The Therapeutic Effect of Bilateral Alternating Stimulation Tactile Form Technology on the Stress Response
Abstract
The application of bilateral alternating stimulation in tactile (BLAST) form technology, a non-invasive, somatosensory-based method, has been shown to modulate the electrical activity of brain networks that mediate the stress response, resulting in a stress-reducing effect in individuals with high reported levels of anxiety, such as post-traumatic stress disorder (PTSD). In this study, we examined archival data from a heterogeneous group of users (n = 1109) of BLAST technology via Touchpoints, a novel BLAST-based treatment modality, all of whom had high self-reported levels of stress and anxiety. Ratings of levels of emotional stress and bodily distress on a scale of 0 (no stress/distress) to 10 (worst stress/distress of one's life) before and after the application of Touchpoints for 30 seconds were entered into an app. Results showed a statistically significant reduction in the levels of both emotional stress and bodily distress, 62.26% and 50.502%, respectively, after 30 seconds of BLAST technology was applied. This demonstrates a clear benefit of BLAST on the stress response, reducing both emotional stress and disturbing body sensations. Recent work examining EEG changes after BLAST technology is applied suggests that BLAST may reduce sympathetic activation by reducing the electrical activity of key areas of the salience network. Further work will more precisely characterize the effects of BLAST, its potential clinical uses, and the mechanisms of actions behind it’s apparent stress-reducing effects.
Article Information
- Received
- Accepted
- Published
Academic Editor: Meili, School of Information Technology Engineering, Tianjin University of Technology and Education, Tianjin 300222, China.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2018 Amy Serin, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Nathan S. Hageman, David Geffen School of Medicine at UCLA, Los Angeles, CA —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Recent advances in neuroscience have allowed us to more clearly identify which parts of the human brain mediate particular behaviors or emotional states. With advances in medical imaging, we can identify structural and functional networks in the living human brain that are active during a specific task. We can also modulate these networks to produce changes in behavior or mood and achieve better therapeutic outcomes.
One particular method of changing the activity of certain brain networks associated with stress and anxiety is through a non-invasive somatosensory-based methodology, called Bilateral Alternating Stimulation in Tactile (BLAST) Form technology. Studies have shown that this therapeutic modality can aid in altering various brain functions and might be of therapeutic benefit to individuals with high or pathological levels of anxiety or stress 1, 2. The results from these studies using BLAST are consistent with the alternating hemispheric activation hypothesis 3, which postulates that rapidly alternating patterns of electrical activity in the two hemispheres might increase inter-hemispheric interaction.
Of considerable interest is the effect of BLAST on the amygdala and its associated networks, given how closely they are linked to feelings of anxiety and stress. An electroencephalogram (EEG) is a non-invasive form of data collection, which evaluates electrical activity in the brain and tracks brain wave patterns. An EEG study by Harper et al., 2009 on subjects with PTSD found that BLAST had a de-potentiation effect on those synapses in the amygdala that are active during the recall of fear-based memories 4. Archival EEG data gathered by our group suggest that, when BLAST is applied, there are significant changes in electrical activity in the amygdala, insula, and somatosensory cortex, as measured by EEG. These results suggest that BLAST may have an effect on the electrical activity in key brain areas associated with stress and anxiety and whose overall effect may de-escalate the human stress response and also lessen or eliminate bodily sensations associated with distressing recall or physical pain.
In particular, the amygdala (and, to a lesser extent, the insula) has been identified as part of the salience network, which is thought to modulate the brain's reaction to stress and create an appropriate behavioral response 5, 6, 7. It's principle cortical and sub-cortical nodes include the anterior cingulate cortex, anterior insula, amygdala, ventral tegmental area, and the ventral striatum. There is strong evidence linking defects in the salience network with many major psychiatric disorders, including generalized anxiety disorder, panic attacks and PTSD 8, 9. Previous studies, along with recent work by our group showed quantitative EEG changes (i.e., amygdala, insula, and somatosensory cortex) in subjects after treatment with BLAST, suggest that the stress-reducing effect of BLAST on the stress response may be due in part to its effect on reducing electrical activity in the salience network, responsible for sympathetic arousal and inducing the body’s physiological stress response.
These findings motivated us to examine archival data to quantify the effects of BLAST technology to consumers setting for individuals who report high levels of stress and disturbing body sensations. Specifically to determine whether the somatosensory application of BLAST can effectively reduce subjective ratings of stress and related physiological body sensations. In this paper, we look at the effect of BLAST on the emotional and physical manifestations of the stress response in individuals before and after treatment with Touchpoints, a novel BLAST-based treatment modality.
Materials and Methods
Subjective ratings of emotional stress level and physical sensations of bodily distress were submitted through a software app by 1109 subjects, adults aged 21-47, who purchased Touchpoints commercially. Individuals were asked to rate their levels of emotional stress and bodily distress on a scale of 0 (no stress/distress) - 10 (worst stress/distress of their lives), before and after using Touchpoints for 30 seconds and submit their answers through the provided software app.
We employed a paired t-test to assess the likelihood that the null hypothesis is valid (i.e. that the mean difference of the experimental and control groups are actually calculated from two samples of the same single population). The test statistic, T, was calculated as follows:
where SE(d) is the standard error of the mean of the difference between the paired values, d=

for n total pairs and are the two observations of the ith pair and is defined as
where sd is the sample standard deviation of the mean of the difference between the n paired values.
The degrees of freedom corresponding to this test statistic, df, are defined as (df = (n – 1) = 1108). A p-value < 0.05 was taken to be statistically significant.
Results
The average ratings from (0 no stress/distress – 10 worst stress/distress of subject's life) across 1109 subjects for emotional stress (Table 1; Figure 1) and bodily distress (Table 1; Figure 2) before (observation1 of pair) and after 30 seconds (observation2 of pair) of treatment with BLAST are shown below. Subjects, after treatment with BLAST, showed a mean reduction in the rating of their level of emotional stress by 62.26% and a mean reduction in the rating of their level of bodily distress by 50.502%.
Table 1. Mean and standard deviation (Sd) of the ratings from (0 no stress/distress – 10 worst stress/distress of subject's life) of the level of before (A) and afer (B) emotional stress across; and before (C) and after (D) bodily distress across all subjects (n=1109) 30 seconds of treatment with BLAST via Touchpoints.| (A) Before BLAST | (B) After BLAST | (C) Before BLAST | (D) After BLAST | |
| Mean | 7.65 | 2.89 | 5.21 | 2.58 |
| Sd | 2.08 | 2.76 | 3.18 | 2.76 |
Figure 1. Mean and standard deviation of the ratings from (0 no stress/distress – 10 worst stress/distress of subject's life) of the level of emotional stress across all subjects (n=1109) before (A) and after (B) 30 seconds of treatment with BLAST via Touchpoints.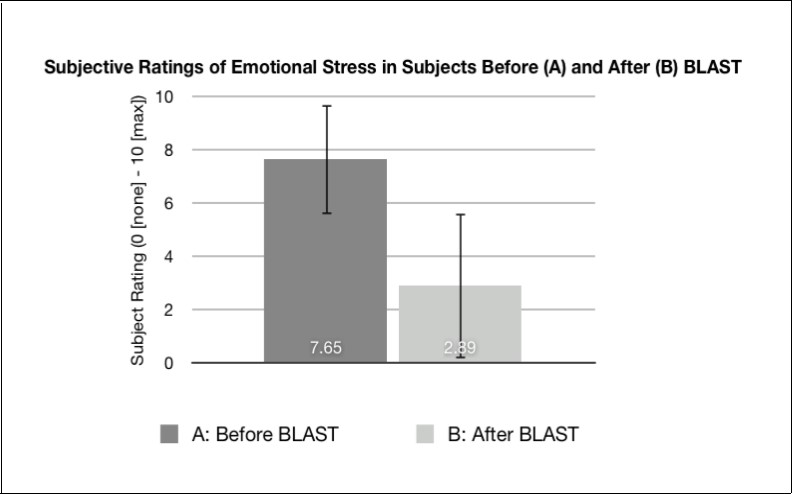
Download figure
Figure 2. Mean and standard deviation of the ratings from (0 no stress/distress – 10 worst stress/distress of subject's life) of the level of bodily stress across subjects (n=1109) before (A) and after (B) 30 seconds of treatment with BLAST via Touchpoints.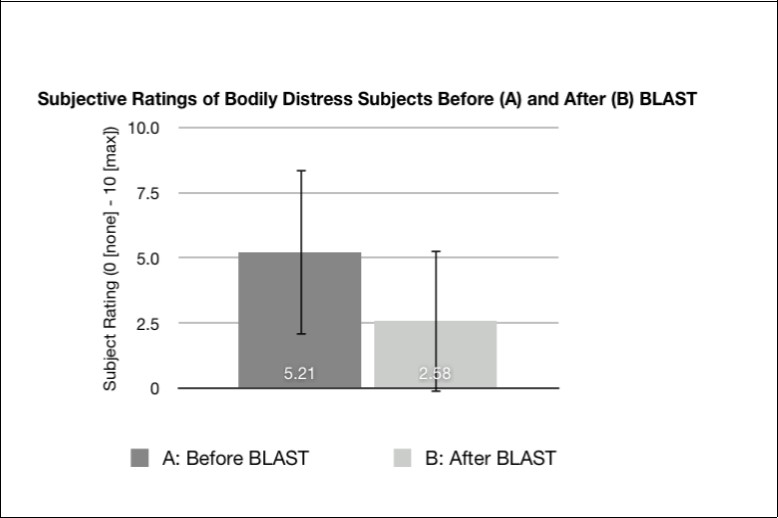
Download figure
To determine whether these reductions in the stress response are statistically significant, the means of the paired difference of each subject’s rating of their level of stress/distress before and after using Touchpoints (BLAST) for 30 seconds were compared using a paired t-test. Results are shown below in Table 2 (emotional stress) and Table 2 (bodily distress). Both of these values of the test statistic, T, are above the cut-off value for p < 0.05 (~1.645 at infinite degrees of freedom). In fact, the p values for the mean reductions in levels of emotional stress and bodily distress are both < 0.0001. Thus, the reductions in the levels of emotional stress and bodily distress after treatment with BLAST are statistically significant.
Table 2. Test statistic and related values for mean paired difference of the subject's rating of their level of emotional stress and bodily stress before (1) and after (2) treatment with BLAST.| Emotional Stress | Bodily Stress | |
| Mean of the paired difference (d) | 4.76 | 2.63 |
| Sample Standard Deviation of d ( s d ) | 3.10 | 3.23 |
| Standard Error of d | 0.0931 | 0.0971 |
| Degrees of freedom, df | 1108 | 1108 |
| Test statistic, T | 51.16 | 27.12 |
| P value | <0.0001 | <0.0001 |
Discussion
Although BLAST has been used many times as a component of eye movement desensitization and reprocessing (EMDR) therapy and many research studies have demonstrated significant changes in both subjective and objective metrics post-treatment with BLAST, it appears to be vastly underutilized as a method for inhibiting the body’s stress response 10, 11. Multiple previous research articles and clinical reports indicate that BLAST can effectively reduce both psychological and physiological pain and distress, enhance memory retrieval, and promote sleep and feelings of calm 12, 13, 14. Because BLAST is relatively inexpensive and has been incorporated into portable devices, it provides a simple, low cost, non-invasive, method to alter the body's negative stress response and improve functioning. This has motivated the construction and clinical use of Touchpoints (patent-pending), a novel device which allows a patient to apply BLAST as either a method of stress-reduction on its own, or as an adjunct to therapy and other medical treatments.
The results above show that a group of individuals (n = 1109) who used BLAST technology in Touchpoints for 30 seconds show a statistically significant reduction in their level of emotional stress and sensations of bodily distress (i.e. breathing difficulty, chest pain, stomach ache), demonstrating a clear benefit. Although BLAST was delivered for 30 seconds for purposes of collecting data, duration is often increased in clinical treatment settings. This clinical result is supported by recent work by our group (not presented here) showing significant quantitative EEG changes in subjects after application of BLAST in brain areas known to be part of the salience network (i.e. amygdala, insular cortex, and somatosensory cortex). It is postulated that the salience network is thought to modulate the brain’s reactivity to stress and to create appropriate behavioral responses to both internal and external sensory information 8, 9. The results presented here show that the application of BLAST leads to a clear clinical reduction in feelings of emotional stress and bodily distress, both of which are manifestations of the stress response. In addition, the quantitative EEG changes in key areas of the salience network that occur after BLAST use may explain why BLAST seems to de-escalate whatever stress response is already occurring, and how it can lessen or eliminate distressing body sensations associated with recall of memories that involve emotional distress or physical pain 14, 15. We cannot determine how long after BLAST an individual may experience cognitive and physiological symptoms of anxiety again, as this is highly variable per individual. However, the individual will be less inclined to become as stressed about the subjective unit of stress post using BLAST as it appears to have a residual effect. In addition, ratings were highly subjective, and level of distress is likely to vary per individual. However, we notice that regardless of where the subjective rating began, it significantly decreased; therefore, it is less important as how accurate these ratings are as to how the individual subjectively is perceiving less feelings of stress post-BLAST. Further and more rigorous clinical studies need to be pursued to fully characterize therapeutic effects of BLAST and determine how they are mediated.
This study had some limitations. In particular, since the archival data was gathered through a software app without oversight or guidance, we cannot be sure how effectively or correctly the Touchpoints were used by each subject. In addition, subjects were not blinded to the treatment, so we cannot discount bias or belief. There were also no age/demographics matching across subjects and no exclusion criteria so we cannot be sure if our results are being altered by these factors or to what degree. To address these limitations, we are pursuing double-blind, placebo-controlled studies of the effect of BLAST on the stress response. Nevertheless, the above results are promising that BLAST and Touchpoints could be an effective therapeutic tool to reduce a pathological stress response, either by itself or as an adjunct to psychotherapy.
Conclusion
We showed that the application of BLAST using Touchpoints for 30 seconds resulted in a statistically significant reduction in a subject's levels of emotional stress and feelings of bodily distress. These results demonstrate a clear stress-reducing effect and suggest that BLAST may be an effective, non-invasive method for reducing stress and anxiety. Further work is needed to fully characterize this stress-reducing effect of BLAST and determine its therapeutic applications.
References
- 1.Servan-Schreiber D, Schooler J, M A Dew, Carter C, Bartone P. (2006) Psychotherapy and Psychosomatics. 75(5), 290-297.
- 2.Nieuwenhuis S, B M Elzinga, P H Ras, Berends F, Duijs P et al. (2013) Brain and cognition. 81(1), 52-56.
- 8.Menon V, A W Toga. (2015) Brain Mapping:An Encyclopedic Reference,Vol 2,Academic Press: Elsevier,San Diego,CA.
- 11.Pagani M, Högberg G, Fernandez I, Siracusano A. (2013) . , Journal of EMDR Practice and Research 7(1), 29-38.
- 12.Wurtz H, El-Khoury-Malhame M, F H Wilhelm, Michael T, E M Beetz et al. (2016) . , Neuroscience 321, 222-235.
Cited by (19)
This article has been cited by 19 scholarly works according to:
Citing Articles:
International Journal of Human-Computer Studies (2025) OpenAlex Crossref
Journal of Cognitive Psychology (2025) OpenAlex Semantic Scholar Crossref
(2024) OpenAlex Semantic Scholar
Pediatric Rheumatology (2024) OpenAlex Semantic Scholar Crossref
Research Square (Research Square) (2024) OpenAlex
Lecture notes in networks and systems (2024) OpenAlex
PLoS ONE (2022) OpenAlex Semantic Scholar Crossref
(2022) OpenAlex
Occupational Therapy In Health Care (2021) OpenAlex Semantic Scholar Crossref
IEEE Access (2020) OpenAlex Semantic Scholar Crossref
Journal of Biotechnology and Biomedical Science (2019) OpenAlex Semantic Scholar Crossref
Springer eBooks (2019) OpenAlex Semantic Scholar
Sensors (2018) OpenAlex Semantic Scholar Crossref
Connie J. McReynolds, Lelah S. Villalpando, Cynthia E. Britt - NeuroRegulation (2018) Semantic Scholar