Abstract
Objectives:
The present study investigated biopsychosocial predictors (HbA1c, self-efficacy, and social support) of self-management and health-related quality of life among patients with type 2 diabetes.
Methods:
160 adults referred to the Iranian Diabetes Society participated in this study. Participants completed General Self-Efficacy Scale, Perceived Social Support, Diabetic Self-care Behaviors scale, and D-39 (diabetics’ quality of life).
Results:
Data were analyzed with SPSS-19 and Lisrel 8.8, utilizing statistical path analysis. Results revealed significant positive correlations between self-efficacy and social support subscales, self-care and health-related quality of life. Also, HbA1c had not correlation with HRQOL. The final path model fitted well and showed that direct self-care paths with (β = 0.24) and indirect social support with (β = 0.32) had the most effects on health-related quality of life.
Conclusions:
The results confirmed the theoretical model and scientific evidence for providing psychological solution to promote quality of life in patients with type 2 Diabetes.
Author Contributions
Academic Editor: Dr. Kamran Mahmood Ahmed Aziz, Ministry of Health, Saudi Arabia
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2017 Saeideh Bazzazian
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction:
Type 2 diabetes as a metabolic disorder, is characterized by a regular rising in cellular resistance to the effects of insulin and, subsequently reducing the insulin production 1. The chronic increase of blood glucose results in a broad range of macrovascular disease (such as strokes and myocardial infraction), microvascular disease (nephropathy and retinopathy), and neuropathy 2. To prevent of complication, durable glycemic control and self-care activities has been recommended 3. A diagnosis of type 2 diabetes usually happens in middle age; while an average age of diagnosis is around 45 years 1, 4.
Diabetes type 2 as an increasingly prevalent condition, have major impact on mortality, quality of life, and health care costs 5 and major challenges in economically developing and developed countries. According to the report of international diabetes federation, about 382 million people in the world have diabetes, and this number is expected to increase to about 600 million by 2035 6. Also, the results of Lipid and Diabetes Study in Iran has indicated that each year, 4 % population of Tehran change from healthy mood to pre-diabetes mood, and 1% reach to diabetes 7.
Concerning the prevalence and importance of diabetes management, most studies reveal a negative effect of diabetes on Health Related Quality of Life (HRQOL) 8, 9, 10, 11. HRQOL is defined as the “physical, psychological and social dimensions of health, seen as distinctive domain that is shaped by a person’s experience, belief, expectation and perception” 12. HRQoL is also generally understood to hold illness or treatment as well as subjective description of a patient’s HRQoL 13, 14.
Also, Self-management has become increasingly important in the treatment of type 2 diabetes. From a biomedical perspective, self-management is defined as a patient’s ability to manage the symptoms, treatment, physical consequences, and lifestyle changes important in living with a chronic disease. Diabetes self-management consists of attending the areas of nutritional management, physical activity, blood glucose checking, and medication use 15.
HRQOL have been shown to be associated with some bio-psycho-social factors however little is known about how these bio-psycho-social variables interact and how they influence self-care behaviors, separately and combined. Increased knowledge may discard light on identifying targets for both diagnosis and treatment. So, this study was aimed to investigate the role of HbA1c (as a biological dimension), self-efficacy (as a psychological dimension), and social support (as a social dimension) in patients’ self-care and HRQOL.
Evidently, one of the methods of assessing the progress of diabetes at the time of diagnosing and achieving the glycemic control after diagnosis is the degree of hyperglycemia. The most objective measure of hyperglycemia is the glycated hemoglobin (HbA1C) value. The higher HbA1C value at diagnosis indicates the delayed disease detection, while further elevation following the diagnosis indicates poor early management of the disease. Prior studies revealed that HbA1C has been associated with certain psychological characters which may affect disease diagnosis and management 16, 17.
Self-efficacy, as a term which is derived from the social cognitive theory, refers to “belief that person has capability to organize and execute the course of action required gaining given levels of achievements” 18. Self-efficacy is described as one’s self-reliance to achieve a specific goal, where diabetes self-efficacy is defined as beliefs about personal capacity to hold diabetic self-care skills 19.
Perceived social support includes emotional support or interactions with social network, family members, friends, or peers 12. Studies have shown positive associations between perceived social support and adherence to disease managements 20. The more perceived social support, the better chronic disease outcomes, that includes glycemic control among those with diabetes, and hospitalization risk and functional status among those with cardiac disease and rheumatoid arthritis 21, 22, 23.
Based on the above mentioned literature review, this research has examined the theoretical path model for effects of self-efficacy, social support, and HbA1c on self-care and health related HRQOL Figure 1
Figure 1. Hypothetical model for prediction of Quality of life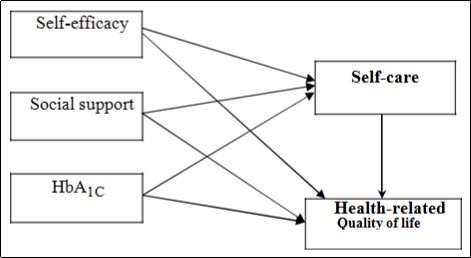
Methods:
Participants
All members of Iranian Diabetes Society in Tehran with type 2 Diabetes approached to participate in the study. Inclusion criteria were: married; age 30-65 (because of the prevalence of type 2 Diabetes in this range); middle socioeconomic classes; diagnosis of diabetes of at least 1 year duration; and insulin administration. Exclusion criteria were: second chronic illness (but comorbidities such as cardiovascular disease are allowed); pregnancy-related diabetes; moderate or severe learning disabilities (due to use self-report questionnaires); other psychological disorders prior to diabetes (according to medical records). 200 patients identified from medical records as fulfilling the eligibility criteria and 176 patients agreed to participate. 16 cases excluded because they had not fulfilled at least 60% of items of the scales. Finally, the number of participants was 160. The demographic and medical characteristics of patients were presented in Table 1.
Procedure
All eligible patients were called and explained purpose of the research and were told that they could withdraw at any time from research. They were invited to go to Iranian Diabetes Society. They completed consent written form, demographic (gender, education, age) and research questionnaires. It took about 30 minutes to fill questionnaires. All patients have the opportunity to take medical or psychological counseling after filing questionnaires. The researchers obtained permission to collect data from the ethical committee of the Iranian Diabetes Society.
Instruments
Demographic and Biomedical Data:
Demographic data were obtained by patient self-report.HbA1c level (the most recent value within the last 4 months), chronic disease co-morbidities (e.g. congestive heart failure, chronic obstructive pulmonary disease, or arthritis) and diabetes-related complications (nephropathy, retinopathy, neuropathy) were obtained from the patients self-report and medical records.
HbA1c is an estimate of blood glucose control over the past 3 months. The closest blood test to the date of questionnaire completion was chosen for each patient. It was determined on a venous blood sample (HBLC, ref. 3.9-6.3).
General self-efficacy scale is a 10-item questionnaire. Each item is scored on a 4-point scaleranging from 1 (never) to 4 (always). So, higher scores indicate a higher level of self-efficacy. Adequate psychometric properties of the scale in sample of students and adult populations have been reported 24. Internal consistency reliability for this study was 0.80.
Multi-dimensional scale of perceived social support have made by Zimmet et al. It has 15items and made up of three subscales: family, friends and other significant. Each item is scored on a 7-point scale which ranged from 1 (strongly agree) to 7 (strongly disagree). Total Cronbach’s alpha internal consistency reliability coefficient and subscales had been reported from 0.85 to 0.91. 25. In this study, the internal consistencies were 0.94, 0.93, and 0.94 for significant, family, and friends’ subscales respectively.
Diabetic Self-care activities scale is developed to diagnose self-care behaviors by Toobert, et al.It has consisted of 12 items including self-care activities of diet, exercise, blood glucose testing, foot-care, and smoking. The measure asked the participant the number of days per week the participant had practiced self-care activities. Toobert et al. reported a relatively stable test-retest correlation and internal consistency. Cronbach’s Alpha of this study was found to be 0.85. Test-retest coefficient with 5 week interval for subscales have been reported from 0.47 to 0.70, and total Cronbach’s alpha internal consistency reliability coefficient and subscales from 0.72 to 0.87 in Iran 26.
Quality of Life Scale of patients with diabetes (D-39) is 36 items scale which assess 5dimension of quality of life in diabetic patients (diabetes control, energy and mobility, social burden, anxiety and worry, and sexual functioning). Adequate psychometric properties of the English 27, 28 and Farsi version of the scale in 460 type I and 2 diabetic patients have been reported 29. In this research, total scores of dimensions were used.
Results:
Structural equation modeling was performed to test the hypothesized theoretical model. Statistical analyses were carried out using SPSS 19.0 software and Lisrel 8.50 for Windows.
The total subjects in this study were 160 patients: 92 (57.50%) female and 68 (42.50%) male (34.6%), with a mean age of 22.40 (3.49) years. Their educational levels ranged from high school diploma (n = 128; 80%) to undergraduate (n = 25; 15.6%), and graduate (n = 7; 4.4%). In diabetes complications, 27 (16.9%) patients had retinopathy, 3 (1.9%) nephropathy, 29 (18.1) neuropathy, 13 (8.1%) heart disease, 2 (1.3%) others, and 86 (53.8%) non-complications. The mean HbA1c level was 7.52 ± 2.62 and the average duration (months) of diabetes was 106.72 in male and 107.26 in female patients. 43(14.3%) patients had Hyperglycemia in last six month, the blood lipid of 47 (29.4%) patients was above normal range, and 47 (29.4%) showed Hypertension. Also weight, height and age of subjects were showed in Table 1. There were not significant differences between males and females in variables Table 1.
In Pearson correlation analysis, positive correlation was found between self-efficacy, and social support and with self-care (P<0.01). The HbA1c scores showed a negative correlation with self-care (P <0.01). Also, there was a positive correlation between self-efficacy, and social support with HRQOL (P<0.01). However, no significant relationship was observed between HbA1c and HRQOL Table 2.
Model fit the data very well (Chi square 0.43, P = 0.50, CFI = 0.90, AGFI = 0.86, RMSEA = 0.055). So, the results indicated desirability, high fitness, and rationality of the parameter relationships based on the conceptual model. Accordingly, the fitted model had no significant difference with the conceptual model Table 3.
Table 1. Patients characteristics (n = 160)| variables | N (%) | t | P |
|---|---|---|---|
| Gender | |||
| Female | 92 (57.50) | ||
| Male | 68 (42.50) | ||
| Age (years) mean (SD); range | 46.40 (3.49); 30-65 | ||
| Education | |||
| High school Diploma | 128 (80) | ||
| Undergraduate student | 25 (15.6) | ||
| Graduate | 7 (4.4) | ||
| Diabetes complication | |||
| Retinopathy | 27(16.9) | ||
| Nephropathy | 3(1.9) | ||
| Neuropathy | 29 (18.1) | ||
| Heart disease | 13(8.1) | ||
| Others | 2 (1.3) | ||
| Non-complication | 86(53.8) | ||
| Hyperglycemia in last six months, mean (SD) | 43(14.3) | ||
| Blood lipid, mean (SD) | 74(46.3) | ||
| Hypertension, mean (SD) | 47(29.4) | ||
| Age (male, female), mean (SD) | 50.77(10.31), 50.55 (10.41) | ||
| Weight (male, female), mean (SD), | 79.19 (16.90), 73.03(13.01) | ||
| Hight (male, female), mean (SD) | 167.73(9.02), 160.47(8.37) | ||
| Diabetes duration (month), (male, female) mean (SD) | 106.72(95.04), 107.26(98.38) | ||
| HbA1c (male, female) mean (SD) | 7.7 (2.25), 7.6(1.98) | 0.244 | 0.80 |
| Self-efficacy (male, female) mean (SD) | 30.94 (6.16), 28.67 (5.62) | 1.57 | 0.12 |
| Social support (male, female) mean (SD) | 57.07 (19.31), 52.35 (19.88) | 1.50 | 0.13 |
| Self-care (male, female) mean (SD) | 42.61 (12.43), 43.08 (13.41) | 0.226 | 0.82 |
| Variables | M (SD) | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|---|
| HbA1c | 7.70 (2.02) | - | ||||
| Self-efficacy | 29.89 (5.54) | -.148 | - | |||
| Social support | 54.36 (19.72) | -.096 | .349** | - | ||
| Self-care | 42.88 (12.97) | -.300** | .367** | .425** | - | |
| HRQOL | 45.47 (1.51) | -.032 | .249** | .337** | .346** | - |
| indices | X 2 | df | P | CFI | GFI | AGFI | RMSEA |
|---|---|---|---|---|---|---|---|
| Initial model | 0.43 | 2 | 0.50 | 0.98 | 0.90 | 0.86 | 0.055 |
According to the path diagram, among direct paths, path of self-efficacy (β = 0.16), social support (β = 0.18), and self-care (β = 0.24) had significant effect on HRQOL. Also, self-efficacy (β = 0.21) and social support (β = 0.32) had significant indirect effect on HRQOL. While HbA1c had not significant direct effect on HRQOL, it had significant indirect effect through self-care on HRQOL (β = 0.23) Table 4Figure 2.
Table 4. Path coefficients for self-efficacy, social support, HbA1c, self-care, HRQOL| Predictor | Effects | Model Coefficients | T value | ||
|---|---|---|---|---|---|
| Variables | Direct | Indirect | Total | ||
| Self-efficacy | 0.161* | 0.219* | 0.380 | 0.25 | 1.925 |
| Social support | 0.183* | 0.328** | 0.411 | 0.27 | 2.235 |
| HbA1c | -0.073 | 0.236** | 0.303 | 0.11 | 0.957 |
| Self-care | 0.241** | 0.241 | 0.34 | 2.813 | |
Figure 2. Path diagram based on direct and indirect effects of variables 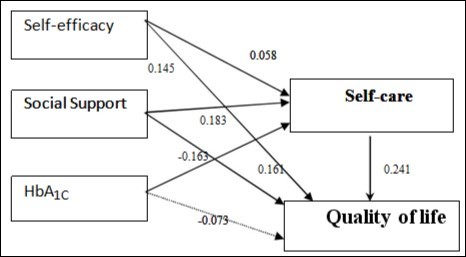
Discussion:
The aim of current study was to examine the theoretical path model of HRQOL on the base of bio-psycho-social variables (HbA1c, self-efficacy, and social support). The results revealed the direct effect of self-efficacy and social support and indirect effect of self-efficacy, social support and HbA1c though self-care on HRQOL in type 2 diabetic patients. In other words, self-care mediated the relationship between bio-psycho-social variables and HRQOL. In literature there was not any study which considers biopsychosocial factors together. But, the results were consistent with other studies that have investigated the relationship between mentioned variables separately 30, 31, 32, 33.
According to the results, HbA1c had not direct effect on HRQOL. HbA1c as a biologic factor is the most important index in diabetics. Some studies 1 suppose that HbA1c was crucial in type 1 diabetes because of importance of controlling daily blood glucose but not in type 2 diabetes 17, 34.
Self-efficacy had direct and indirect effect on HRQOL. Previous studies 35, 18, showed that self-efficacy has a significant relation with diabetic patients’ mental health among older adults regardless of their racial and ethnic backgrounds.
Self-efficacy in the meaning of one’s judgment about its abilities for performing actions, could enable person to adopt health-promoting behaviors and to hold out health- damaging behaviors. People tend to involve in tasks which they feel ability to perform them and to avoid them when they feel that they go above their capacities. Also, self-efficacy influences how people motivate themselves in the tasks that they carry out. People with a strong sense of self-efficacy consider situations as challenges to be overcome. In addition, self-efficacy beliefs influence emotional states; people with higher self-efficacy are likely to have lower stress and depression than others 22. Therefore, self-efficacy has appeared as an important factor in diabetes self-management behaviors and quality of life 32. In other words, diabetic patients’ well-being and quality of life can be encompassed by promoting diabetes self-efficacy.
Patients with high self-efficacy will be more persistent in coping with of problems 36; that is, patients may feel capability to manage diabetes and handle their regimens and have low distress through diabetes self-efficacy. In other hand, higher self-efficacy improves problem-solving. So, they could learn adequate self-care procedure to manage diabetes.
In consistency of other studies 37, 38, the results of this study revealed direct and indirect effects of social support on HRQOL.
Social support as an important resource of adjustment with chronic diseases, have effective role in outcomes of functional and psychological adaptation with chronic conditions. There were increasing evidence that social support is a determinant variable in individual differences in reaction to the stress and illness management 39. The perception that one has reliable social resources to rely on in times of stress or change that could be important to successful self-management behavior. Moreover, social support (e.g., having regular contact with or encouragement from family and friends) is relatively low cost and has many other potential benefits to multiple aspects of chronic illness care (such as reduction of co-morbid depressive symptoms) 37.
It seems that some friends or family members may pass more deserving message to patients about how to practice self-care, or provide better emotional and informational support to patients and in turn increase patient’s diabetes self-efficacy 40. In Iran as a country with higher level of family affiliation, even in elderly, family ties are very strong. So, this finding was predictable.
Conclusions:
Given the previously reported crucial effect of self-efficacy and social support on the diabetic management and quality of life of patients 41, 42, 43, increasing the level of self-efficacy and social support would be helpful for patients with diabetes not only to manage diabetes but also to improve their overall well-being and HRQOL. Also, researches showed that the risk of developing many of disease complications can be reduced if people with type 2 diabetes are provided the knowledge and skills to self-manage their condition. This involves creating considerable behavioral and lifestyle changes 44. Thus, researchers, health psychologists, and clinicians should pay more attention to developing intervention strategies focusing on increasing diabetic self-efficacy and social support especially in family affiliated communities such as Iran. Also it was recommended that biopsychosocial factors would be considered in management programs. Future researches might be considered to interactional effects of biopsychosocial factors as well.
Several limitations, however, need to be considered. First, self-efficacy and social support were assessed by self-report scales that may not have adequately reflected the complexities of these constructs. Second, only the general self-efficacy and social support was used and these scales were not specifically for diabetic patients. Last, there were some inclusion criteria that restrict the findings generalization. Further researches in other patients group with other inclusion criteria can support our conclusion.
Acknowledgment
The author thanks A. Rajab, the head of Iranian Diabetes Society and his colleagues, and all members of Iranian diabetes Society for their cooperation in this study as patients. Also, the author thanks the head of Islamic Azad University, Abhar Branch, for the financial support.
Funding:
This study was funded by Islamic Azad university, Abhar Branch (Grant number 02-11-5-12353/ 2011/7/6).
Ethical Approval:
For this type of study formal consent is not required. However permission tocollect data was obtained from the ethical committee of the Iranian Diabetes Society.