Abstract
This case report describes the treatment of a dento-alveolar protrusion with anterior open bite. The 21-year old patient had a convex profile , class I dental malocclusion , anterior open bite of 4 mm and presented tongue thrust. The treatment plan was to insert two mini-implants for premolar intrusion along with the straight –wire fixed appliances. Tongue therapy was performed by myofunctional exercises. Using the absolute anchorage we were able to achieve our goals in a predictable manner without the use of orthognathic surgery or patient compliance . After the tongue thrust habit was removed we are confident that this is a stable result .
Author Contributions
Academic Editor: Vinayak Raghunathan, Assistant Professor
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Camelia Szuhanek, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Orthodontic mini-implants are now widely used to provide absolute anchorage because of their versatility , minimal invasiveness and low cost .1
Difficult orthodontic cases , like molar intrusion, molar uprighting , anterior open bite treatment with molar intrusion, anterior deep bite treatment with incisal intrusion, leveling of transverse tipping of the occlusal plane, asymmetric expansion, space closure are corrected without the need of extraction, orthognathic surgery or patient compliance.3
New mechanics based on absolute anchorage have expanded the variety of ortho-mecanoterapy .4 The most important change is that it becomes possible to intrude posterior teeth bilaterally with mechanotherapy alone.5
Diagnosis and Etiology
The patient, a 21-year old woman , had a convex profile , class I dental malocclusion ,anterior open bite of 4 mm . She was a mouth breather and presented tongue thrust. Her chief complain was the anterior open bite .(Figure 1)
Figure 1. Pretreatment intraoral photography
The cephalometric analysis indicated that she had a skeletal class II profile ,proclination of the maxillary central incisor ,high mandibular plane angle that contributed to the class II skeletal relationship and increased lower facial height.
Figure 2. Pretreatment cephalometric film
The panoramic radiograph showed bilateral mandibular third molars. The level of alveolar bone crest was within the normal range. (Figure 3)
Figure 3. Pretreatment panoramic X-ray 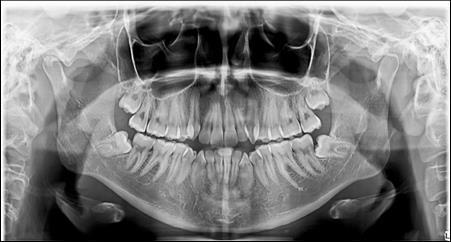
Figure 4. Intraoral photography at the start of the treatment.
Theories to explain the cause of anterior open bite: digital habits , airway obstruction, tongue posture, unfavourable growth, tongue trust .2
The patient presented tongue thrust and mouth breathing. She was reffered for myofunctional exercises for tongue thrusting before orthodontic mechanics began.
Treatment Objectives
·To maintain class I molar and canine relationship with ideal overjet and overbite while maintaining facial esthetics
·Avoid extrusion of the molars and clockwise rotation of the mandible during treatment
·Close the anterior open bite
Treatment Options
Anterior open-bite treatment alternative:
1.Extrusion or eruption of anterior teeth. Several authors reported the side- effects of this orthodontic movement: root resorption, less stability and esthetics 7
2.Intrusion of the lateral teeth- Studies reported different methods to intrude the posterior teeth ( posterior bite blocks, high- pull headgear , mini-implants )8
3. Orthognathic surgical impaction of the posterior maxilla to allow the mandible to autorotate counter clockwise and close the bite .
4. Extraction of the first premolars in order to close the bite and reduce the overjet.
5. Surgical removal of all third molars was indicated before appliance removal.
The patient refused orthognathic surgery and premolar extractions and elected the less invasive orthodontic treatment .
After obtaining the informed consent the orthodontic treatment began and 0,22 Roth straight-wire fixed appliances were bonded. After leveling and aligning, during upper arch expansion, we took impressions and made intermediate study models. We noticed that palatal cusps of the upper premolars could not be intruded by classic mechanics. We decided to intrude first and second bicuspids to resolve the open bite. Skeletal anchorage was indicated and two orthodontic mini-implants were inserted on the palatal side between the premolars.
Procedure to Insert the Mini-Implants
Anesthesia of the implant site. Root parallelism and position was checked on the panoramic x-ray. The implant site was marked with a periodontal probe . The screw had 1,6 mm diameter and 8 mm length. Contra-angle screw driver and the self-tapping method was used.
Anatomic Considerations
In the palatal area the soft tissue is thicker than in other areas12 . It is important to measure the soft tissue thickness to determine the ideal length of the mini-implant .
Complications
Treatment
The optimal force for intrusion reported by several authors are : 20 g of force for the anterior teeth- Burstone9, Gianelly and Goldman 15-50 g force10 .For the molar intrusion, the initial force recommended by Umemori et al is 500 g 11, Melson and Fiorelly used 50 g buccolingualy to intrude maxillary molars.13. Reitan and Rygh 6 reported that intrusion is more stable than extrusion
In this case the implants were loaded after one week with a 100-150 force using an elastic chain.
The intrusion rate obtained was 0,5-1 mm per month without root resorbtion or vitality problems.
Tongue therapy was performed.
Before the finishing stage, a panoramic x-ray was taken. The third molars were removed .(Figure 6)
Figure 5. Intraoral photography after the mini-implant activation
Figure 6. Panoramic X-ray before the removal of the third molars.
Figure 7. Clinical situation after intrusion with orthodontic implants.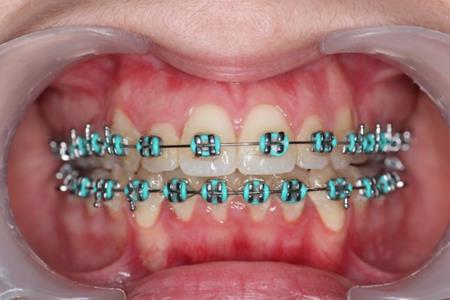
Results
After treatment the patient had a normal overbite and overjet and a stable occlusion, a class I canine and molar relationship.
Conclusion
Open bites can be closed without orthognathic surgery by using mini-implants as skeletal anchorage to intrude posterior teeth.
Good stability is expected with the intrusion of the lateral teeth and no extrusion of the anterior .