
A Model-Based Estimation of Annual Long-Term Care Costs in Germany Following Post-Operative Cognitive Dysfunction (POCD) in Elderly Patients
Abstract
Acute post-operative delirium (POD) and long-term post-operative cognitive dysfunction (POCD) are frequent and associated with increased mortality, dependency on care giving and institutionalization rates. The POCD-related cost burden on the German long-term care insurance provides an indication for the savings potential from risk-adapted treatment schemes. Comprehensive estimates have not been assessed or published so far.
A model-based cost-analysis was designed to estimate POCD-related costs in the long-term care insurance. Comprehensive analysis of inpatient operations and procedures (OPS-codes) served as the base for case number calculations, which were then used as input to the actual cost model. POCD-incidence rates were obtained from the BioCog study. Various sensitivity analyses were performed to assess uncertainty of the model results.
Total POCD related annual costs in the German long-term care insurance account for approximately 1.6 billion EUR according to the base case of our analysis. Total annual costs for all POCD cases depend on surgery numbers, incidence rates, other assumptions, and uncertain input parameters.
The financial burden to the long-term care insurance is substantial, even in a conservative scenario of the cost model. Variability of results stems from uncertain assumptions, POCD-incidence rates and from uncertain patient numbers who are undergoing surgery and are therefore at risk to develop POCD.
Article Information
- Received
- Accepted
- Published
Academic Editor: Sasho Stoleski, Institute of Occupational Health of R. Macedonia, WHO CC and Ga2len CC , Macedonia.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2021 Simon A. Weber, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Simon Weber, Cellogic GmbH, Niedstrasse 21, 12159 Berlin —
Competing Interests
The authors have declared that no competing interests exist.
Funding
The research leading to these results has received funding from European Union funded Seventh Framework Research Program FP7/2007–2013, under grant agreement No. HEALTH-F2-2014-60246, BioCog (Biomarker Development for Postoperative Cognitive Impairment in the Elderly), www.biocog.eu.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
The long-term care insurance (“Pflegeversicherung”) in Germany is financed by income-dependent charges of the national workforce and experienced significantly increasing expenditures during the last years. From 2013 until 2019 they increased from 23.2 billion EUR to 40.7 billion EUR, which represents an increase by nearly 75% 1. The increase in expenditures can be explained by an expansion of services which are paid by the long-term care insurance as well as the demographic development of the German population, which is characterized by an increase in the older population 2. In light of potential future losses incurred by the long-term care insurance, the need for cost reductions becomes obvious. Cost implications stemming from other sectors of welfare state, e.g. the health care sector, become increasingly important in this context.
Post-operative cognitive dysfunction (POCD) is a frequently occurring complication after surgeries, not only but especially among elderly patients aged 65 years and above 3, 4. It can be described as a relative decline in patients` cognitive function following surgery compared to pre-surgery and might trigger dependency on care giving in a substantial share of elderly patients. Post-operative delirium (POD) is in many cases preceding a temporary or even sustained POCD 5, 6, 7. This is especially the case when several risk-factors like pre-OP dementia, or other pre-existing comorbidities are present 8, 9. As a result, many patients remain dependent on care giving after the initial hospitalization either temporarily or permanently. In light of the high operation numbers in elderly patients aged 65 years and above in Germany (>6.4 mio in 2019), who often carry a number of POCD risk factors, the long-term care burden stemming from POD and subsequent POCD has not been comprehensively assessed and published to date but might be substantial.
It is worth noticing that the existing nomenclature for perioperative cognitive deficits has recently been revised and the Nomenclature Consensus Working Group has made recommendations for a refined naming of perioperative cognitive dysfunctions 10. According to their recommendation neuro-cognitive disorders (PNDs) should be defined differently depending on the time of diagnosis in the perioperative period in order to better distinguish them from neurocognitive disorders of other genesis. Preoperative neurocognitive disorders are referred as mild / major neurocognitive disorders (NCD) or pre-existing cognitive impairment (PreCI). If a neurocognitive disorder occurs during the early postoperative intra-hospital phase, it is defined as emergence delirium (e.a. agitation after first awakening) and postoperative delirium (POD). If there is delayed cognitive recovery in the in-patient and post-hospital setting until 30 days after the operation, this condition can be described as delayed neurocognitive recovery (dNCR). All postoperative neurocognitive disorders that persist for more than 30 days are referred as "mild / major NCD (postoperative)" (formerly known as POCD). To emphasize the clinical association of NCD after surgery, the term "postoperative" is used for up to one year after surgery. Outside this period suffix “postoperative” is omitted. In the present analysis, we are focusing on POD and postoperative neurocognitive disorders that persist for more than 30 days and define the latter as POCD, because we will not differentiate between mild and major NCD.
Primary aim of the BioCog consortium is the development of a prospective diagnostic tool, capable of reliably predicting POD and POCD risks of patients, in order to either individually adapt and improve post-operative care or to suspend and potentially discard the initially planned surgery. For this purpose, the BioCog consortium conducted an observational study to identify suitable biomarkers by including more than one thousand patients in Berlin, Germany and Utrecht, Netherlands aged 65 years and above, undergoing an inpatient major elective surgery with general anesthesia. Specifics of the BioCog study design are reported elsewhere 11. Final study results have been submitted for publication. For the present study we used age-specific incidence rates of POCD observed in the BioCog trial, to estimate post-operative long-term care costs associated with POCD.
In anticipation of the prospective diagnostic POCD risk prediction tool we seek to determine parts of the possible market size of such a tool in terms of EUR. To estimate the health-economic value of the proposed pre-operative assessment it is essential to also consider downstream costs associated with POCD, which could potentially be avoided. A major share of these downstream costs is suspected to be incurred by the long-term care insurance in Germany due to sustained POCD of a significant proportion of patients.
Health-economic literature on POD - and POCD-related costs is scarce, especially literature on costs borne by long-term care insurances. According to published studies in the field of health-economics, it could be shown that POD significantly contributes to increased inpatient costs 12, 13, 14. It has been reported that new onset of delirium during hospitalization was associated with additional inpatient costs of approximately 1300 EUR compared to non-delirium cases in Germany, with the majority of additional costs (approximately 60%) stemming from increased inpatient nursing personnel costs 14. Budget impact estimates of POD and subsequent POCD state total direct 1-year health care costs for the US between $143 billion to $152 billion 15.
Analyses of the financial burden of POCD to the German long-term insurance caused by premature dependency on care giving could not be found in the present literature. There is a lack of published, transparent, and reproducible estimates of the long-term care burden in Germany attributable to POD/POCD, especially within the new framework of “Pflegegrade” – a formal system which assigns a patient to one out of five categories depending on the degree of long-term care intensity. The BioCog group therefore decided to develop a health-economic model estimating the cost-consequences attributable to POCD for the German long-term care insurance, based on the BioCog trial results and other published data.
Methods
Model-Structure
The health-economic model was specifically designed to estimate annual long-term care costs in Germany in 2019 attributable to POCD in patients aged 65 and above, undergoing an inpatient surgery. Using this case-definition we are aiming to reflect the patient population of the BioCog study and leverage the results to the national level.
Input Parameters (Variables)
A combination of age-specific incidence rates from the BioCog study and officially available operation and procedure numbers is used to obtain numbers of affected patients who experience POCD and are post-operatively dependent on long-term care giving in Germany. Combining the number of affected patients with officially available long-term care insurance payments yields annual long-term care burden in a reproducible and transparent manner.
The model is implemented in Microsoft Excel and the model structure was developed in order to suit the main input data, which is publicly available. The model structure is illustrated in Figure 1. Major inputs include:
Figure 1. Model Structure
Download figure
Age-specific POCD incidence rates observed in the BioCog study
Age-specific operation numbers, that were retrieved from national German hospital-statistics 16 to obtain the number of patients who undergo inpatient surgeries
Monthly payments and absolute numbers of patients receiving long-term care in three different types of long-term care schemes (outpatient care by relatives, outpatient care by professionals, inpatient care) and on 5 different levels of long-term care intensity (so called “Pflegegrade”)
The modelled scenario uses a set of age specific POCD incidence rates derived from the results of the BioCog study. The incidence rates are based on a strict definition of POCD according to the ISPOCD criteria proposed by Rasmussen 17. This definition includes all patients developing POCD independently of a potentially preceding POD. Resulting POCD cases are assumed to be dependent on care giving and trigger long-term care costs. In order to account for uncertainty of the chosen input parameters, sensitivity analyses were performed for several input variables.
Intervention numbers – Analysis of Chapter 5 OPS-Codes in Germany
To determine the amount of patients aged 65 and above undergoing surgery and who are therefore at risk for POCD, official German hospital statistics in 2019 16 and a sub-sample of the BioCog study were used. The German OPS statistic is part of the German hospital statistic (DRG statistic) and lists the number of all operations and procedures applied to patients in German hospitals, based on the OPS classification system for reimbursement purposes. Chapter 5 of the OPS statistic lists all operations applied on patients and was used for the following analyses.
As a first step, all chapter 5 OPS-codes were corrected for all supplementary codes (“Zusatzcodes”), that are used in practice to further specify operations (e.g. number of stents implanted etc.) and do not represent separate surgeries. In total we excluded 406 supplementary codes, representing more than 1mio entries in the age group of 65 years and above.
Among the corrected number of chapter 5 OPS-codes, 43% of the entries are reported for patients aged 65 and above. Patients aged between 75 and 79 years represent the group with the highest amount of chapter 5 OPS-codes in 2019 (Figure 2). In total, around 6.4mio chapter 5 OPS-codes are reported in our patient target group (patients aged 65 and above).
Figure 2. Shares of considered patient numbers per age-group in OPS and BioCog samples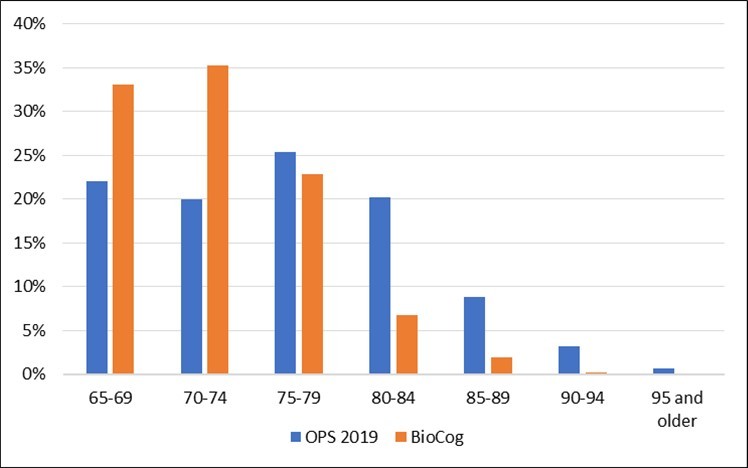
Download figure
Intervention numbers – Analysis of chapter 5 OPS-codes in BioCog sub-sample
The analysis of chapter 5 OPS-codes described above was repeated for a sub sample of the BioCog study (n=662), representing all patients recruited in Berlin, Germany. The aim of this analysis was to identify the average amount of chapter 5 OPS-codes reported per patient, that we would subsequently apply to the total amount of relevant chapter 5 OPS-codes reported for Germany to estimate the number of patients undergoing surgery in 2019 on the national level. Using this methodology, we identified 2438 chapter 5 OPS-codes that were recorded for 662 patients included in the BioCog sample. On average, one patient was represented with 3.68 chapter 5 OPS-codes in this sub-sample of the BioCog study.
In a next step we divided number of chapter 5 OPS-code entries in the German hospital statistic by the average number of 3.68 chapter 5 OPS-codes per patient, to estimate the total amount of patients undergoing surgery in Germany. The result is displayed in Table 1 for patients aged 65 years and above in each age group.
Table 1. Estimated number of patients undergoing surgery per age-group| Base Case | Age groups | ||||||
| 65-69 | 70-74 | 75-79 | 80-84 | 85-89 | 90-94 | 95 and older | |
| Amount of chapter 5 OPS-codes | 1,416,395 | 1,279,235 | 1,626,461 | 1,294,527 | 563,399 | 199,934 | 39,234 |
| Patients undergoing surgery | 384,599 | 347,356 | 441,640 | 351,508 | 152,982 | 54,289 | 10,653 |
Comparison of the OPS- and the BioCog Samples
Combining derivatives from two different samples with the aim of estimating representative results requires consideration of relevant differences between the samples. We therefore compared both samples with regards to observable factors that are likely to have an impact on the POCD incidence rates and that represent important inputs to the cost model.
(Figure 2) shows the shares of included patients per age-group in both samples. It can be seen by visual inspection that the BioCog sample, from which we obtained POCD incidence rates and the average number of chapter 5 OPS-codes per patient, represents a younger cohort than the OPS 2019 sample. Consequences of this mismatch are discussed in section Discussion of Results.
Furthermore, we aimed to compare the two samples with regards to the site of the underlying surgeries, since this is a factor perceived to have an influence on POCD incidence. The analysis of the OPS 2019 sample involved analyzing 19,825 different OPS-codes and no automated classification of the codes into the groups (i) intracranial, (ii) intrathoracic, -abdominal, -pelvic and (iii) peripheral was feasible. Therefore, we focused on analyzing the TOP-50 OPS-codes (based on the first 4 digits) that were mostly reported and represent 58% of all reported OPS-codes in patients aged 65 years and above. This step required classification of 2935 single OPS-codes (based on the full number of digits). The resulting distribution of operations to the 3 site-classes is shown in Table 2.
Table 2. Site of Surgeries in Samples used| Intracranial | Intrathoracic, -abdominal, -pelvic | Peripheral | |
| OPS 2019 | 7% | 44% | 49% |
| BioCog | 1% | 44% | 55% |
The shares of intrathoracic, -abdominal, and -pelvic operations exactly match between the two samples. The share of intracranial operations is slightly higher in the German OPS-sample and the share of peripheral operations is slightly higher in the BioCog sample.
Incidence Rates – Definition of POCD in BioCog Trial
For the calculation of age-specific incidence rates, we used respective results from the BioCog study 11. In this study, POCD assessment consisted of a comprehensive neuropsychological test battery (CANTAB, Cambridge Cognition Ltd.) performed at baseline before surgery, at discharge and at three months after surgery. Repeated cognitive tests typically trigger learning effects in a patient, which also influence test results. To account for these effects, POCD was defined according to the ISPOCD criteria proposed by Rasmussen 17 that put a patients change in cognitive function in relation to the change in a non-surgical control group.
In short, for each cognitive test parameter (CTP), the corresponding Reliable Change Index (RCI) has been calculated as RCI=(ΔX-ΔXc)/(SD (ΔXc)). ΔX refers to the difference in test score after surgery compared to before and ΔXc refers to the mean test score difference between the two consecutive measurements in a non-surgical control group. RCI is normalized to the standard deviation of mean differences in the control group SD (ΔXc). A compound RCI for each patient was defined as the sum of all RCIs in relation to the standard deviation of the sum of RCIs in the control group (RCIc): compound RCI=(∑(RCI))/(SD ∑(RCIc)). A subject was considered to suffer from POCD when the difference between post- and pre-operative cognitive function was lower than 2 standard deviations from the mean of the reference control group, as recommended by Rasmussen et al., 2001. The implementation of this POCD definition in the R package ‘POCDr’ has been described by Spies et al. in a previous publication. Note: In recently published recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery, more liberal cut-off points (between 1 and 2 standard deviations) have been suggested 10.
Age-Specific Incidence Rates of POCD
Estimating the total amount of patients experiencing POCD and therefore entering the cost-model, was performed by applying age-specific incidence rates to the estimated number of patients undergoing surgery (see above). For our base case scenario, POCD-incidence rates were obtained from 641 patients enrolled in the BioCog study for whom POCD data at month 3 were available and complemented by an exponential extrapolation for the two age groups 90-94 and 95 and above, because there were only two enrolled patients and no POCD cases were observed in the BioCog study in these two age groups. The extrapolated value for the age-group 95 and above was cut-off at 100%. A graphical representation of the applied incidence rates is shown in Figure 3.
Figure 3. POCD incidence rates per age-group applied in the cost model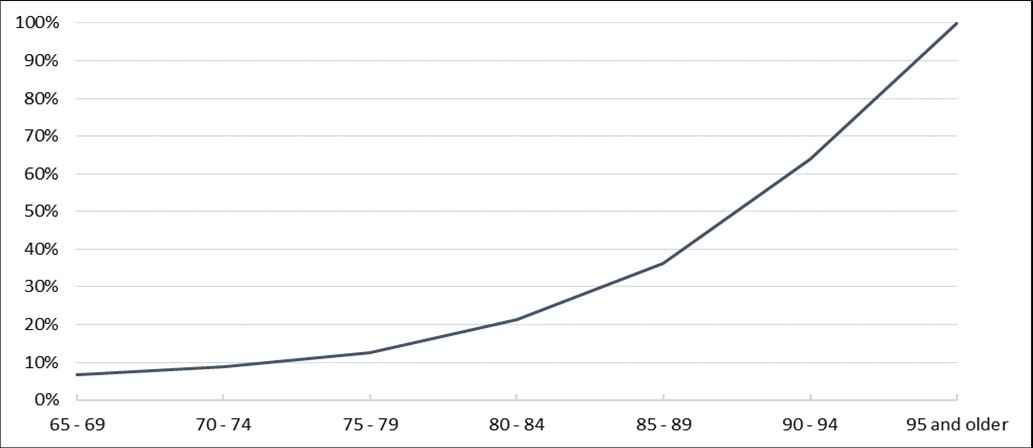
Download figure
POCD Case Numbers
Combining the estimated patient numbers obtained from the OPS analysis and the POCD incidence rates from BioCog yields the total amount of POCD cases that is calculated within the model framework and serves as the base for long-term care cost estimations. Details of these calculations can be found in Table 3.
Table 3. Calculated POCD cases entering the cost-estimations| Base Case | Age groups | ||||||
|---|---|---|---|---|---|---|---|
| 65-69 | 70-74 | 75-79 | 80-84 | 85-89 | 90-94 | 95 and older | |
| Patients undergoing surgery | 384,599 | 347,356 | 441,640 | 351,508 | 152,982 | 54,289 | 10,653 |
| POCD incidence rates | 6.8% | 8.8% | 12.6% | 21.3% | 36.4% | 64.0% | 100.0% |
| Resulting POCD cases | 26,223 | 30,739 | 55,614 | 74,789 | 55,630 | 34,726 | 10,653 |
| Total amount of POCD cases | 288,375 | ||||||
Referring to the base case of the presented model, a total number of more than 288,000 cases is calculated to experience POCD in 2019 and entered our cost extrapolation.
Inputs from Long-Term care Insurance and Validation
Based on the estimated number of POCD cases, monetary costs to the long-term care insurance in 2019 are calculated. These cost parameters in the model are obtained from official sources and distinguish the type of long-term care and the degree of long-term care intensity. Standard monthly costs per person to the long-term care insurance are publicly available and are displayed in Table 41.
Table 4. Monthly costs to long-term care insurance per person| Costs - Outpatient long-term care | Costs - Inpatient long-term care | ||
| Pflegegrade | Outpatient long-term care by Relatives | Outpatient long-term care by Professionals | Inpatient long-term care |
| Pflegegrad 1 | 0 € | 0 € | 125 € |
| Pflegegrad 2 | 316 € | 689 € | 770 € |
| Pflegegrad 3 | 545 € | 1,298 € | 1,262 € |
| Pflegegrad 4 | 728 € | 1,612 € | 1,775 € |
| Pflegegrad 5 | 901 € | 1,995 € | 2,005 € |
The assessment of long-term care intensity within the German nursing care insurance is a complex process, accounting for various factors such as mobility, cognitive abilities, psychological problems, self-reliance, dealing with disease-specific challenges, aspects of everyday life and social contacts. During the assessment a patient is assigned to different amount of points in each of the aforementioned domains by an independent assessor. According to the total amount of points, a patient is then assigned to long-term care intensity 1 to 5 (Pflegegrad 1 to 5). Due to a lack of published studies on the long-term care dependency resulting from POCD within the framework of Pflegegrade (legally introduced in 2017), we implemented the assumption that a new POCD case will transition from long-term care intensity 0 (no dependency on care-giving) to long-term care intensity 2 (Pflegegrad 2), which represents a low level of dependency on care-giving. This assumption is in line with the fact, that patients who were grouped into degree 0 or 1 (Pflegestufe 0 and 1) according to the former long-term care intensity definition before 2017 (Pflegestufen), would today be grouped into intensity 2 (Pflegegrad 2).
Long-term care intensity 2 (Pflegegrad 2) is therefore highlighted in Table 4, because we modelled the additional costs to the long-term care insurance stemming from a switch from intensity 0 (zero costs) to intensity 2 (Pflegegrad 2) as a conservative estimate. The German long-term care insurance grants compensation payments to relatives providing care as so called long-term care money (Pflegegeld). We denote this long-term care scheme as outpatient long-term care by relatives. A patient, who is otherwise dependent on outpatient long-term care, is eligible for receiving compensation payments (“Pflegesachleistungen”) which can only be spent for outpatient long-term care by professionals. The third major long-term care scheme, which is reflected in our model, is denoted as inpatient long-term care.
The absolute amount of patients receiving long-term care services in each long-term care type and intensity is available from another official source 18. We used this statistic for two purposes: (a) for a validation of model consistency and (b) for determining relative shares of patients in long-term care intensity 2 (Pflegegrad 2), which we used to estimate costs associated with a switch from intensity 0 to 2.
The model validation aimed at reproducing total expenditures of the long-term care insurance by multiplying the amount of patients receiving long-term care in each cell (long-term care type and intensity) by the monthly payments of the long-term care insurance (see Table 4). Following this rationale, we could reproduce around 90.5% of total expenditures and interpret this result as a consistent validation. The remaining difference of 9.5% of total expenditure can be explained by many additional services provided by long-term care insurance that have a financial impact, but which are not considered in our model. These include payments for technical long-term care aids (“Pflegehilfsmittel”), support for improvements in home environments (“Wohnumfeldverbesserungs-maßnahmen”), transfer payments to pension funds, unemployment insurance, health insurances and other legal financial support of the long-term care insurance. The numbers of patients receiving long-term care and the resulting reproduction of total expenditures can be found in Table 6 and Table 7.
Table 5. Base Case Model Results| Costs - Outpatient long-term care | Costs - Inpatient long-term care | |||
| Annual POCD-Cases | Outpatient long-term care by Relatives | Outpatient long-term care by Professionals | Inpatient long-term care | Sum |
| 288,375 | 720,057,563 € | 599,296,954 € | 240,259,590 € | 1,559,614,106 € |
| Source: Pflegestatistik - Pflege im Rahmen der Pflegeversicherung, Deutschlandergebnisse, 2019 | ||||
| Outpatient long-term care | Inpatient long-term care | |||
| Long-term care degree | Outpatient long-term care by Relatives | Outpatient long-term care by/with Professionals | Inpatient long-term care (excl. Non-classified patients) | Sum |
| Pflegegrad 1 | 0 | 81,363 | 6,521 | 87,884 |
| Pflegegrad 2 | 1,182,632 | 451,432 | 161,942 | 1,796,006 |
| Pflegegrad 3 | 644,501 | 289,492 | 281,765 | 1,215,758 |
| Pflegegrad 4 | 216,579 | 115,886 | 240,680 | 573,145 |
| Pflegegrad 5 | 72,739 | 44,431 | 124,473 | 241,643 |
| Sum | 2,116,451 | 982,604 | 815,381 | 3,914,436 |
| Outpatient long-term care | Inpatient long-term care | |||
| long-term care degree | Outpatient long-term care by Relatives | Outpatient long-term care by Professionals | Inpatient long-term care | Sum |
| Pflegegrad 1 | - € | - € | 9,781,500 € | 9,781,500 € |
| Pflegegrad 2 | 4,484,540,544 € | 3,732,439,776 € | 1,496,344,080 € | 9,713,324,400 € |
| Pflegegrad 3 | 4,215,036,540 € | 4,509,127,392 € | 4,267,049,160 € | 12,991,213,092 € |
| Pflegegrad 4 | 1,892,034,144 € | 2,241,698,784 € | 5,126,484,000 € | 9,260,216,928 € |
| Pflegegrad 5 | 786,454,068 € | 1,063,678,140 € | 2,994,820,380 € | 4,844,952,588 € |
| Sum | 1,378,065,296 € | 11,546,944,092 € | 13,894,479,120 € | 36,819,488,508 € |
Assumptions
To finally calculate the financial burden to the long-term care insurance associated with POCD some major assumptions need to be made, when using the publicly available input data outlined above. These assumptions include:
A POCD case triggers an individual transition from long-term care intensity 0 (Pflegegrad 0, no dependency on care giving) to long-term care intensity 2 (Pflegegrad 2, low dependency on care giving).
Occurrence of POCD and associated consequences do not alter the patient distributions between long-term care types (outpatient care giving by relatives, ambulatory services, or inpatient care).
Potential dependency on long-term care as consequence of POCD occurs in the same fiscal year as the analyzed and included patient numbers (2019).
Considered cases are limited to patients aged 65 and above. All patients developing POCD and subsequent dependency on care giving below the age of 65 are not accounted for in this model.
Results
The results of the base case are displayed in Table 5. Case numbers were calculated as described above and yield a total of 288,375 POCD cases annually. Applying monetary costs of the long-term care insurance in the different types of long-term care schemes described above, yields annual costs triggered by POCD of approximately 1.6 billion EUR in the base case of the model. The relative distribution of POCD related costs across long-term care schemes is shown in Figure 4. The highest share of costs (46%, or approximately 60mio EUR) is devoted to long-term care money (Pflegegeld) as compensation for relatives providing care. Care provided by professionals in an outpatient setting accounts for 38% and inpatient care for 15% of calculated additional costs.
Figure 4. Relative distribution of POCD-related costs across nursing schemes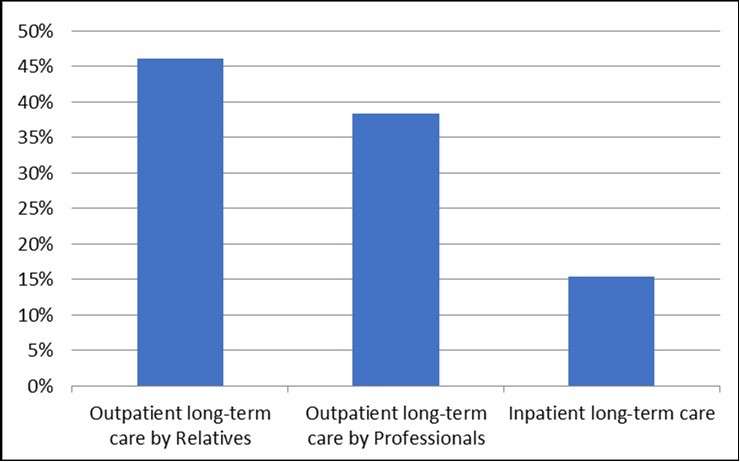
Download figure
Several deterministic sensitivity analyses were performed, and the results are shown in a tornado diagram (Figure 5) to investigate the uncertainty surrounding the model results. We in- and decreased the age-specific incidence rates and the average amount of OPS-codes per patient by +/-10% and recalculated the relevant POCD cases and additional costs with the aim to evaluate the effect of uncertain and varying POCD case numbers. In addition, we investigated the effect of assuming half of the POCD cases transitioning from long-term care intensity 0 to 1 and from intensity 0 to 3 instead of assuming all POCD cases transitioning from intensity 0 to 2.
Figure 5. Results of deterministic sensitivity analyses (Tornado Diagram)
Download figure
Regarding the three chosen parameters and assumptions, it becomes obvious that the highest share of uncertainty surrounding the model results stems from the assumption of all POCD cases transitioning from long-term care intensity 0 to 2. Assuming half of the POCD cases transitioning from care intensity 0 to 1 and the other half from 0 to 2 would decrease annual costs to the long-term-care insurance to approximately 796mio EUR. On the other hand, assuming half the POCD cases transitioning from care intensity 0 to 3 and the other half again from 0 to 2 would increase total costs to 2.3 billion EUR.
While a 10% in- or decrease in POCD incidence rates directly translates into a 10% in- or decrease in total long-term care costs, a corresponding in- and decrease of the average amount of chapter 5 OPS-codes per patient and inpatient surgery would result in annual costs of either 1.4 billion EUR (10% increase) or 1.7 billion EUR (10% decrease). The diverging effect compared to an alteration of POCD incidences stems from the distribution of cases in respective age-groups and the fact, that OPS numbers are divided by this factor.
Discussion
A strength of the present analysis lies in its transparency and the utilization of publicly available data, together with recently established POCD incidence rates in Germany and reasonable assumptions. However, the results of the sensitivity analyses vary – in one case even significantly – indicating the degree of uncertainty of assumptions and inputs that were used.
The reported results of our model-based calculations depend on the applied incidence rates of POCD. Therefore, significant effort was made to obtain reliable estimates of age-specific incidence rates across surgery types from the BioCog study. The fact that we applied incidence rates across surgery types introduces uncertainty of the modelled results, because the data base used for estimating POCD patient numbers (OPS 2019 statistic) reflects slightly different shares of operations with regards to the surgery site compared to the BioCog sample from which POCD incidence was inferred. This is important to note, since most publications on POCD incidences focus on specific types of surgeries and report highly heterogeneous numbers 19, 20, 21, 22.
For the base case, we used a controlled definition of POCD based on a reliable change index as suggested by Rasmussen et al., 2001. This definition results in lower POCD incidence compared to more liberal definitions. To give an example: A recent publication on recommendations for the nomenclature of cognitive change associated with anesthesia and surgery suggests to report postoperative cognitive dysfunction more in line with the DSM-5 diagnosis of Neurocognitive disorder (mild/major NCD) and use the former ‘POCD’ as a specifier to indicate its coincidence with surgery for up to one year postoperatively 10. Mild NCD with a more liberal cut-off of 1-2 standard deviations would result in higher POCD case numbers and subsequently in higher costs to long-term care insurance.
It should also be noted, that the BioCog sample – from which we drew the applied POCD incidence rates – represents a younger cohort than the chapter 5 OPS utilization sample that was used to estimate the number of patients undergoing surgery in Germany in 2019. Since POCD-incidence is highly dependent on patient age, the model rather underestimates the true number of POCD cases.
In addition to that, POCD incidence rates obtained from the BioCog study might be influenced by the trial`s drop-out rate: POCD data at 3 months is available for 641 out of 933 patients. Low follow-up rates (69% for cognitive testing in BioCog) are common in POCD trials, e.g. the ISPOCD study reported a similar low POCD prevalence (10%) with a comparable follow-up rate of 78% 4. This comparably high number of patients lost-to-follow-up was anticipated at the outset of the BioCog study and detailed analyses of patients lost to follow-up were performed. In our context, an increased drop-out rate is considered to mask actual POCD rates, rendering our applied POCD rates as conservative approximations of the reality.
A limitation of the present study involves the fact, that cost consequences of transitions from long-term care intensity 0 to 2 (Pflegegrad 2) were modelled. We investigate the effect of exemplary alternative transition distributions in corresponding sensitivity analyses, but in fact there are many other possible transitions (e.g. from care intensity 1 to 4, from 2 to 5 etc. and even switches between long-term care types) that were not modelled but each triggering different cost consequences depending on the shares of patients in each segment of inpatient or outpatient long-term care. These aspects were not modelled, because there is a lack of evidence that could serve as a base for reasonable assumptions and guide our calculations. The fact that we only modelled one possible switch from long-term care intensity 0 to 2 – but in fact there many more – indicates that the long-term care costs attributable to POCD are likely to be even higher than we report. Future analyses should focus on determining the exact amounts and shares of patients transitioning from one care segment to another.
In light of our conservatively chosen incidence rates, the analyzed chapter 5 OPS utilization numbers as a representative base for POCD case number calculations, actually reflect performed operations and not cases or patients. We sought to control for that aspect by excluding supplemental OPS-codes not reflecting separate surgeries, and by dividing the resulting number of chapter 5 OPS-codes by the average number of chapter 5 OPS-codes per patient observed in a sub-sample of the BioCog study. Dividing chapter 5 OPS utilization by the average number of chapter 5 codes per patient introduces additional uncertainty, because it is unclear whether this factor is the same in all German patients undergoing surgery captured in the OPS data. Therefore, we investigated the effect of varying average numbers of chapter 5 OPS-codes per patient in corresponding sensitivity analyses.
Currently, a large multicenter clinical trial is recruiting patients in Germany who will undergo a multimodal and multidisciplinary intervention after surgery with the aim to reduce POD rates by at least 40% and to reduce POCD rates by at least 20% 23. Assuming a 20% decrease in POCD rates within the framework of the presented model, would translate into a reduction of POCD related costs of around 312mio EUR in the long-term care insurance according to the base case model. Additional savings in the health care sector are likely due to reduced expenses for diagnostic procedures associated with the staging of POCD patients for different long-term care intensities. Given the assumed effectiveness of the multidisciplinary intervention, a prospective diagnostic tool that could reliably detect POCD before surgery, would have a significant value from a health- and socio-economic perspective. The precise value of such a tool in terms of EUR would depend on the treatment consequence of a detected suspected POCD case and associated costs of these consequences. Test-performance in terms of sensitivity and specificity as well as associated costs of applying the test on a patient are additional determinants of the health- and socio-economic value. In the present context, treatment consequences are limited to:
cancellation of surgery, if justifiable from a medical perspective
suspension of surgery, if improvement of test-outcome at a later point of time is likely
modification of treatment path, e.g. application of multimodal and multidisciplinary interventions, modified anesthesia or other measures
These consequences would need to be precisely investigated with regards to costs and effectiveness for an exact estimation of the health- and socio-economic value of a prognostic POCD detection tool.
Conclusion
A first and transparent model-based analysis of POCD associated costs in the German social long-term care insurance could be developed and evaluated. The analysis reveals significant long-term care costs associated with POCD of approximately 1.6 billion EUR annually. Several assumptions and features of the cost-model ensure conservative estimates of the results, suggesting that the actual financial burden of POCD to the long-term care insurance is even higher. For a precise determination of POCD related long-term care costs more research needs to be devoted to aspects surrounding the consequences of POCD with respect to the long-term care insurance. These aspects include age-specific POCD incidence rates, numbers and shares of patients transitioning from no dependency on long-term care to other segments of long-term care intensity and type. Additional studies should further reveal whether shares of patients are altered between different long-term care schemes due to the development of POCD, and consider effects on expenses for technical long-term care aids (Pflegehilfsmittel), support for improvements in home environments (Wohnumfeld-Verbesserungsmaßnahmen), transfer payments to pension funds, unemployment insurance, statutory health insurances and other legal financial support of the long-term care insurance.
Authors' Contributions
All authors contributed to the study conception and design. The first draft of the manuscript was written by Simon A. Weber and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Affiliations
Simon A. Weber1, Malte Pietzsch1, Claudia Spies2, Fatima Yürek2, Daniel Hadzidiakos2, Friedrich Borchers2, Florian Lammers-Lietz2, Sophie K. Piper3,5, Jochen Kruppa3,5, Georg Winterer2,4, on behalf of the BioCog consortium
Cellogic GmbH, Niedstrasse 21, 12159 Berlin
Department of Anesthesiology and Intensive Care Medicine (CCM, CVK), Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Augustenburger Platz 1, 13353 Berlin, Germany.
Institute of Biometry and Clinical Epidemiology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Charitéplatz 1, 10117 Berlin, Germany
Pharmaimage Biomarker Solutions GmbH, Biotech Park Berlin-Buch, Robert-Rössle-Str. 10, 13125 Berlin, Germany
Berlin Institute of Health (BIH), Anna-Louisa-Karsch-Strasse 2, 10178 Berlin, Germany
References
- 2.Arentz C. (2019) Szenarien zur zukünftigen Finanzentwicklung der Sozialen Pflegeversicherung.Wissenschaftliches Institut der PKV.
- 3.Gold S, Forryan S. (2019) Postoperative cognitive decline: a current problem with a difficult future.Trends in Anaesthesia and Critical Care. 24, 49-58.
- 4.Moller J, Cluitmans P, Rasmussen L, Houx P, Rasmussen H. (1998) Long-term postoperative cognitive dysfunction in the elderly:. ISPOCD1 study.The Lancet 351(9106), 857-861.
- 5.Rudolph J, E R Marcantonio, D J Culley, Silverstein J, Rasmussen L. (2008) Delirium is associated with early postoperative cognitive dysfunction.Anaesthesia. 63(9), 941-947.
- 8.T G Fong, Davis D, M E Growdon, Albuquerque A, S K Inouye. (2015) The interface between delirium and dementia in elderly adults.Lancet. , Neurol 14(8), 823-832.
- 9.T N Robinson, C D Raeburn, Z V Tran, E M Angles, L A Brenner. (2009) Postoperative delirium in the elderly: risk factors and outcomes.Annals of surgery. 249(1), 173-178.
- 10.Evered L, Silbert B, D S Knopman, D A Scott, S T DeKosky. (2018) Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018.Br. 121(5), 1005-1012.
- 11.Winterer G, Androsova G, Bender O, Boraschi D, Borchers F. (2018) Personalized risk prediction of postoperative cognitive impairment - rationale for the EU-funded BioCog project.Eur Psychiatry. 50, 34-39.
- 12.D L Leslie, E R Marcantonio, Zhang Y, Leo-Summers L, S K Inouye. (2008) One-year health care costs associated with delirium in the elderly population.Arch Intern Med. 168(1), 27-32.
- 13.Brown C H t, Laflam A, Max L, Lymar D, K J Neufeld. (2016) . The Impact of Delirium After Cardiac Surgical Procedures on Postoperative Resource Use.Ann Thorac Surg 101(5), 1663-9.
- 14.Weinrebe W, Johannsdottir E, Karaman M, Fusgen I. (2016) What does delirium cost? An economic evaluation of hyperactive delirium.Z. , Gerontol Geriatr 49(1), 52-8.
- 15.D L Leslie, S K Inouye. (2011) The importance of delirium: economic and societal costs.J. , Am Geriatr Soc 59, 241-3.
- 16.Bundesamt Statistisches, D. (2020) Fallpauschalenbezogene Krankenhausstatistik (DRG-Statistik). Operationen und Prozeduren der vollstationären Patientinnen und Patienten bis zum kodierbaren Endpunkt .
- 17.Rasmussen L, Larsen K, Houx P, Skovgaard L, Hanning C. (2001) The assessment of postoperative cognitive function.Acta Anaesthesiologica Scandinavica. 45(3), 275-289.
- 18.Bundesamt Statistisches, D. (2020) Pflegestatistik - Pflege im Rahmen der Pflegeversicherung. , Deutschlandergebnisse
- 19.M J Needham, C E Webb, D C Bryden. (2017) Postoperative cognitive dysfunction and dementia: what we need to know and do.Br. 119, 115-125.
- 20.Holmgaard F, A G Vedel, L S Rasmussen, O B Paulson, J C Nilsson. (2019) The association between postoperative cognitive dysfunction and cerebral oximetry during cardiac surgery: a secondary analysis of a randomised trial.Br. , J Anaesth 123(2), 196-205.
- 21.W X Li, R Y Luo, Chen C, Li X, J S Ao. (2019) Effects of propofol, dexmedetomidine, and midazolam on postoperative cognitive dysfunction in elderly patients: a randomized controlled preliminary trial.Chin Med. 132(4), 437-445.
- 22.Tzimas P, Samara E, Petrou A, Korompilias A, Chalkias A. (2018) The influence of anesthetic techniques on postoperative cognitive function in elderly patients undergoing hip fracture surgery: General vs spinal anesthesia.Injury. 49(12), 2221-2226.
- 23.Sanchez A, Thomas C, Deeken F, Wagner S, Kloppel S. (2019) Patient safety, cost-effectiveness, and quality of life: reduction of delirium risk and postoperative cognitive dysfunction after elective procedures in older adults-study protocol for a stepped-wedge cluster randomized trial. , (PAWEL Study).Trials 20(1), 71.
Cited by (10)
This article has been cited by 10 scholarly works according to:
Citing Articles:
Frontiers in Endocrinology (2026) Crossref
European Journal of Anaesthesiology (2026) Crossref
Springer eBooks (2025) OpenAlex
K. Granger, Claudia D. Spies, Sheryl Caswell, D. Hadzidiakos, Saya Speidel et al. - JAR life (2025) Semantic Scholar OpenAlex Crossref
H. Varpaei, Kousha Farhadi, Mostafa Mohammadi, Alireza Khafaee Pour Khamseh, Tahereh Mokhtari - Aging Clinical and Experimental Research (2024) Semantic Scholar OpenAlex Crossref
Marinus Fislage, I. Feinkohl, F. Borchers, T. Pischon, C. Spies et al. - Scientific Reports (2023) Semantic Scholar OpenAlex Crossref
Research Square (Research Square) (2023) OpenAlex
Research Square (Research Square) (2022) OpenAlex