
P16/INK4a and KI-67 Evaluation of Intraepithelial and Benign Cervical Lesions at the University College Hospital, Ibadan - A Retrospective Immunohistochemically Study
Abstract
Objective
P16INK4a and Ki-67 are adjuncts to current histological assessment of cervical biopsies in identifying cases that require strict follow up and prompt intervention. This study aimed to evaluate P16INK4a and Ki-67 expression in squamous intraepithelial and other benign cervical lesions.
Methods
A retrospective cross-sectional study of 153 cases of cervical biopsies diagnosed as CIN and benign cervical lesions between 2006 and 2013 at the University College Hospital, Ibadan, Nigeria. Slides and tissue blocks of all the selected cases were retrieved and classified using the 2003 WHO classification for intraepithelial and benign cervical lesions and were stained with p16INK4a and Ki-67 immunohistochemical stains following heat-induced antigen retrieval. Results were evaluated and compared with histologic diagnosis.
Results
Cases were classified as chronic cervicitis (12.3%), squamous Metaplasia (0.7%), CIN 1 (47.1%), CIN 2 (36.6%) and CIN 3 (3.3%). Majority of the non-dysplastic cervical lesions (including chronic cervicitis cases) showed low P16INK4a reactivity. Positive P16INK4a reactivity was seen in 80% of CIN 3 cases, 83.9% of CIN 2 cases, and, surprisingly, in 97.2% of CIN 1 cases. Ki-67 positivity was seen in 36.6% of cases (75% CIN 2 and 60% CIN 3). There was a significant correlation between the H&E diagnoses of CIN and P16INK4a/Ki-67 immunoreactivities.
Conclusion
Majority of the CIN 1 cases showing low grade p16INK4a immunereactivity strongly suggesting that cervical squamous intraepithelial neoplasia in this environment is likely associated with high grade HPV subtype infections and may predict possible progression to high grade squamous intraepithelial neoplasia. The use of P16INK4a and Ki-67 in the evaluation of cervical biopsies for benign mimics of high grade intraepithelial lesion will aid proper single Pathologist evaluation and help in patients triaging for follow up.
Article Information
- Received
- Accepted
- Published
Academic Editor: Xi Zhang, Co-founder & Scientist SinoScript LLC
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Adetona A. E, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: Ogunbiyi John Olufemi, MBBS, FWACP (Lab. Med), IFCAP, FCPath (ECSA); UCH/UI IBADAN —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
The incidence of cervical cancer is increasing yearly and it is only second to breast cancer among women.1 The precursor lesions for invasive squamous cell carcinoma are squamous intraepithelial neoplasia, variably referred to as squamous intraepithelial lesion (SIL) and carcinoma in situ.
P16INK4a and Ki-67 have gained increasing popularity as adjuncts in the prognostication of cervical cancer because they may serve as markers indicating the presence of high risk HPV subtypes in this lesion. The E6 and E7 proteins of the high-risk HPV inhibit the p53 and pRb proteins respectively, which are cell cycle regulatory proteins controlling G1-S transition.4, 5 The phosphorylation of pRb induces the release of a transcription factor E2F from the bound form of E2F and pRb. The released E2F then stimulates the expression of genes which are involved in G1-S transition5. The inactivation of pRb by E7 causes the p16INK4a (P16 Inhibitor of Cyclin Dependent Kinase 4a) overexpression by negative feedback of pRb.3 p16INK4a overexpression appears to be independent of the particular type of high-risk HPV and is overexpressed in almost all high grade SIL (HSIL) and invasive cervical cancers.8, 20p16INK4a is particularly an important biomarker for HPV-associated SIL since its overexpression within cervical neoplasia has been directly linked to high expression of E7 HPV oncogene.2, 3
Ki-67 is a well-known cell proliferation marker andcan be used in the grading of Cervical intraepithelial lesion (CIN)/SIL,2, 3in which staining occurs in the upper two-thirds of the epithelium, whereas normal squamous epithelium typically shows only limited staining in the parabasal cell layer. Other benign lesions that are most commonly mistaken for HSIL include immature squamous metaplasia, reactive/reparative processes, and atrophy and these can be clearly separated from HGSIL by the use of p16INK4a and Ki-67 immunostains which are usually negative in them.
This study aimed to evaluate p16INK4a and Ki-67 expression in SIL and other benign cervical lesions in order to increase the diagnostic accuracy in equivocal cases.
Materials and Methods
Materials
A retrospective cross-sectional study was done involving the review of all the histologically diagnosed cases of SIL and other benign cervical lesions seen in the Pathology Department of a large tertiary hospital in South Western Nigeria between January 2006 and December 2013. Information was extracted from the departmental records and request forms.
The slides and tissue blocks of all the selected cases were retrieved. The primary antibody for p16INK4a was a monoclonal mouse anti-p16INK4a antibody (1E12E10, San Diego, CA 92124) in 1:200 dilutions while that of Ki-67 was monoclonal rabbit anti Ki-67 antibody (Thermo RM-9106-R7, UK) in 1:100 dilutions. The staining was validated with the respective negative and positive controls.
Methods
All the Haematoxylin and Eosin (H&E) slides were reviewed and classified using the 2003 World Health Organization classification for intraepithelial and benign lesions of the cervix.8 All the cases were reviewed and re-grouped based on consensus H&E diagnoses agreed upon by two Pathologists and the first author. The cases were also stained with p16INK4a and Ki-67 immunohistochemically stains following heat-induced antigen retrieval method. Briefly, the sections were deparaffinized in xylene and were sequentially rehydrated in graded alcohol for two minutes. To increase the antigen detection, the slides were immersed in a citrate acid solution and were heated for 20 minutes and then incubated with antibodies for 32 minutes; Diaminobenzidine (DAB) was introduced for 4 minutes and they were counterstained with Mayer's Haematoxylin for 4 minutes. Stained slides were dried and were covered with glass cover slides.
The p16INK4a immunostaining was nuclear and/or cytoplasmic staining in the epithelium and was graded based on the pattern of distribution and levels of epithelial involvement as negative (0), 1+, 2+, and 3+. Cases with no epithelial staining were grouped as negative for p16INK4a, 1+ was staining of basal/parabasal up to one-third of the epithelium in a focal or diffuse nuclear and/or cytoplasmic stain, 2+ involves up to two-third of the epithelium and 3+ which involves above two-third to full epithelial thickness. The pattern of Ki-67 immunostain was graded as positive and negative based on the pattern of distribution and the level of involvement of the cervical epithelium. Negative Ki-67 was determined by scattered epithelial staining limited to the basal cells or a complete absence of staining while positive Ki-67 immunostain was accepted when the pattern was that of scattered or diffuse epithelial staining above the basal and parabasal cells. The Immunohistochemistry slides were subsequently viewed and analysed. The relationship between the age, H&E diagnoses, P16INK4a and Ki-67 reactivity were determined by correlation and the statistical significance was obtained using the Statistical Package for Social Sciences version 18 (SPSS-18). The chi-square test was used for discrete variables, with the level of significance set at p ≤ 0.05 and kappa was used to test for the strength of the associations. All ethical issues were duly considerfed and ethical approval was obtained from appropriate Local Ethical Committee.
Exclusion criteria:
Cases whose blocks and/or slides could not be retrieved were excluded from this study.
Results
On the basis of their initial diagnoses, the 153 cases of SIL and benign cervical lesions, were classified as CIN 1 (49%), CIN 2 (25.5%) and CIN 3 (3.3%) while the clearly benign cases were basically chronic cervicitis (20.3%) and squamous metaplasia (2.0%).
All the cases were reviewed and re-grouped based on consensus H&E diagnoses as 47.1% CIN 1, 36.6% CIN 2 and 3.3% CIN 3 i.e. some cases of CIN 1 were upgraded to CIN 2 likely because severe chronic inflammation associated with some of the CIN 1 masked the severity of the squamous intraepithelial neoplasia in the initial evaluation. Also, we allotted chronic cervicitis to 12.3% and Squamous metaplasia were 0.7%. Also noted were various degrees of stromal lymphocytic infiltrations. The overall agreement between previous and consensus diagnosis was 60%, and their correlation was statistically significant (p<0.0001).
Age Distribution
The cases ranged in age from 23 years to 80 years (mean: 46.3 years). The largest proportion of cases (41.8%) was within the age group 40-49 years while the lowest proportion, (2.6%) were within the 20-29 years age group (Table 1). The age distribution correlation with the various categories of cases is also shown in Table 1.
Table 1. Age Distributions of Various Categories of cases| Age group (Years) | Chronic Cervicitis | Stpuunous Metaplash * | CIN I | CINII | CIN III | Total |
| 20-29 | 0 (0.0%) | 0 (0.0%) | 2(1.3%) | 1 (0.7%) | 1 (0.7%) | 4(2.6%) |
|---|---|---|---|---|---|---|
| 30-39 | 3(2.0%) | 0 (0.0%) | 21(13.7%) | 12 (7.8%) | 0 (0.0%) | 36(23.5%) |
| 40-49 | 13 (8.5%) | 0 (0.0%) | 29(19.0%) | 20(13.1%) | 2(1.3%) | 64(41.8%) |
| 50-59 | 0(0.0%) | 0 (0.0%) | 14 (9.2%) | 15 (9.8%) | 1(0.7%) | 30(19.6%) |
| 60 -above | 3(2.0%) | 1(0.7%) | 6(3.9%) | 8(5.3%) | 1(0.7%) | 19(12.4%) |
| Total | 19(12.4%) | 1(0.7%) | 72(47.1%) | 56(36.6%) | 5(3.3%) | 153(100.0) |
P16INK4a Immunostaining
The p16INK4a distribution pattern was such that 1+ was seen in 92 (60.1%) cases, 2+ seen in 51 (33.3%), 3+ in 8 (5.2%) while only 2 (1.3%) were negative.
Table 2 below also showed that there was a good correlation between the grade of the intraepithelial lesions and the degree of expressivity of p16INK4a. Positive p16INK4aexpression varied significantly with H&E diagnosis, among the CIN 1, low grade P16INK4a reactivity (1+) was seen in 95.8% of cases, (Table 2; Figure 1.1), while only 1.4% show grade 2+ and others were negative. The majority of CIN 2 lesions (83.9%) showed grade 2+ P16INK4a reactivity (Figure 1.2), however, 80% of CIN 3 lesions showed grade 3+ P16INK4a reactivity (Figure 1.3) with the remaining 20% showing grade 2+ staining (Table 2). Most of the non-dysplastic cervical lesions in this study also showed low grade of p16INK4a reactivity. The overall agreement between the H&E diagnoses and the p16INK4a immunostain reactivity was significant (p<0.0001).
Table 2. Correlation between H&E diagnoses, P16INK4a and KI-67| P16INk4a | ||||
| Cases | I+ | 3+ | 3. NEG | TOTAL |
| Chronic Cervicitis | 17 (89.5%) | 2 (10.5%) | 0 (0.0%) 0(0.0%) | 19 (100.0%) |
| Squamous metaplasia | 1(100.0%) | 0(0.0%) | 0(0.0%) 0(0.0%) | I (100.0%) |
| CIN I | 69 (95.8%) | 1 (1.4%) | 0(0.0%) 2 (2.8%) | 72 (100.0%) |
| CIN II | 5(9.0%) | 47(83.9%) | 4(7.1%) 0(0.0%) | 56(100.0%) |
| CIN III | 0(0.0%) | 1(20.0%) | 4(80.0%) 0 (0.0%) | 5 (100.0%) |
| Ki-67 | ||||
| Cases | positive | Negative | Total | |
| Chronic Cervicitis | 4(21.1 %) | 15(78.9%) | 19(100.0%) | |
| Squamous metaplasia | 1 (100.0%) | 0(0.0%) | 1 (100.0%) | |
| CIN I | 5 (6.9%) | 67 (93.1%) | 72 (100.0%) | |
| C1N II | 42 (75%) | 14 (25%) | 56 (100.0%) | |
| CIN 111 | 3 (60%) | 2 (40%) | 5 (100.0%) |
Figure 1. Photomicrographs showing (a. x 100) Hematoxylin and Eosin (H&E) and immunohistochemical staining of (b. x 400) p16INK4a and (c. x 400) Ki-67. 1.1. CIN I, a, H&E staining. b, diffuse (one-third) p16INK4a immunostaining. c, scattered Ki-67 immunostaining in CIN 1; 1.2. CIN 2. a, H&E staining. b, diffuse nuclear and cytoplasmic (two-third) p16INK4a immunostaining. c, scattered Ki-67 immunostaining in CIN 2; 1.3. CIN 3. a, H&E staining. b, diffuse nuclear and cytoplasmic (above two-third) p16INK4a immunostaining. c, scattered Ki-67 immunostaining in CIN 3.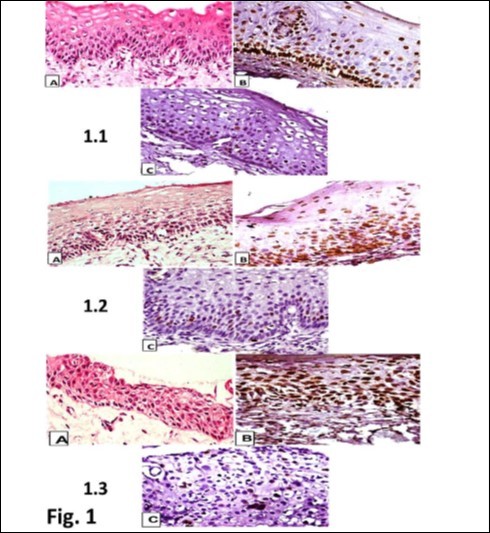
Download figure
Ki-67 Immunostain
Ki-67 immunoreactivity was seen in fewer cases (36.6%) with the greater proportion seen in CIN 2 (75%) and CIN 3 (60%), while the majority (64.1%) of the cases showed negative Ki-67expression. Ki-67 positivity was also seen in some cases of chronic cervicitis and in the only case of squamous metaplasia.
(p<0.0001) respectively.
P16INK4a and Ki-67 Immunostains
Majority of the grade 2+ (76.5%) and grade 3+ (87.5%) p16INK4a positive cases were positive for Ki-67. However, 8.7% of grade 1+ p16INK4a positive cases were also positive for Ki-67. The correlation between the p16INK4a and Ki-67 immunoreactivities seen in this study is significant (p<0.0001). (Table 3)
Table 3. Correlation between P16INK4a and Ki-67| Ki-67 | P16INK4a | ||||
| 1+ | 2+ | 3+ | NEG | TOTAL | |
| POS | 8(14.5%) | 39(71.0%) | 7(12.7%) | 1(1.8%) | 55(100.0%) |
|---|---|---|---|---|---|
| NEG | 84(85.7%) | 12(12.3%) | 1(1.0%) | 1(1.0%) | 98(100.0%) |
| Total | 92(60.1%) | 51(33.3%) | 8(5.2%) | 2(1.4%) | 153(100%) |
The overall agreement between the p16INK4a and the Ki-67 immunostain reactivity was 68.7% (kappa 52.4%, p<0.0001).
Discussion
Due to the subjectivity in the CIN evaluation with intra- and inter-observer variations of histomorphological characteristics, the consensus pathologist’s review resulted in variations between the initial H&E assessment and final diagnoses. There was concordance in up to about 60%, slightly less than the 67.5% correlation observed in an Iranian study.9
This variation between the initial and final diagnoses seen in the present study may be partly explained by the chronic cervicitis and tissue reaction observed with most dysplastic changes10. However, equivocal cervical lesions had their diagnosis aided by useful adjunctive immunohistochemical stains such as P16INK4a and Ki-67, this was also observed to be useful in previous studies.2, 9, 11
The majority of cases reviewed in this study were CIN 1 (47.1%) and a significant proportion of chronic cervicitis (12.4%) was also observed to be associated with CIN 1 as compared to the 36.6% of the CIN 2 and the 3.3% of CIN 3. The preponderance of CIN 1 observed in this study (47.1%) is slightly lower than those observed in some previous studies done by Sari et al9 in Iran, Hariri et al12 in Denmark, and Guo et al13 in the US who reported 51%, 65% and 72% respectively of CIN 1 proportion in their studies.
The highest proportion of all the reviewed cases in this study was in the age group 40-49 years (mean age: 46.3 years) which is slightly higher than what was obtained in the studies done in Greece by Haidopoulos et al14 with a mean age of 40.7 years and the United States by Guo et al15 with a mean age of 24.7 years. This observed pattern of age distribution may be due to the fact that more women around the age group 40-49 years have better attitudes toward cervical cancer screening. The 40-49 years correspond to the average perimenopausal age group of women in this environment16 and they are therefore more concerned about their health status despite poor awareness and lack of easy accessibility to the few locally available cervical cancer screening programmes.17 The age group 20-29 years was least represented despite the fact that they represent a very sexually active cohort of women. This may be largely due to many factors, including poor awareness on the importance of cervical cancer screening, and the lack of a national cervical screening programme and screening policy that ensure early commencement of screening (pap smear) by females in this age group which will eventually reduced the cancer incidence drastically.18, 19 p16INK4a is one of the most intensely studied biomarker in uterine cervix related diseases and findings from such studies have consistently affirmed a potential role of this ancillary diagnostic tool in the evaluation of histologic and cytologic cervical samples.15, 20, 21 It is a new diagnostic approach, which is based on the detection of measureable indicators of exposure to HPV, susceptibility to infection and actual establishment of the disease.
The patterns of p16INK4a expressivity in this study revealed that majority of the cases (60.1%) had low grade (+1) p16INK4a immunostain reactivity, both in extent and in intensity, 38.5% had high grade (+2 or +3) while less than 5% cases remaining were negative.
There are variations in the pattern of expression of p16INK4a among different grades of cervical intraepithelial neoplasia in several previous studies.7, 9, 12, 22 Generally, p16INK4a positivity was low (0-62%) in CIN 1 but higher (50-100%) in CIN 2 and CIN 3.6, 23 With respect to CIN 1, the p16INK4a expression varied in different centres and was considerably higher in some.
The correlation between the H&E and p16INK4a immunostain showed that high grade dysplastic changes are more associated with high grade p16INK4a immunostain and vice versa. This is also seen in most of the previous studies done7, 9, 12, 22 indicating a better agreement between the H&E diagnoses and the p16INK4a expression with a correlation of 77.5% (p<0.0001) in this study.
Majority of the CIN 1 cases show low grade p16INK4a immunoreactivity in this study and this is similar to what was observed in previous studies by Klaes et al,7 Hariri et al12 and Focchi et al,22 in which higher proportions of CIN 1 cases (87%, 90.9% and 91% respectively) showed low grade p16INK4a expressions. However, in Sari9 and Queiroz24 studies among the Iranian and Brazilian populations, lower proportions of CIN 1(31% and 40%) showed p16INK4a expression. Since positive staining with p16INK4a is associated with high-risk HPV subtype infections, finding significant staining even in CIN 1 and chronic cervicitis cases will suggest that, in this environment, there is an increased risk of HPV induced squamous intraepithelial lesion, (the exact proportion of which has not been determined). The presence of p16INK4a positive cells suggests the possibility of progression from a low grade to a higher grade dysplastic lesion among these cases. This can aid in triaging cases of CIN 1 that will need strict follow up plans. This was shown in two previous prospective studies by Haidopoulos et al.14 in Greece and Miyamoto et al.15 in the United States where initial and follow up biopsies were subsequently reviewed with a high incidence of progression to CIN 2 among patients with initial CIN 1 cases with p16INK4a positivity. Higher positive p16INK4a expression of 80% in CIN 3 was seen in this study as compared to many previous studies.7, 15, 25, 26
The use of a cocktail of both p16INK4a and Ki-67 antibodies along with the H&E staining has been shown in various studies to aid the proper evaluation of cervical squamous intraepithelial lesions and other benign lesions and for possible prognostication of the progression of a low grade to a high grade squamous intraepithelial neoplasia.27, 28
In this study, only a few cases with low p16INK4a positivity (5.2%) showed Ki-67 positivity but there was a significant correlation between p16INK4a and Ki-67 immunostaining with an overall agreement of 68.7%. A high correlation was seen between Ki-67 positivity and high grade p16INK4a immunostaining. This high correlation between p16INK4a and Ki-67 in high grade squamous intraepithelial neoplasia is similar to what was reported in several previous studies,3, 29, 30 one of which concluded that co-localization of p16INK4a and Ki-67 is a practically and potentially powerful diagnostic approach to facilitate accuracy of CIN histopathologic diagnosis.30
Thus, the findings in this study further affirm the importance of these stains in the evaluation of the squamous intraepithelial and other benign lesions.
Conclusions
This study revealed the pattern of distribution of the squamous intraepithelial lesions and benign lesions usually encountered in this environment with a higher incidence of CIN 1 cases as against CIN 2 or 3. The majority of these CIN 1 cases have associated cervicitis.
A high proportion of low grade squamous intraepithelial neoplasia (CIN 1) with varying degrees of p16INK4a and Ki-67 expression seen strongly suggests that cervical squamous intraepithelial neoplasia in this environment are likely associated with high grade HPV subtype infections and may predict possible progression to high grade squamous intraepithelial neoplasia.12, 13 This finding is also corroborated by the p16INK4a expression seen among few cases of chronic cervicitis without squamous intraepithelial neoplasia. Although, this submission will need to be confirmed by further evaluation of positive cases for HPV DNA identification and sequencing.
The use of P16INK4a and Ki-67 in the evaluation of cervical biopsies for benign mimics of high grade intraepithelial lesion will aid proper single Pathologist evaluation and help in patients triaging for follow up.
List of Abbreviations
P16INK4a - P16 Inhibitor of Cyclin Dependent Kinase 4a
Ki-67 – proliferative index
HPV – Human Papillomavirus
E6 and E7 - “Early” genes 6 and 7 oncoprotein (nonstructural)
CIN – Cervical Intraepithelial Neoplasm
H&E – Haematoxylin and Eosin
SIL - Squamous Intraepithelial Lesion
E2F – E2 transcription factor
DAB - Diaminobenzidine
SPSS-18 - Statistical Package for Social Sciences version 18
References
- 1.Torre L A, Bray F, Siegel R L, Ferlay J, Lortet-Tieulent J et al. (2015) . Global cancer statistics,CA Cancer JClin 65(2), 87-108.
- 2.Keating J T, Cviko A, Riethdorf S. (2001) Ki-67, cyclin E, and p16INK4 are complimentary surrogate biomarkers for human Papillomavirus-related cervical neoplasia.Am JSurgPathol. 25(7), 884-891.
- 3.Nam E J, Kim J W, Hong J W. (2008) Expression of the p16 and Ki-67 in relation to the grade of cervical intraepithelial neoplasia and high-risk human papillomavirus infection.JGynecolOncol. 19(3), 162-168.
- 4.Slebos R J, Lee M H, Plunkett B S. (1994) p53-dependent G1 arrest involves pRB-related proteins and is disrupted by the human papillomavirus 16 E7 oncoprotein.Proc. , NatlAcadSci 91, 5320-5324.
- 5.Tsoumpou I, Arbyn M, Kyrgiou M. (2009) p16(INK4a) immunostaining in cytological and histological specimens from the uterine cervix: a systematic review and meta-analysis.Cancer Treat Rev. 35(3), 210-220.
- 6.Wright T C, Ronnett B M, Kurman R J. (2011) . Precancerous Lesions of the Cervix. In: Kurman RJ, Ellenson LH RB, ed.Blaustein’sPathology of the Female GenitalTract.Sixth.London:Springer-Verlag; 193-252.
- 7.R1 Klaes, Friedrich T, Spitkovsky D. (2001) Overexpression of p16(INK4A) as a specific marker for dysplastic and neoplastic epithelial cells of the cervix uteri.IntJcancerJ. 92(2), 276-284.
- 8.Wells M, Ostor A G, Franceschi S. (2003) Epithelial tumors of the uterine cervix. In: Tavassoli FA, Devilee P, ed.IARC. Lyon 221-232.
- 9.Sari A, Fatemeh S, Akbar P. (2013) . Evaluation of Ki67, p16 and CK17 markers in differentiating cervical intraepithelial neoplasia and benign lesions.Iran J Med Sci 38(1), 15-21.
- 10.Mei P, Liu Y, Zhuang H. (2007) Diagnostic value of p16INK4a in squamous intraepithelial lesion in gynecologic cytology.ZhonghuaBing LiXueZaZhi. 36(8), 521-523.
- 11.Iaconis L, Hyjek E, Ellenson L H. (2007) P16 and Ki-67 immunostaining in atypical immature squamous metaplasia of the uterine cervix: correlation with human papillomavirus detection.ArchPatholLab Med. 131(9), 1343-1349.
- 12.Hariri J, Oster A. (2007) The negative predictive value of p16INK4a to assess the outcome of cervical intraepithelial neoplasia in the uterine cervix.IntJGynecolPathol. 26(3), 223-228.
- 13.Guo M, Warriage I, Mutyala B. (2011) Evaluation of p16 immunostaining to predict high-grade cervical intraepithelial neoplasia in women with Pap results of atypical squamous cells of undetermined significance.DiagnCytopathol. 39(7), 482-488.
- 14.Haidopoulos D, Partsinevelos G A, Vlachos G D. (2009) P16INK4A is a strong biomarker for cervical intraepithelial neoplasia and invasive cervical carcinoma: a reappraisal.ReprodSci Thousand Oaks Calif. 16(7), 685-693.
- 15.Miyamoto S, Hasegawa J, Morioka M, Hirota Y, Kushima M et al.The association between p16 and Ki-67 immunohistostaining and the progression of cervical intraepithelial neoplasia grade 2.International. , Journal ofGynecology& Obstetrics 134, 45-48.
- 16.Rogo K O, Omany J, Onyango J N. (1990) . , Carcinoma of the Cervix in the African Setting.IntJGynecolObstet 33(3), 249-255.
- 17.Ndikom C M, Ofi B A. (2012) Awareness, perception and factors affecting utilization of cervical cancer screening services among women in Ibadan, Nigeria: a qualitative study.ReprodHealth. 9, 11.
- 18.Ezem B. (2007) Awareness and uptake of cervical cancer screening in Owerri. , South-Eastern Nigeria.AnnAfrMed 6(3), 94-98.
- 19.RNK Adanu. (2002) Cervical cancer knowledge and screening in Accra. , Ghana.JWomensHealGendBased Med 11(6), 487-488.
- 20.O’Neill C J, McCluggage W G. (2006) p16 expression in the female genital tract and its value in diagnosis.AdvAnatPathol. 13, 8-15.
- 21.Venturoli S, Ambretti S, Mirasoli M. (2008) Chemiluminescent quantitative immunohistochemical p16 INK4A localization as a marker for cervical intraepithelial neoplasias.IntJGynecolPatholOff JIntSocGynecolPathol. 27(4), 575-581.
- 22.GRA Focchi, IDC Silva, Nogueira-de-Souza N C. (2007) Immunohistochemical expression of p16(INK4A) in normal uterine cervix, nonneoplastic epithelial lesions, and low-grade squamous intraepithelial lesions.J LowGenitTract Dis. 11(2), 98-104.
- 23.Ganesan R, Rollason T P. (2006) Pathology of neoplastic squamous lesions. In:Joseph A.Jordan and Albert Singer,ed.TheCervix.Second.Blackwell Publishing Ltd 301-316.
- 24.Queiroz C, Silva T C, VAF Alves. (2006) Comparative study of the expression of cellular cycle proteins in cervical intraepithelial lesions.PatholResPract. 202(10), 731-737.
- 25.Kava S, Rajaram S, V K Arora, Goel N, Aggarwal S et al. (2015) Conventional cytology, visual tests and evaluation of P16INK4A as a biomarker in cervical intraepithelial neoplasia. , Indian J Cancer 52, 270-5.
- 26.Murphy N, CCBB Heffron, King B. (2004) p16INK4A positivity in benign, premalignant and malignant cervical glandular lesions: a potential diagnostic problem.VirchowsArch anIntJPathol. 445(6), 610-615.
- 27.Duggan M A, Akbari M, Magliocco A M. (2006) Atypical immature cervical metaplasia: immunoprofiling and longitudinal outcome.HumPathol. 37(11), 1473-1481.
- 28.Qiao X, Bhuiya T A, Spitzer M. (2005) Differentiating high-grade cervical intraepithelial lesion from atrophy in postmenopausal women using Ki-67, cyclin E, and p16 immunohistochemical analysis.J LowGenitTract Dis. 9(2), 100-107.
Cited by (3)
This article has been cited by 3 scholarly works according to:
Citing Articles:
Ibnosina Journal of Medicine and Biomedical Sciences (2023) Crossref Semantic Scholar OpenAlex
Journal of the Scientific Society (2021) OpenAlex
Journal of Cancer Genetics and Biomarkers (2017) OpenAlex