
Temporalis Fascia Lateral or Medial Side Up In Underlay Tympanoplasty Type – I Does It Makes A Difference?
Abstract
Objectives:
The study was aimed to find out which of the two techniques, medial or lateral side of the temporalis fascia graft was better in underlay method for correcting the perforations of the tympanic membrane keeping all other factors constant.
Methods:
We designed a prospective randomized study from Jan 2010 to Jan 2013 at Buraidah Central Hospital, Al Qassim, Saudi Arabia. Eighty patients having dry central; moderate, large and subtotal perforations of the tympanic membrane were subjected for tympanoplasty type –I by underlay technique. In 41 patients the temporalis fascia graft was placed with medial (rough) side up (Technique-I) and 39 patients the graft was placed with the lateral (smooth) side up (Technique-II).
Results:
The graft take up rate was 95.1% in technique-I and 87.2% in technique -II. Failure rate was 4.9% in technique – I and 12.8% in technique – II.
Conclusion:
Technique – I was judge to be giving better result because:
1.Rough surface of the medial side of the graft after moistening enhances wetting, increases the critical surface tension and broadens the contact surface.
2.The friction due to rough surface resists displacement forces between the graft and remains of the tympanic membrane.
3.Rough surface of the medial side of the temporalis fascia increases the adhesion power and increases the overlap between the two surfaces.
To the best of our knowledge this is the only such prospective study for this method.
Article Information
- Received
- Accepted
- Published
Academic Editor: Saqib Ahmed, University of California San Francisco, CA 94122
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 Latifi Asrar Ahmed, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Dr Latifi Asrar Ahmed, Chief of Ent Department, Buraidah, Central Hospital, P O Box: 2290, KFSH Housing Complex, Buraidah, -, Alqassim, KSA, Tel / —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction:
Fundamental principles of tympanoplasty were introduced by Wullstein and Zollner, since than different graft materials like; skin, vein, perichondrium and temporalis fascia were used for the closure of tympanic membrane perforation.1, 2 The use of Temporalis fascia graft was described for the repair of tympanic membrane by Ortegren in 1959.3 In 1961 Storrs described the successful use of autograft, temporalis fascia (TMF) in the underlay position for repair of tympanic membrane perforation.4 Since then use of autologous temporalis fascia graft for tympanoplasty has increased in popularity.
It was also apparent that the viability of the graft is not a factor as it was merely acting as a scaffold for the mucous membrane and epithelium from the drum remnant to epithelialize.5 This is the process of repair of the tympanic membrane. In underlay technique graft should be well placed under the remnant of the tympanic membrane. It should be well supported medially in the middle ear.6, 7
Rough surface of the TMF after moistening plays a great role in support of the graft, as it increases the critical surface tension and elasticity between the graft and the undersurface of the tympanic membrane remnant.7, 8
None of the otological studies described in the literature indicate the graft should be placed with medial or lateral side up in using the TMF in the underlay tympanoplasty technique; despite the great deal that has been written about the use of TMF in tympanoplsty. In our study placing the medial side face up in the underlay technique has proven better than the lateral side up for proposed reasons in the paper.
Method:
The study was undertaken at Buraidah Central Hospital, Buraidah, K.S.A. This faculty serves as secondary referral centre for ENT patients. This was a prospective randomized study over a period of three years, 80 cases of the chronic suppurative otitis media (CSOM) having central, subtotal and large perforation in the pars tensa were selected randomly. All were in dry stage. Patients ranged in age from 15-55 years; most were aged between 20 to 35 years.
Cases with active ear disease, cholesteatoma, polyp in the external auditory canal, external otitis or with chronic systemic disease were excluded from the study.
Ears were dry for at least 3 – 4 weeks prior to the surgery.
Hearing test was done by Pure tone audiometry. Patients with conductive and mixed hearing loss were included in the study. Complete hematological investigations were carried out in all cases with X-ray chest. X-ray paranasal sinsuses and mastoid were done in suspicious cases only.
Forty one (41) cases were operated by underlay technique by placing the medial side of temporalis fascia graft facing the mucous membrane of tympanic membrane remnants (Technique I).
In thirty nine (39) cases the lateral side of TMF graft was placed facing to the mucus membrane of the tympanic membrane remnant (Technique II).
Technique I: Medial Side Up of TMF in the Under Technique
Procedure:
The perforation margins were freshened and the mucosal surface was made raw. Through a post aural approach, the tympanomeatal flap was elevated and the middle ear exposed. TMF was harvested from the same incision and the graft was dried after removing the fascia and muscle over it. The side which was attached to the temporalis muscle was the medial side and the side with fascia and shiny part was the lateral side of the graft, the state of middle ea was examined and filled with gelfoam, TMF graft was placed medial to the annulus tympanicus with the medial side towards the remnant of tympanic membrane and a mucosal overlap of 2mm all around the margins of tympanic memrane.
Tympanomeatal flap was replaced and gelfoam was kept in the external auditory canal. Fucidin ointment wick was kept in the external auditory canal for 10 days.
Technique II:Lateral Side Up of The TMF in Underlay Method
The same procedure was applied as above except that the lateral (shiny) part of the graft was placed facing up towards the remnant of tympanic membrane.
In the post operative period the fucidin ointment wick was removed after 10 days. The graft was inspected and external auditory canal toileting was done on frequent visits to the clinic. All cases were followed weekly for a month, by the operating surgeon. Minimum follow up was up to six months.
All the cases were regularly followed up to two weeks, four weeks, and six weeks, twelve weeks and six months up till one year by the first author who was mainly involved in the operation for all cases. Hearing assessment was done after twelve weeks and six months. Average gain in hearing of 10db was considered as having hearing improvement.
Results:
A total of eighty (80) cases were operated in both techniques. The patients’ age ranged from 15 – 55 yrs.
Total male were 33 (41.2%) and females were 47 (58.7%). (TABLE 1)
The criterion for success was the restoration of an intact tympanic membrane.
In Forty-one (41) patient the medial side of TMF was placed facing the mucosal surface of the tympanic membrane in underlay technique. 2 (4.8%) patient had middle ear infection and graft was rejected, success rate of graft take-up was 95.1% (39 cases).
In thirty nine patients the lateral side of the TMF graft was placed facing the mucosal surface of the tympanic membrane. Five cases (12.8%) had rejection of the graft and success rate was 87.2% in (34 cases).
The overall success rate of our study including both techniques was 91.2% and failure rate was 8.7%. (TABLE 2)
Two (2) of the cases had pseudomonas infection, three (3) did not keep follow-up appointments for removal of pack and two (2) cases had post operative upper respiratory tract infection leading to middle ear infection.
Healing time of graft was also more in technique II (six to eight weeks) than in technique I (four to six weeks). (TABLE 3)
Until six months of follow-up there has been no evidence of anterior blunting or lateralization of the graft in any of the successful cases.
TABLE 1. Sex Distribution in Technique I and Technique II with total number of cases in percentage in underlay Tympanoplasty – I.| No. of Cases | Technique I | Technique II | Total with % |
|---|---|---|---|
| M | 17 | 16 | 33 (41.2%) |
| F | 24 | 23 | 47 (58.7%) |
| Total | 41 (51.2%) | 39 (48.7%) | 80 |
| Results | N = 41 Technique I | N = 39 Technique II |
|---|---|---|
| Successful graft take up | 39 (95.1%) | 34 (87.2%) |
| Graft failure | 2 (4.9%) | 5 (12.8%) |
| Healing Time (In weeks) | Technique I (No. of cases) n = 41 | Technique II (No. of cases) n = 39 |
| 4 | 19 | 11 |
| 5 | 7 | 4 |
| 6 | 9 | 13 |
| 7 | 0 | 3 |
| 8 | 2 | 1 |
| 10 | 0 | 2 |
| 12 | 2 | 0 |
| no. of successful cases | 39 | 34 |
Discussions:
Autologus temporalis fascia was first described by Ortegren in 1959, and then by Herrman in 1960.3, 9 Storrs and Glasscock described the successful use of autologus temporalis fascia in the underlay position for closure of tympanic memrane perforation.4, 10
In the underlay technique, there are a number of factors responsible for holding the graft in place that results in a successful graft take up.7, 11
Among them are:
1.Perfectly dry ear or a ear which is not grossly infected.5
2.Adequate operative exposure.3, 12
3.Well prepared base for the graft by gelfoam in the middle ear.6
4.Insertion of the graft between handle of malleus and tympanic membrane remnant.13
5.Surface tension acting between the graft and under the surface of the tympanic membrane remnant.7
6.Adequate blood supply from the tympanomeatal flap or a vascular strip.5, 11, 14
Various studies have demonstrated that, viability of the graft is least important as it merely acts as a scaffold for mucous membrane and epithelium for the drum remnant to epithelialise.5, 15 For this reason the underlay technique, the graft should be well stuck or get attached to the mucous membrane of the tympanic membrane remnant.
This two years prospective study tried to compare the results of placing of medial side up and the lateral side up of the TMF in the underlay technique of tympanoplasty. Both techniques were tried in all sizes of perforation of the tympanic membrane, while keeping the other entire influencing factor constant. The ear was kept dry for at least 3 – 4 weeks before operations.
Our study seems to be first study to asses and compare the placement the lateral and medial side of the TMF toward the mucous membrane of the tymapanic membrane remnant.
The medial side of the TMF graft is attached to the temporalis muscle after harvesting the graft, the muscle fibres were scraped of the graft. This part of the graft is still rough as compared to the lateral side which is shiny and smooth on microscopic examination. (Figure-1) Before placing the graft it was moistened with saline. In forty one patient technique I was used and in thirty nine patient, technique II was applied.
Figure-1. Fig x40, HE: Shows skeletal muscle on lower left and fibrocollagenous tissue of fascia on upper right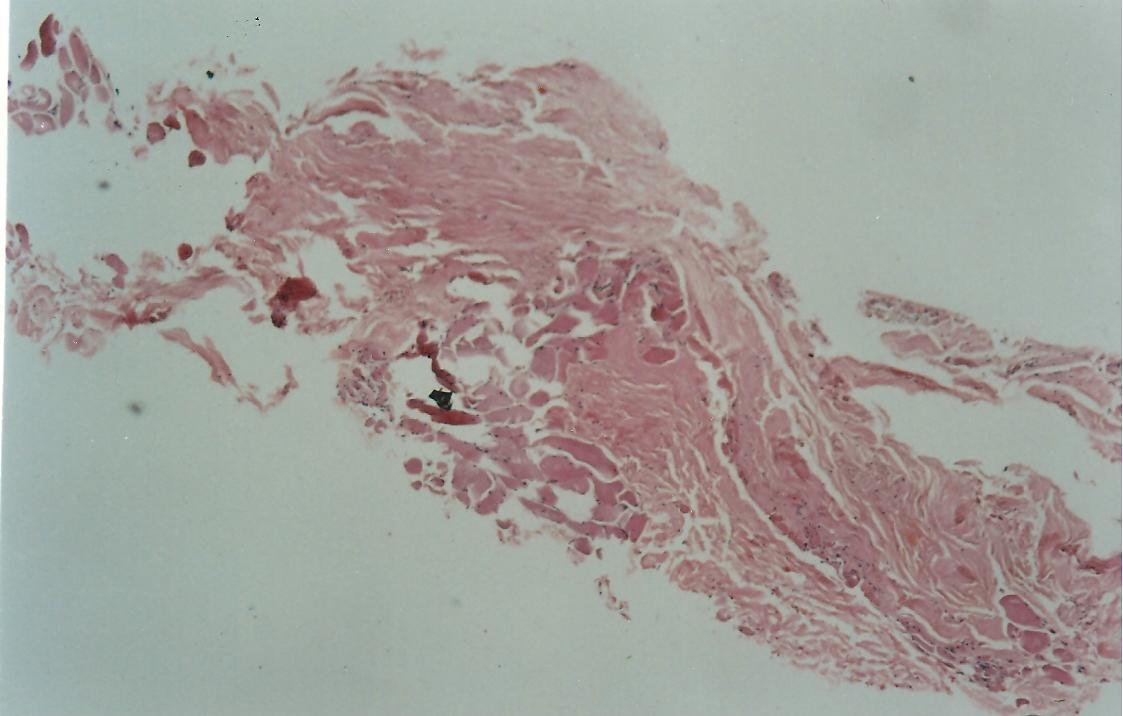
Download figure
The overall result showed that the success or graft take up rate was better in Technique I because of reasons explained below. We came to conclusion that the rough surface of medial side TMF after moistening created more friction and elasticity which resist the displacement between the tympanic membrane remnant.7, 16
Secondly studies in physics have proven that rough surface after wetting increases the critical surface tension and broadens the contact surface.8The role of surface tension was well studied by Cable HR in 1981.7
Thus surface tension plays a great role in stability of the graft on rough surface as compared to the smooth surface of the lateral side of the TMF graft. It has also been established that graft stability increases in proportion to the distance of overlap between the graft and tympanic membrane remnant.7, 15
So as the rough medial side of TMF graft after moistening increases the critical surface tension and widens the contact surface which decreases the gap between the graft and mucous membrane of the TM remnant. These may be the reasons for giving better result in Technique I as compared to Technique II. We had an overall success rate of 91.2% (73 out of 80 cases) with 95% success rate in Technique I and 87.1% success rate in Technique II.
In the entire failure rate was – 6.8% (7 cases out of 80). This was ascribed to post operative infection. The overall healing time was also less in technique I as compared to technique II.
Graft take up rate was not significant, but definitely Technique I gave better result than Technique II.
Absence of previous studies makes it difficult to compare with this study. It is hoped that our study will encourage other Otologist to do similar studies to duplicate our results.
Conclusion:
In conclusion this is ‘first of its kind’ study in the literature, Technique I was shown to be better than Technique II because of the following reasons.
1.Rough surface after wetting increases the critical surface tension.
2.It also broadens the contact surface.
3.The friction due to rough surface resists the displacement forces between the graft and remnant of tympanic membrane.
4.Rough surface of the medial side of TMF increases adhesive power and increase the overlap between the two surfaces.
References
- 1.Wullstein H. (1952) Funktjonelle operationed in millelohr mit filfedes frelen spal teppen transplantales. Archiv Fur Ohren-Nasanund kahlke ptheil kinde;. 161, 442-55.
- 2.Zollner F. (1955) The principles of plastic surgery of sound conduction apparatus. , J laryngol Otol 69, 637-52.
- 3.Ortegren U.Tympanic membrane graft of full thickness skin, fascia and cartilage in its perichondrium. Acta Otolaryngology 1959; supplement 244.
- 6.J B Booth. (1973) Myringoplasty – Factors affecting results. Final report. , Journal of Laryngology & Otology 87, 1039.
- 7.Cable H R. (1981) Surface Tension and temporalis fascia graft. , Journal of Laryngology and Otology 95, 667-73.
- 9.Heermann H. (1960) Frommelfill plastic mit Faserngewebe von muskulus. temporalis nach begradung der vorderen gehorgangswand. Hals Nasin Ohrenh. 9; 136 – 7
- 10.Glasscock M E. (1973) Tympanic membrane grafting with fascia; overlay vs under surface technique. Laryngoscope. 83(5), 754-70.
- 11.Albu S, Babighian G, Trabalzini F. (1998) Prognostic factors in Tympanoplasty. , American Journal of Otology 19, 136-40.
- 12.Sheehy J L, GlassCock M E, 3rd. (1967) Tympanic membrane grafting with temporalis fascia. Arch Otolaryngol. 86(4), 391-402.
- 13.Jung T, Kim Y H, Kim Y H, Pork S K, Martin D. (2009) Medial or medio-lateralgraft tympanoplasty for repair of tympanic membrane perforation. , Int J Paediatr otorhinolaryngol; 73(7), 941-43.