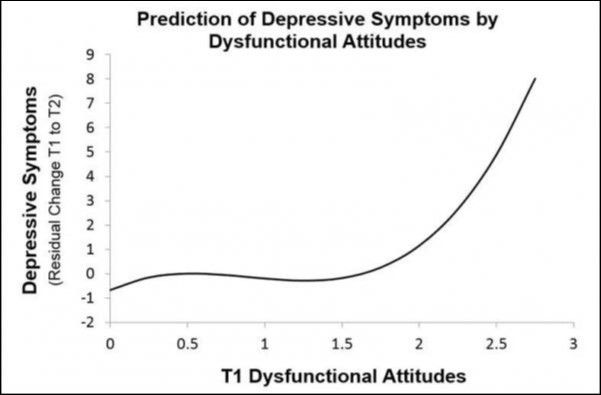
Download figure
| Predictor | β | t | p | Δ F | |
| Step 1 | Age | .048 | 1.565 | .118 | |
| Sex | .194 | 6.151 | .000 | ||
| T1 Depressive Symptoms | .369 | 11.089 | .000 | ||
| T1 Aggressive Behavior | .023 | .727 | .468 | ||
| T1 Eating Disorder Symptoms | .036 | 1.093 | .275 | ||
| 40.917*** | |||||
| Step 2 | T1 Dysfunctional Attitudes | .059 | 1.799 | .072 | |
| Life Events | .172 | 5.567 | .000 | ||
| Life Events * Age | -.081 | -2.644 | .008 | ||
| 16.600*** | |||||
| Step 3 | Dysfunctional Attitudes * Life Events | .058 | 1.916 | .056 | |
| 3.670† | |||||
| Step 4 | DAS2 | .155 | 1.531 | .126 | |
| 2.344 | |||||
| Step 5 | DAS3 | .623 | 2.081 | .038 | |
| 4.330* | |||||
| Step 6 | DAS2*Life Events | .145 | 1.454 | .146 | |
| 2.115 | |||||
| Step 7 | DAS3*Life Events | .519 | 1.668 | .096 | |
| 2.782† | |||||
Prediction of Eating Disorder Symptoms
Results of the regression model predicting eating disorder symptoms at T2 are presented in Table 3Eating disorder symptoms at T2 were, in Step 1, significantly predicted by T1 eating disorder symptoms and gender. Steps 2 showed that life events, too, predicted eating disorder symptoms while dysfunctional attitudes were unrelated to the outcome. The interaction of life events and dysfunctional attitudes reached marginal significance in Step 3. No nonlinear effects of dysfunctional attitudes were detected (all ps > .17).
Table 3. Hierarchical linear and nonlinear regression analysis predicting T2 eating disorder symptoms.| Predictor | β | t | p | Δ F | |
| Step 1 | Age | -.010 | -.325 | .745 | |
| Sex | .193 | 6.203 | .000 | ||
| T1 Eating Disorder Symptoms | .388 | 11.919 | .000 | ||
| T1 Depressive Symptoms | .023 | .700 | .484 | ||
| T1 Aggressive Behavior | -.057 | -1.760 | .079 | ||
| 45.744*** | |||||
| Step 2 | T1 Dysfunctional Attitudes | -.014 | -.417 | .677 | |
| Life Events | .105 | 3.380 | .001 | ||
| 5.867** | |||||
| Step 3 | Dysfunctional Attitudes * Life Events | .053 | 1.787 | .074 | |
| 3.192† | |||||
| Step 4 | DAS2 | -.008 | -.080 | .936 | |
| .006 | |||||
| Step 5 | DAS3 | .043 | .173 | .862 | |
| .030 | |||||
| Step 6 | DAS2* Life Events | -.009 | -.081 | .935 | |
| .007 | |||||
| Step 7 | DAS3* Life Events | -.387 | -1.364 | .173 | |
| 1.861 |
In order to determine whether the marginally significant interaction of dysfunctional attitudes and life events detected in Step 3 was accounted for by a specific symptom type, the linear regression models were re-run separately for the four chEDE-Q subscales restrained eating, eating concerns, shape concerns and weight concerns. These analyses revealed that the interaction of dysfunctional attitudes and stressful life events significantly predicted weight concerns (β = .068, t = 2.220, p = .027, see Figure 2) and marginally significantly predicted eating concerns
Figure 2. Interaction effect of dysfunctional attitudes and life events (stress) predicting change in weight concern. Note that entering T1 weight concern symptoms prior to other predictors into the regression model leaves residual change in symptoms to be explained by subsequent predictors (e.g. dysfunctional attitudes and stressful life events). 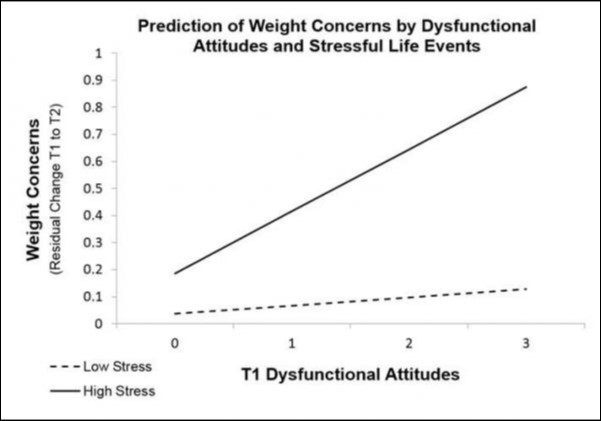
Download figure
(β = .060, t = 1.885, p = .060), while for restrained eating and shape concerns, no direct or indirect effects of dysfunctional attitudes were detected (all ps > .190).
Prediction of Aggressive Behavior
As depicted in Table 4, in the linear regression model, aggressive behavior at T2 was significantly predicted by effects of gender, T1 aggressive behavior, T1 depressive symptoms and age. Moreover, life events showed a significant effect in Step 2, but neither dysfunctional attitudes nor the interaction of dysfunctional attitudes and life events predicted T2 aggressive behavior significantly. However, the nonlinear tests revealed significant nonlinear effects of dysfunctional attitudes as squared values and the interaction of cubic values of dysfunctional attitudes and life events reached significance. As can be seen in Figure 3, the obtained nonlinear effects indicate a positive relationship between dysfunctional attitudes and aggressive behavior at low levels of dysfunctional attitudes while the opposite effect occurs at higher levels of dysfunctional attitudes. Slopes are more extremely pronounced in participants who experienced many life events.
Figure 3. Nonlinear interaction effect of dysfunctional attitudes and life events (stress) predicting change in aggressive behavior. Note that entering T1 aggressive behavior prior to other predictors into the regression model leaves residual change in symptoms to be explained by subsequent predictors (e.g. dysfunctional attitudes and stressful life events).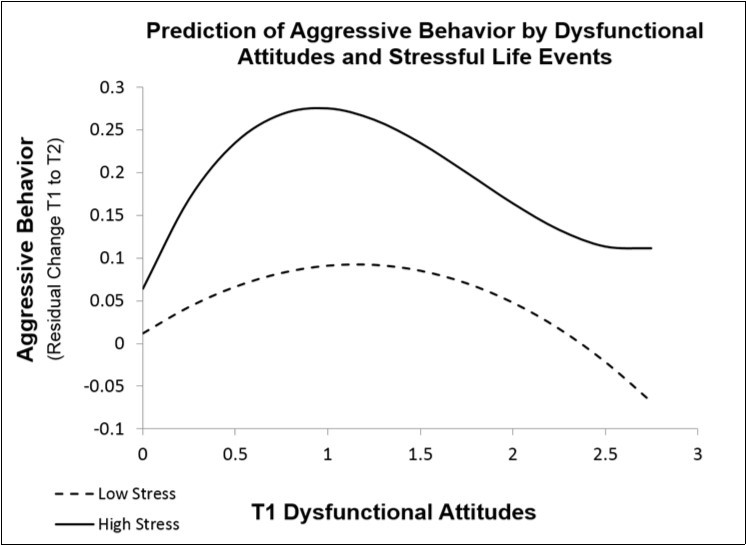
Download figure
| Predictor | β | t | p | Δ F | |
| Step 1 | Age | -.073 | -2.423 | .016 | |
| Sex | -.111 | -3.657 | .000 | ||
| T1 Aggressive Behavior | .422 | 13.688 | .000 | ||
| T1 Depressive Symptoms | .076 | 2.248 | .025 | ||
| T1 Eating Disorder Symptoms | .024 | .722 | .471 | ||
| 51.033*** | |||||
| Step 2 | T1 Dysfunctional Attitudes | .038 | 1.129 | .259 | |
| Life Events | .109 | 3.602 | .000 | ||
| 7.015** | |||||
| Step 3 | Dysfunctional Attitudes * Life Events | -.010 | -.331 | .740 | |
| .110 | |||||
| Step 4 | DAS2 | -.206 | -2.077 | .038 | |
| 4.314* | |||||
| Step 5 | DAS3 | .000 | -.001 | .999 | |
| .000 | |||||
| Step 6 | DAS2* Life Events | -.095 | -.880 | .379 | |
| .775 | |||||
| Step 7 | DAS3* Life Events | .591 | 1.985 | .047 | |
| 3.941* | |||||
Discussion
The aim of the current study was to extend knowledge on the specificity of Beck´s vulnerability-stress model of depression by exploring effects of dysfunctional attitudes on the development of depressive, aggressive and eating disorder symptoms in initially asymptomatic children and adolescents. Results show diverse, linear and nonlinear associations between dysfunctional attitudes and all the investigated symptom domains and thus indicate that dysfunctional attitudes in children and adolescents are not uniquely related to depressive symptomatology.
In the model predicting depressive symptoms, dysfunctional attitudes and their interaction with stressful life events were only marginally related to future depressive symptoms when only looking at linear effects. However, tests of nonlinear effects revealed a significant cubic effect of dysfunctional attitudes suggesting a strong impact at higher levels but almost no effect in the lower range of dysfunctional attitudes. This finding is consistent with a threshold view of dysfunctional attitudes, which was also suggested by the results of Lewinsohn and colleagues 3
Eating disorder symptoms in general were marginally predicted by the interaction of dysfunctional attitudes and life events. Analyses of the chEDE-Q subscales revealed that this effect was mainly accounted for by weight concerns, which were significantly predicted by the diathesis-stress interaction, and by eating concerns, which were marginally significantly related to the diathesis-stress interaction. Inspection of the interaction effect on weight concerns showed that dysfunctional attitudes had little effect under low stress conditions but a strong effect when participants experienced many life events.
These results suggest that dysfunctional attitudes in children and adolescents may also lead to increased preoccupation with weight and eating behavior. This seems plausible as perfectionistic standards for self-evaluation conferred by dysfunctional attitudes may also be applied to one´s body and food intake. Moreover, results are in line with previous findings suggesting an association between depression-related cognitions and eating disorder symptomatology 8, 9, 10, 11. Among other factors, these manifold effects of dysfunctional attitudes may thus represent a possible explanation for the co-occurrence of depression and eating disorders.
With regard to aggressive behavior, the linear analyses did not show any prospective effects of dysfunctional attitudes. So far, our results add to the existing findings suggesting no relationship between externalizing problems and depression-related cognitions 33, 34. However, a significant nonlinear effect of dysfunctional attitudes, moderated by life events, was revealed, which essentially exhibited an inverted U-shape. Both under low and high stress conditions, children and adolescents with moderate dysfunctional attitudes showed the greatest increase in aggressive behavior while participants with very low and very high dysfunctional attitudes exhibited the smallest increase or even a decrease in aggressive behavior.
To interpret this finding, correlations of single dysfunctional attitudes items with aggressive behavior were calculated 35. Inspection of the correlational pattern revealed some items to be positively associated with change in aggressive behavior while others showed a negative relationship. The dysfunctional attitude exhibiting the strongest positive correlation with aggressive behavior was “In order to be happy, it is important often to be the center of attention”, an attitude suggesting a certain amount of striving for attention and admiration by others. The strongest negative correlation, in turn, was found for the item “I have to be really good at one thing at least in order to be worth something”, which, in contrast, seems to represent a tendency towards critical self-evaluation. It could be hypothesized that participants with an overall moderate score on the dysfunctional attitudes scale are (partly) characterized by the ambition to distinguish themselves and to stand out from peers, which might increase readiness for aggressive acts. In individuals exhibiting overall high dysfunctional attitudes, in contrast, this need for attention seems to be accompanied by a high degree of self-criticism, which may cause them to refrain from behaving aggressively. As indicated by the moderating effect of life events, the difference between individuals showing overall moderate dysfunctional attitudes and those showing low or high dysfunctional attitudes is exacerbated by the experience of stressful life events.
Taken together, our results point to a certain degree of non-specificity of Beck´s vulnerability-stress model. However, types of associations between dysfunctional attitudes and outcomes varied considerably suggesting some degree of specificity in the exact shape of relationships. For example, both depressive symptoms and aggressive behavior were related to depressive symptoms, but while participants with moderate levels of dysfunctional attitudes showed heightened aggressive behavior, participants with high levels of dysfunctional attitudes exhibited heightened depressive symptoms but decreased aggressive behavior. In fact, relations of dysfunctional attitudes with aggression versus depression seem to be inverse to each other once a critical level is exceeded.
Life events were similarly predictive of increases in all investigated symptom domains. This confirms extant evidence suggesting that stressful life events should be understood as an unspecific risk factor for the development of psychopathology (e.g). 6, 24, 36. Interestingly, a life events*age interaction indicated that younger participants experienced higher depressive symptoms following life events than older participants. This is in line with theories suggesting that in younger children, environmental circumstances such as life events may be particularly strongly linked to depression 37, 38.
Our findings highlight the significance of transdiagnostic models of psychopathology as a way of conceptualizing the high co-occurrence of mental disorders. Recently, structural investigations of psychopathology yielded support for a bifactor model with the two higher-order factors Internalizing and Externalizing 39, which share a common liability, represented by a General Psychopathology dimension (the “p-factor”) 40. As dysfunctional attitudes and life events showed relations to all investigated symptom domains, the current findings might reflect a general association between these variables and the p-factor. Clearly, future research would benefit from linking investigations of specificity of vulnerability factors to structural models of psychopathology. For example, the inverted-U-shape association between dysfunctional attitudes and aggressive behavior found in the current study might be reflective of a positive association between dysfunctional attitudes and the p-factor, but of a negative one with the externalizing factor once p is controlled for.
Strengths and Limitations
Strengths of the current study include the use of a large sample, the examination of a variety of symptom domains, and the longitudinal design which, for example, allowed the exploration of longitudinal effects of dysfunctional attitudes on the development of eating disorder symptoms in youth for the first time. This is also the first study to include nonlinear effects in analyses of specificity of dysfunctional attitudes. By using an initially asymptomatic sample, effects of dysfunctional attitudes during the initial development of symptomatology could be assessed so that dysfunctional attitudes truly represented a predisposing factor (and not a symptom or consequence of psychopathology).
At the same time, some limitations should be considered. First, sample selection procedures such as eliminating initially symptomatic participants are controversial, mainly because this might also deplete the sub-sample of participants with high scores on the vulnerability measure and result in an attenuation of statistical associations due to a restriction in range 14, 41. However, the possibility that differential effects are active in high ranges of vulnerability was directly addressed by our nonlinear analyses.
Second, depressive, aggressive and eating psychopathology were assessed on the level of symptoms instead of clinical diagnoses. The clinical relevance of the obtained results therefore remains unclear. A replication of the present findings by future studies assessing clinical depression, conduct disorder and eating disorders is desirable.
Third, the total number of experienced life events was used as the stress variable in this study without taking into account the severity of each life event. While this is in line with a number of previous studies (e.g.) 3, 4, 12, 30), future studies using more extensive measurement techniques allowing a weighing of events according to their severity would be desirable.
Conclusion
Findings of the present study demonstrate that dysfunctional attitudes in initially asymptomatic children and adolescents prospectively relate to a variety of symptom domains, such as depressive symptoms, weight concerns, or aggressive behavior. However, dysfunctional attitudes showed associations of varying shapes (linear, cubic, inverted U-shape) with different symptom measures indicating that individuals exhibiting different levels of dysfunctional attitudes may be particularly at risk for different symptom domains: For example, children and adolescents showing very high levels of dysfunctional attitudes seem to be primarily at risk of developing depressive symptoms, while children and adolescents with moderate levels of dysfunctional attitudes are more likely to develop externalizing problems following the experience of stress. Considering this diversity in effects of dysfunctional attitudes, including nonlinear effects in future investigations of dysfunctional attitudes as a vulnerability factor seems advisable. Moreover, a replication of results by future studies assessing clinical diagnoses and using elaborate stressful life events measures is desirable.
At present, our findings suggest that dysfunctional attitudes in children and adolescents are not uniquely related to the development of depressive symptomatology and thus emphasize the necessity of scrutinizing the specificity of putatively disorder-specific etiological models. If replicated, the current results can be regarded as an important hint that prevention programs aiming at a modification of dysfunctional attitudes might be useful in reducing vulnerability to a variety of outcomes in children and adolescents.
References
- 1.A T Beck. (1967) Depression: Clinical, experimental, and theoretical aspects. , New York: Harper & Row
- 3.P M Lewinsohn, T E Joiner, Rohde P. (2001) Evaluation of cognitive diathesis-stress models in predicting major depressive disorder in adolescents. , J. Abn. Psy 110(2), 203-215.
- 4.Abela J R Z, Sullivan C. (2003) A Test of Beck’s Cognitive Diathesis-Stress Theory of Depression in Early Adolescents. , The J. Ear. Adolesc 23(4), 384-404.
- 5.J A Ralph, Mineka S. (1998) Attributional style and self-esteem; The prediction of emotional distress following a midterm exam. , J. Abn. Psy 107(2), 203-215.
- 6.B L Hankin, L Y Abramson, Miller N, G J Haeffel. (2004) Cognitive Vulnerability-Stress Theories of Depression: Examining Affective Specificity in the Prediction of Depression Versus Anxiety in Three Prospective Studies. , Cogn. Ther. Res 28(3), 309-345.
- 7.B L Hankin, Wetter E, Cheely C, C W Oppenheimer. (2008) Beck's cognitive theory of depression in adolescence: Specific prediction of depressive symptoms and reciprocal influences in a multi-wave prospective study. , Int. J. Cogn. Ther 1(4), 313-332.
- 8.J S Rawana, A S Morgan, Nguyen H, S G Craig. (2010) The relation between eating- and weight-related disturbances and depression in adolescence: A review. , Clin. Child Fam. Psy. Rev 13(3), 213-230.
- 9.Lazarus S, J P Galassi. (1994) Affect and cognitions in obese binge eaters and nonbinge eaters: The association between depression, anxiety, and bulimic cognitions. , Eat. Dis.: J. Treat. & Prev 2(2), 141-157.
- 10.Schlesier-Carter B, S A Hamilton, P M O’Neil, R B Lydiard, Malcolm R. (1989) Depression and bulimia: The link between depression and bulimic cognitions. , J. Abn. Psy 98(3), 322-325.
- 11.Steiger H, Goldstein C, Mongrain M, Feen J Van der. (1990) Description of eating-disordered, psychiatric, and normal women along cognitive and psychodynamic dimensions. , Int. J. Eat. Dis 9(2), 129-140.
- 12.Nolen-Hoeksema S, Stice E, Wade E, Bohon C. (2007) Reciprocal relations between rumination and bulimic, substance abuse, and depressive symptoms in female adolescents. , J. Abn. Psy 116(1), 198-207.
- 13.B E Gibb, L B Alloy, L Y Abramson, C G Beevers, I W Miller. (2004) Cognitive Vulnerability to Depression: A Taxometric Analysis. , J. Abn. Psy 113(1), 81-89.
- 14.B M Dykman, Johll M. (1998) Dysfunctional attitudes and vulnerability to depressive symptoms: A 14-week longitudinal study. , Cogn. Ther. Res 22(4), 337-352.
- 15.A N Weissmann, A T Beck. (1978) Development and validation of the Dysfunctional Attitudes Scale. Paper presented at the annual meeting of the Association for the Advancement of Behavior Therapy. , Chicago, IL
- 16.D'Alessandro D U, Burton K D. (2006) Development and validation of the Dysfunctional Attitudes Scale for Children: Tests of Beck's cognitive diathesis-stress theory of depression, of its causal mediation component, and of developmental effects. , Cogn. Ther. Res 30(3), 335-353.
- 17.Keller F, Kirchner I, Pössel P. (2010) Die Skala Dysfunktionaler Einstellungen für Jugendliche (DAS-J): Entwicklung und Evaluation. [Dysfunctional Attitude Scale for adolescents (DAS-J): Development and evaluation.] Zeitschrift für Klinische Psychologie und Psychotherapie: Forschung und Praxis. 39(4), 234-243.
- 19.Krackow E, Kania K, R M Travers. (2013) Does negative mood confer an advantage in the recall of negative life events?. , Imagination, Cognition and Personality 32(3), 291-305.
- 20.Bondü R, Esser G. (2015) Justice and rejection sensitivity in children and adolescents with ADHD symptoms. [Empfänglichkeit für Gerechtigkeit und Ablehnung bei Kindern und Jugendlichen mit ADHS-Symptomen]. Eur. Child & Adolesc. Psychiatr 24(2), 185-198.
- 21.Schwarz S, Beyer L. (2008) Validierung der deutschen Montgomery Asberg Depression Rating Scale (MADRS) für das Kindes- und Jugendalter. [Validation of the German Montgomery Asberg Depression Rating Scale (MADRS) for children and adolescents]. Empirische Evaluationsmethoden. Band 12: Workshop2007. 63-75.
- 22.Hilbert A, A S Hartmann, Czaja J. (2008) Child Eating Disorder Examination-Questionnaire: Evaluation der deutschsprachigen Version des Essstörungsfragebogens für Kinder. [The Eating Disorder Examination-Questionnaire for Children: Psychometric properties of the German version]. Klinische Diagnostik und Evaluation. 1(4), 447-463.
- 23.Möller I, Krahé B. (2009) Exposure to violent video games and aggression in German adolescents: A longitudinal analysis. , Aggr. Beh 35(1), 75-89.
- 24.Björkqvist K, Österman K, Kaukiainen A. (1992) The development of direct and indirect aggressive strategies in males and females. In. , San Diego, CA, US: 51-64.
- 25.Archer J, S M Coyne. (2005) An Integrated Review of Indirect. , Relational, and Social Aggression. Pers. & Soc. Psy. Rev 9(3), 212-230.
- 26.Krahe B, Möller I. (2010) Longitudinal effects of media violence on aggression and empathy among German adolescents. Längsschnittliche Effekte von Gewalt in den Medien auf Aggression und Empathie , Psy 31(5), 401-409.
- 27.Maier-Diewald W, H U Wittchen, Hecht H, Werner-Eilert K. (1983) Münchner Ereignisliste. München: Max-Plank Institut für Psychiatrie.
- 28.Asselmann E, H U Wittchen, Lieb R, Höfler M, Beesdo-Baum K. (2015) Danger and loss events and the incidence of anxiety and depressive disorders: A prospective-longitudinal community study of adolescents and young adults. , Psy. Med 45(1), 153-163.
- 29.Perkonigg A, K A Yonkers, Pfister H, Lieb R, Wittchen H-U. (2004) Risk Factors for Premenstrual Dysphoric Disorder in a Community Sample of Young Women: The Role of Traumatic Events and Posttraumatic Stress Disorder. , J. Clin. Psychiat 65(10), 1314-1322.
- 30.Abela J R Z, S A. (2007) Dysfunctional attitudes, self-esteem, and hassles: Cognitive vulnerability to depression in children of affectively ill parents. , Beh. Res. Ther 45(6), 1127-1140.
- 31.Frühe B, Allgaier A-K, Pietsch K, Schulte-Körne G. (2012) Depression screening in pediatric patients - A comparison of the concurrent validity of the German version of the Children's Depression Inventory (Depressionsinventar für Kinder und Jugendliche), the Depressionstest für Kinder (German Depression Test for Children), and the new Children's Depression Screener. Zeitschrift für Kinder- und Jugendpsychiatrie und Psychotherapie. 40(3), 161-169.
- 32.Goebel M, Spalthoff G, Schulze C, Florin I. (1989) Dysfunctional cognitions, attributional style, and depression in bulimia. , J. Psychosom. Res 33(6), 747-752.
- 33.L B Alloy, S K Black, M E Young, K E Goldstein, B G Shapero. (2012) Cognitive vulnerabilities and depression versus other psychopathology symptoms and diagnoses in early adolescence. , J. Clin. Child & Adolesc. Psy 41(5), 539-560.
- 34.B L Hankin. (2008) Cognitive vulnerability-stress model of depression during adolescence: Investigating depressive symptom specificity in a multi-wave prospective study. , J. Abn. Child Psy 36(7), 999-1014.
- 35.R J Haans, Pieters C, He Z. (2016) Thinking about u: Theorizing and testing U- and inverted U-shaped relationships in strategy research. , Strat. Manag. J 37(7), 1177-1195.
- 36.Rojo L, Conesa L, Bermudez O, Livianos L. (2006) Influence of Stress in the Onset of Eating Disorders: Data From a Two-Stage Epidemiologic Controlled Study. , Psychosom. Med 68(4), 628-635.
- 37.Nolen-Hoeksema S, J S Girgus, M E Seligman. (1992) Predictors and consequences of childhood depressive symptoms: A 5-year longitudinal study. , J Abn. Psych 101(3), 405-422.
- 38.Shirk S R. (1988) Causal reasoning and children´s comprehension of therapeutic interpretations.In. , SR Shirk (Ed.), Cogn Dev & Child
- 39.R F Krueger, N R Eaton. (2015) Transdiagnostic factors of mental disorders. , World Psychiatr 14(1), 27-29.
Cited by (2)
This article has been cited by 2 scholarly works according to:
Citing Articles:
Psychological applications and trends (2023) OpenAlex
Journal of Depression And Therapy (2017) OpenAlex