
Influence of Regular Astigmatism on the Human Visual Cortex. A Functional Magnetic Resonance Imaging Study
Abstract
Purpose:
To describe a new functional magnetic resonance imaging (fMRI) method for measuring the influence of regular astigmatism, both against-the-rule (ATR) and with-the-rule (WTR), on the human visual cortex.
Setting:
Department of Ophthalmology, Jikei University School of Medicine, Tokyo, Japan.
Design:
Experimental study.
Methods:
Images were acquired in two healthy volunteers using a 1.5 T scanner equipped for echo planar imaging. Horizontal and vertical sine wave grating flickering at a frequency of 8 Hz were simultaneously presented during the 20-second stimulation period. During the control period , subjects fixated on a control target. Stimulations were performed under three different conditions that included with hard contact lenses that were equal to emmetropia without astigmatism (condition 1); with hard contact lenses and cylindrical glasses of +6.00D at 0°, imitating WTR (condition 2); and with hard contact lenses and cylindrical glasses of +6. 00 D at 90°, imitating ATR (condition 3). Raw data were processed using in-house software with the significance of activation determined by Statistical Parametric Mapping (SPM 99).
Results:
Although higher activation was found in the primary visual cortex for condition 1 versus conditions 2 and 3, activation in the dorsal pathway was higher in conditions 2 and 3 compared to condition 1. Dorsal pathway activation was also higher in condition 3 versus condition 2.
Conclusions:
Study findings showed the potential influence of ATR and WTR on the human visual cortex , with fMRI able to detect the influence of regular astigmatism on the visual cortex. Our current results suggest that fMRI may be useful in exploring the influence of astigmatism on vision.
Author Contributions
Academic Editor: Zheng Jiang, Johns Hopkins University School of Medicine
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2015 Takuya SHIBA, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Unlike in a normal eye that focuses rays of light on a single point, the astigmatic eye refracts two focal lines separated from each other by a focal interval 1. Furthermore, astigmatism is a typical refractive anomaly that can be roughly divided into regular astigmatism and irregular astigmatism. While regular astigmatism can be fully corrected by using a spectacle lens 2, irregular astigmatism is interrupted by a variety of alterations of the refractive corneal surface, thereby presenting different degrees of the astigmatism 3. Various studies performed in the field of ophthalmological surgery, especially studies involving surgeries of the anterior eye segment, have attempted to lessen induced cornea astigmatism 4, 5, 6, 7. Furthermore, both regular astigmatism 8, 9, 10, 11 and irregular astigmatism have recently become more treatable due to the progress that has been made in refractive surgery 12,13,14. The better medical treatments have also greatly contributed to achieving better diagnoses. For example, analysis of the radius of curvature and refractive power can be determined by kerato-refractometer 15, 16, analysis of the form of the whole cornea by corneal videokeratoscopy 17, 18, 19, and measurement of the total ocular profile of refraction by wavefront analysis 20, 21, 22. However, the influence of astigmatism on the visual pathway has yet to be fully investigated. Several studies have recently reported using functional magnetic resonance imaging (fMRI) to diagnose the visual pathway 23,24. fMRI is a noninvasive method that can be used for human brain activity imaging 25,26. We used this methodology to investigate the influence of regular astigmatism on the visual cortex in addition to trying to determine the influence of astigmatism on the visual pathway.
Subjects
Two normal healthy male volunteers (aged 27, 34 years) gave informed consent prior enrollment in the study. Both participants were right-handed, and had no history, past or current, of ophthalmologic, neurological, or psychiatric illness. Measurements were performed 6 times in each subject.
Methods
Device for Refractive Correction and Simulation
The left eye of both subjects was covered with an eyepatch. In the right eye, each subject wore a hard contact lens, which was set to emmetropia. Moreover, +6.00 diopter (D) glasses were positioned at two different angles, one at 0 degrees and the other at 90 degrees. These three different conditions were used to create emmetropia (condition 1), with-the-rule (WTR) astigmatism (condition 2), and against-the-rule (ATR) astigmatism (condition 3), respectively.
Visual Stimulation
Visual stimuli were back-projected onto a translucent screen placed at the subjects' feet. Subjects viewed the visual stimuli using the built-in mirror of a standard head coil. Stimuli were created using in-house software. The three types of visual stimulation used during the experiment are described below.
Stimulation 1
During the 20 second stimulation period, horizontal and vertical sine wave gratings were presented for 15 minutes within a circle of 9 degrees, with the simultaneous flickering set at a frequency of 8 Hz (Figure 1). This phase was defined as ‘activation’. During the control period, the subjects fixated on the control target. This target was a 50% grey circle of 9 degrees, with the fixation point located at the center (Figure 1). This phase was defined as the ‘baseline’. The stimulation and control periods were alternated 5 times during the entire sequence. Each stimulation was performed under the three different conditions (used during the study (conditions 1-3).
Stimulation 2
Activation of stimulation 2 was created by removing the horizontal line activation factor of stimulation 1 (Figure 1). All other conditions were kept the same as in stimulation 1.
Stimulation 3
Activation of stimulation 3 was created by removing the vertical line activation factor of stimulation 1 (Figure 1). All other conditions were kept the same as in stimulations 1 and 2.
Figure 1.Visual stimulations. (A) Activation phrase of stimulation 1. Presentation of horizontal and vertical sine wave gratings of 15 minutes in the circle of 9 degrees. (B) Control phrase of all stimulations. The control stimuli is the 50% grey circle of 9 degrees, with the fixation point at the center. (C) Activation phrase of stimulation 2. Stimulation was created by removing the ingredient of activation of stimulation 1 to horizontal lines. (D) Activation phrase of stimulation 3. Stimulation was created by removing the ingredient of activation of stimulation 1 to vertical lines.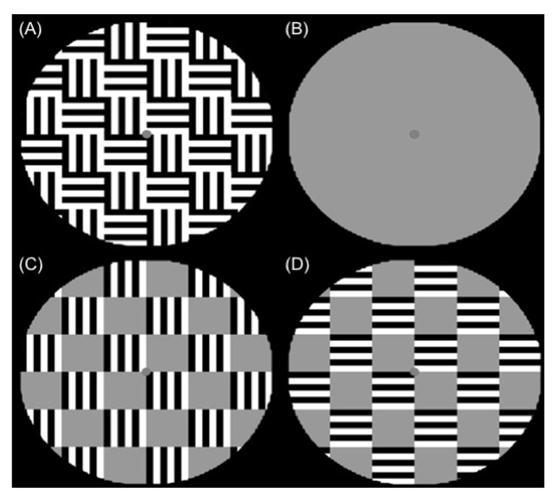
fMRI Experimental Procedure
fMRI was performed on a 1.5 Tesla GE Signa Echospeed system (General Electric, Milwaukee, WI, USA) and Siemens Magnetom Vision (Siemens, Erlangen, Germany) using a standard quadrature head coil (repetition time (TR) = 2000 ms, echo time (TE) = 60 ms, field of view (FOV) = 32 cm, matrix = 64 x 64, thickness = 5 mm). T1-weighted images were acquired and used to obtain three-dimensional structural images that helped locate the activated areas. Visual stimuli were presented in a boxcar design 27.
Data Analysis
After acquisition, images were converted from the native GE or Siemens format to the format used to analyze the data in the current study. After the image processing steps, data analysis was performed using statistical parametric mapping (SPM99; Wellcome Department of Cognitive Neurology, London, UK). After uniting the position of each image, all volumes were realigned to the first volume. Spatial smoothing of the functional signal within each slice was performed prior to the analysis. We then defined a design matrix that consisted of contrast modeling of the alternating periods of ‘baseline’ and ‘activation’ when using a delayed boxcar reference vector 27 that accounted for the delayed cerebral hemodynamic response function after the stimulus presentation. Data were first analyzed for neural activations that were common to the experimental conditions relative to the baseline. To determine the statistical significance, we used a corrected significance level of the individual voxel of P < 0.005 and a cluster size of 26, with an AlphaSim-corrected cluster threshold of P < 0.05.
Results
Stimulation 1
Remarkably consistent activations were detected bilaterally for each condition in the primary visual cortex (Figure 2). The amplitude of the vascular response for condition 1 was higher than that for conditions 2 and 3 in the primary visual cortex (Figure 3). For conditions 2 and 3, activation led to responses in the dorsal visual pathway (Figure 2). Furthermore, the range that showed activation was larger in condition 3 versus condition 2 (Figure 2). For the fitted response and PSTH (peri-stimulus time histogram), the condition 1 response was higher than that seen for conditions 2 and 3 in the primary visual cortex (Figure 4). Moreover, the fitted response and PSTH for the condition 2 and 3 responses were higher than that observed for condition 1 in the dorsal visual pathway (Figure 5)
Figure 2.Result of stimulation 1. The black areas denote active brain regions (P<0.05). (A) Condition 1. Activations was detected in bilaterally primary visual cortex. (B) Condition 2. Activations was detected in bilaterally primary visual cortex and dorsal visual pathway. (C) Condition 3. Activations was detected in bilaterally primary visual cortex and dorsal visual pathway.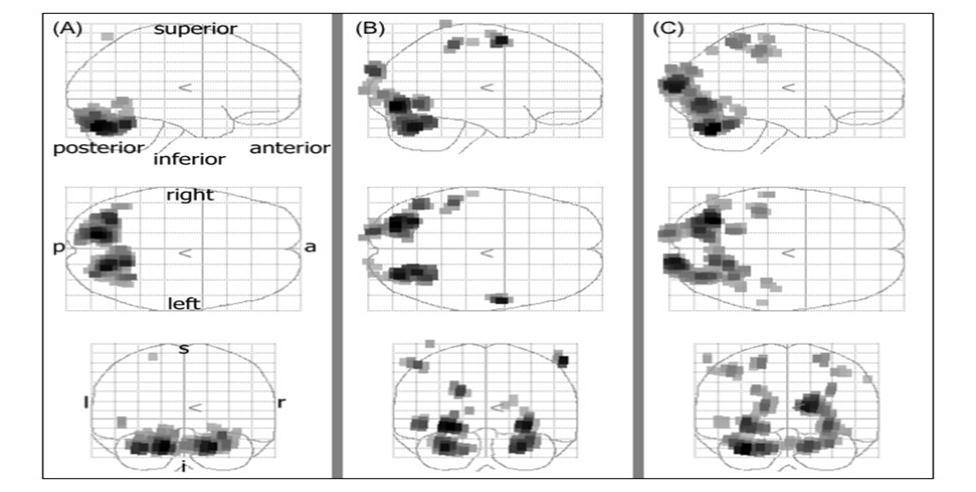
Figure 3.The amplitude of vascular response of primary visual cortex.The amplitude of vascular response of condition 1 (1) was higher than condition 2 (2) and 3 (3) (P<0.05).
Figure 4.Fitted response and PSTH in primary visual cortex. The average response to an event type with mean signal +/- SE for each peri-stimulus time bin. Response of condition 1 (1) was higher than condition 2 (2) and 3 (3) in primary visual cortex (P<0.05).
Figure 5.Fitted response and PSTH in dorsal visual pathway. The average response to an event type with mean signal +/- SE for each peri-stimulus time bin. Response of condition 2 (2) and 3 (3) was higher than condition 1 (1) in dorsal visual pathway (P<0.05).
Stimulation 2
Although activation was bilaterally detected for conditions
1 and 2 in the primary visual cortex, (Figure 6), it was not detected for condition 3 (Figure 6). For condition 2, activation led to a response in the dorsal visual pathway (Figure 6).
Figure 6.Result of stimulation 2. The black areas denote active brain regions (P<0.05). (A) Condition 1. Activations was detected in bilaterally primary visual cortex. (B) Condition 2. Activations was detected in bilaterally primary visual cortex. (C) Condition 3. Activations was not detected in primary visual cortex.
Stimulation 3
Activation was bilaterally detected for conditions 1 and 3 in the primary visual cortex (Figure 7), but was not detected for condition 2 (Figure 7). For condition 3, activation led to a response in the dorsal visual pathway (Figure 7).
Figure 7.Result of stimulation 3. The black areas denote active brain regions (P<0.05). (A) Condition 1. Activations was detected in bilaterally primary visual cortex. (B) Condition 2. Activations was not detected in primary visual cortex. (C) Condition 3. Activations was not detected in primary visual cortex.
Discussion
Several studies have investigated both the influence of astigmatism on vision, and the evaluation methods used to examine astigmatism 28, 29. However, these studies only examined the influence and the evaluation methods in the anterior and posterior eye segments. In the current study, we investigated astigmatism influence on the visual pathway located beyond the posterior eye segment.
Recent studies have reported using the fMRI cerebral functional appraisal method to evaluate the influence of regular astigmatism on the visual cortex. For more than ten years, fMRI has been used to evaluate cerebral function 25, 26. This method calculates brain activity, by measuring the induction of regional cerebral blood flow changes. Although there are several different ways that the fMRI measurements can be made 30, 31, 32, we used the blood oxygenation level dependent (BOLD) method 30 in our study. This method determines the hemodynamic changes associated with the variations in the amount of blood flow that accompany the brain activity, which is partly based on the phenomenon of magnetic resonance. The amount or speed of the inflow of blood to a peripheral blood vessel floor increases in conjunction with the activity of cerebral cortex is anaerobic, there is a fall in the ratio of the deoxy hemoglobin / oxy hemoglobin relative to the blood vessel floor 33. In the human body, deoxy hemoglobin is a magnetic substance, and thus, is capable of creating a detectable magnetic resonance signal. The BOLD fMRI method measures the rise and fall of this magnetic resonance signal, and thus, does not require the injection of a contrast media.. Since this method can be quickly performed and used to simultaneously measure the entire brain, there has been a rapid increase in the use of fMRI in many different types of studies
When a seeing on subject with WTR astigmatism views an object at a long distance, the image will be distorted perpendicularly, while a subject with ATR astigmatism will find the image to be distorted horizontally 34. In the current study, stimulation 1 was designed so that the subject would experience WTR and ATR astigmatism. we used stimulation 1. To achieve this stimulation, subjects were simultaneously presented with an image that contained the same quantity of vertical and horizontal lines. In a previous study that examined the developmental origins of visual perception, visual circuity involved with the processing of vertical and horizontal contours was found to be important in the enhanced visual capabilities of humans 35. Furthermore, since these contours and conditions are found throughout an image, our stimulations were designed to be circular in shape. The stimulation used in condition 1 resulted in a higher amplitude of vascular response as compared to that seen in conditions 2 and 3. It has been suggested that both WTR and ATR astigmatism can adversely influence the primary visual cortex. In conditions 2 and 3, activation led to a response in dorsal visual pathway. The dorsal visual pathway carries vision information going to the parietal association area from area V1. This pathway is roughly divided into two, with one section going to area 7 via the medial superior temporal area (MST) 36,37, ventral intraparietal area (VIP) 38, middle temporal area (MT) 39,40, etc. This pathway is involved in the analysis of visual motion. The other pathway goes to the lateral intraparietal area (LIP) or the caudal intraparietal sulcus area (cIPS) via the V3A and PO. areas. It is thought that this pathway is related to the objective position or the information processing of the three-dimensional form 41, 42. However, the exact nature of this pathway has yet to be fully understood. The activation response in the dorsal visual pathway observed for conditions 2 and 3 suggests that astigmatism can influence activation whithin the dorsal visual pathway. However, the question of what the exact nature of this influence really is remains to be answered. If the direction of the line of the stimuli and the axis of the astigmatism are in agreement, then the line will be extended in this direction as it is projected on the retina. In contrast, when the directions of the line of the stimuli and the axis of the astigmatism differ, the line fades as it is projected on the retina. Thus, this suggests that this phenomenon is the visual factor responsible for generating noise on the retina can be considered. When stimulation 1 was presented through the range that resulted in activation, the response for condition 3 was larger than that for condition 2. However, there was no difference between stimulation 2 for condition 2 and stimulation 3 for condition 3. Moreover, the large difference seen between conditions 2 and 3 was not observed between stimulation 2 with condition 3 and stimulation 3 with condition 2. This suggests that ATR astigmatism may have a greater influence on the visual noise as compared to the WTR astigmatism.
In studies of ophthalmological surgeries, especially surgeries of the anterior eye segment, there have been several attempts to find ways to lessen induced cornea astigmatism if possible have been attempted 4, 7. One study reported that a superior incision induced ATR astigmatism 43. Although the position of the incision during cataract surgery can be due to a variety of reasons 44, 45, 46 the overall outcomes seen in these cases have led to the creation of a defined protocol when performing these surgeries in the general population. Moreover, although there have been many reported cases of WTR astigmatism in young men, there have been other studies that have found that aging can cause a large number of people to develop ATR astigmatism 47, 48, 49. Irregular astigmatism is commonly treated by laser in situ keratomileusis (LASIK), using the wavefront technique 12, 14. After this medical treatment, the cornea temporarily becomes a perfect surface of a sphere. However, a large number of corneas could change to ATR astigmatism with aging. Thus, it will be necessary to closely follow these subjects in order to determine the validity of this hypothesis in the future.
Ophthalmologists need to pay close attention to basic fundamental abnormalities, such as WTR and ATR astigmatism, in order to ensure patients receive the best possible ophthalmological care.
References
- 1.Duke-Elder W S, Abrams D. (1970) . System of Ophthalmology (Vol.5) , London, England: Henry Kimpton 283-285.
- 2.Duke-Elder W S, Abrams D. (1970) . System of Ophthalmology (Vol.5) , London, England: Henry Kimpton 288.
- 3.Duke-Elder W S, Abrams D. (1970) . System of Ophthalmology (Vol.5) , London, England: Henry Kimpton 365.
- 4.Neumann A C, McCarty G R, Sanders D R, Raanan M G. (1989) Small incisions to control astigmatism during cataract surgery. J Cataract Refract Surg. 15(1), 78-84.
- 5.Holladay J T, Cravy T V, Koch D D.Calculating the surgically induced refractive change following ocular surgery.JCataractRefractSurg.1992Sep;18(5):. 429-43.
- 6.Gills J P.Cataract surgery with a single relaxing incision at the steep meridian. JCataractRefract Surg.1994May;20(3):. 368-9.
- 7.Tsuneoka H, Shiba T, Takahashi Y.Ultrasonic phacoemulsification using a 1.4 mm incision: clinical results.JCataractRefractSurg.2002Jan;28(1):. 81-6.
- 8.S Leroux Les Jardins, Frish E, Bertrand I, Massin M.Congenital myopic astigmatism: results of surgery using the Thornton T-CUTS technic, combined with radial keratotomy Bull Soc Ophtalmol Fr.1989Dec;89(12):. 1379-84.
- 9.McCarey B E, Amos C F.Topographic evaluation of toric soft contact lens correction.CLAOJ.1994Oct;20(4):. 261-5.
- 10.Molina R, Monasterio R, Soliz E, Foianini J.Correction of astigmatism using positive and negative cylinder programs with the Nidek EC-5000 excimer laser.JRefractSurg.1999Mar-Apr;15(2 Suppl):S195-6.
- 11.Gills J P, MA Van der Karr.Correcting high astigmatism with piggyback toric intraocularlensimplantation.JCataractRefractSurg.2002Mar;28(3);547-9,Surg,2003Mar-Apr;19(2 Suppl);S209-16..
- 12.Seiler T, Mrochen M, Kaemmerer M. (2000) Operative correction of ocular aberrations to improve visual acuity.JRefractSurg.2000Sep-Oct;16(5):S619-22..
- 13.Mrochen M, Kaemmerer M, Seiler T. (2000) Wavefront-guided laser in situ keratomileusis: early results in three eyes.JRefractSurg.2000Mar-Apr;16(2):. 116-21.
- 14.Gimbel H V, Sofinski S J, Mahler O S, van Westenbrugge JA, Ferensowicz M I et al. (2003) Wavefront-guided multipoint (segmental) custom ablation enhancement using the Nidek NAVEXplatform.JRefractSurg.2003MarApr;19(2 Suppl):S209-16.
- 15.Westheimer G, Felsenstein L.Automatic photoelectric keratometer.JOptSocAm.1966Jun;56(6):. 807-10.
- 16.Tennen D G, Keates R H, Montoya C.. Comparison of three keratometry instruments.JCataractRefractSurg.1995 Jul;21(4): 407-8.
- 17.Klyce S D, Wilson S E, Kaufman H E. (1989) . , Corneal topography comes of of age.RefractCornealSurg.1989Nov-Dec; 5(6), 359-61.
- 18.Oshika T, Tomidokoro A, Tsuji H. (1998) Regular and irregular refractive powers of the front and back surfaces of the cornea. Exp Eye Res.1998 Oct. 67(4), 443-7.
- 19.Maeda N. (2002) Evaluation of optical quality of corneas using corneal topographers. , Cornea,Oct;21 21(7(Suppl)), 75-8.
- 20.Liang J, Grimm B, Goelz S, Bille J F. (1994) Objective measurement of wave aberrations of the human eye with the use of a wave-front sensor. J Opt Soc Am A,Jul;. 11(7), 1949-57.
- 21.Salmon T O, Thibos L N, Bradley A. (1998) Comparison of the eye's wave-front aberration measured psychophysically and with the Shack-Hartmann wave-front sensor. J Opt Soc Am A Opt Image Sci Vis,Sep. 15(9), 2457-65.
- 22.Hofer H, Artal P, Singer B, Aragon J L, Williams D R. (2001) Dynamics of the eye's wave aberration. J Opt Soc Am A Opt Image Sci Vis,Mar;. 18(3), 497-506.
- 23.Zeki S, Watson J D, Frackowiak R S. (1993) Going beyond the information given: the relation of illusory visual motion to brain activity. Proc R Soc Lond B Biol Sci,Jun . 252(1335), 215-22.
- 24.Engel S A, Glover G H, Wandell B A. (1997) Retinotopic organization in human visual cortex and the spatial precision of functional MRI. Cereb Cortex,Mar. 7(2), 181-92.
- 25.Cohen M S, Bookheimer S Y. (1994) Localization of brain function using magnetic resonance imaging. Trends Neurosci,Jul. 17(7), 268-77.
- 26.Courtney S M, Ungerleider L G. (1997) What fMRI has taught us about human vision. Curr Opin Neurobiol,Aug. 7(4), 554-61.
- 28.Eisenmann D, Wagner R, Dick B, Jacobi K W. (1996) Effect of corneal astigmatism on contrast sensitivity in mono- and multifocal pseudophakia--a theoretical study of the physical eye Klin Monatsbl Augenheilkd,Aug-Sep 209(2-3):125-31..
- 29.Guirao A, Porter J, Williams D R, Cox I G. (2002) Calculated impact of higher-order monochromatic aberrations on retinal image quality in a population of human eyes. J Opt Soc Am A Opt Image Sci Vis,Mar. 19(3), 620-8.
- 30.Ogawa S, Lee T M, Nayak A S, Glynn P. (1990) Oxygenation-sensitive contrast in magnetic resonance image of rodent brain at high magnetic fields. Magn Reson Med,Apr. 14(1), 68-78.
- 31.Rosen B R, Belliveau J W, Vevea J M, Brady T J. (1990) Perfusion imaging with NMR contrast agents. Magn Reson Med,May;. 14(2), 249-65.
- 32.Edelman R R, Siewert B, Darby D G, Thangaraj V, Nobre A C et al. (1994) Qualitative mapping of cerebral blood flow and functional localization with echo-planar MR imaging and signal targeting with alternating radio frequency. Radiology,Aug;. 192(2), 513-20.
- 33.Fox P T, Raichle M E, Mintun M A, Dence C. (1988) Nonoxidative glucose consumption during focal physiologic neural activity. Science,Jul 22. 241(4864), 462-4.
- 34.Duke-Elder W S, Abrams D. (1970) . System of Ophthalmology (Vol.5) , London, England: Henry Kimpton 275.
- 35.Coppola D M, Purves H R, McCoy A N, Purves D. (1998) The distribution of oriented contours in the real world. Proc Natl Acad Sci U S A,Mar 31; 95(7), 4002-6.
- 36.Saito H, Yukie M, Tanaka K, Hikosaka K, Fukada Y et al. (1986) Integration of direction signals of image motion in the superior temporal sulcus of the macaque monkey. J Neurosci,Jan;. 6(1), 145-57.
- 37.Sakata H, Shibutani H, Ito Y, Tsurugai K, Mine S et al.1994. Functional properties of rotation-sensitive neurons in the posterior parietal association cortex of the monkey. Exp Brain Res. 101(2), 183-202.
- 38.Colby C L, Duhamel J R, Goldberg M E. (1993) Ventral intraparietal area of the macaque: anatomic location and visual response properties. J Neurophysiol,Mar;. 69(3), 902-14.
- 39.Albright T D, Desimone R, Gross C G. (1984) Columnar organization of directionally selective cells in visual area MT of the macaque. J Neurophysiol,Jan;. 51(1), 16-31.
- 40.Albright T D. (1992) Form-cue invariant motion processing in primate visual cortex. Science,Feb 28. 255(5048), 1141-3.
- 41.Andersen R A, Essick G K, Siegel R M. (1985) Encoding of spatial location by posterior parietal neurons. Science,Oct 25;. 230(4724), 456-8.
- 42.Andersen R A, Snyder L H, Bradley D C, Xing J.Multimodal representation of space in the posterior parietal cortex and its use in planning movements. Annu Rev Neurosci,20:. 1997, 303-30.
- 43.Oshika T, Sugita G, Tanabe T, Tomidokoro A, Amano S. (2000) Regular and irregular astigmatism after superior versus temporal scleral incision cataract surgery. Ophthalmology,Nov;. 107(11), 2049-53.
- 44.Nielsen J. (1993) Induced astigmatism and its decay with a frown incision. J Cataract Refract Surg,May;. 19(3), 375-9.
- 45.Jacobs B J, Gaynes B I, Deutsch T A. (1999) Refractive astigmatism after oblique clear corneal phacoemulsification cataract incision. J Cataract Refract Surg,Jul;. 25(7), 949-52.
- 46.Nagaki Y, Hayasaka S, Kadoi C, Matsumoto M, Yanagisawa S et al. (2003) Bacterial endophthalmitis after small-incision cataract surgery. effect of incision placement and intraocular lens type. J Cataract Refract Surg,Jan;. 29(1), 20-6.
- 47.Baldwin W R, Mills D. (1981) A longitudinal study of corneal astigmatism and total astigmatism. , Am J Optom Physiol Opt,Mar; 58(3), 206-11.
- 48.Hayashi K, Masumoto M, Fujino S, Hayashi F. (1993) Changes in corneal astigmatism with aging. Nippon Ganka Gakkai Zasshi,Oct;. 97(10), 1193-6.
- 49.Gudmundsdottir E, Jonasson F, Jonsson V, Stefansson E, Sasaki H et al. (2000) With the rule" astigmatism is not the rule in the elderly. Reykjavik Eye Study: a population based study of refraction and visual acuity in citizens of Reykjavik 50 years and older. Iceland-Japan Co-Working Study Groups. Acta Ophthalmol Scand,Dec;. 78(6), 642-6.
Cited by (1)
This article has been cited by 1 scholarly work according to:
Citing Articles:
Journal of Ophthalmic Science (2015) OpenAlex