
High-Resolution SD-OCT and EDI-OCT in the Evaluation and Management of Multifocal Serpigenoed Choroditis
Abstract
Purpose
To describe spectral domain optical coherence tomography (SD-OCT) and enhanced depth image OCT (EDI-OCT) findings of multifocal serpiginoid choroditis (MSC) , including affected layer of retinal involvement, changes at the vitreoretinal interface, and response to therapy.
Methods
A retrospective review of 20 eyes (14 patients) with MSC. Each patient underwent a complete ophthalmologic examination, fundus photography, fundus autoflorecence (FAF) and OCT imaging of the affected retina at the initial visit and on each follow-up.
Results
In acute stage, SD-OCT showed hyperreflective areas involving the outer retinal layers which include retinal pigment epithelium (RPE), photoreceptor outer segment tips (POST), inner segment–outer segment (IS/OS) junction, external limiting membrane (ELM), and outer nuclear layer (ONL) with choroidal and intraretinal layer cells infiltrate. EDI-OCT showed increase choroidal thickness.
As the lesions began to heal, irregular, knobby elevations of outer retinal layers appeared (RPE, POST, IS/OS junction, and ELM could not be distinguished) with significant decrease in choroidal and intraretinal cells.
On complete healing, loss of RPE, POST, IS/OS junction, and ELM in SD-OCT scan and absent of the choroidal and intraretinal cells and continous hyperreflactivity of the choroid (increased penetrance).
Conclusion
SD-OCT and EDI-OCT provides high-resolution detail regarding ultrastructural changes in vitreoretinal interface, outer retina and choroid during the course of the lesion. Serial SD-OCT and EDI-OCT also provides further insight into response to therapy by observing choroidal and intraretinal cells.
Article Information
- Received
- Accepted
- Published
Academic Editor: Chang Liu, Johns Hopkins University, China.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Eman Abo Taleb, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Corresponding author: Eman Abo Taleb, Retina Foundation, Asopalav Eye Hospital, Rajbhavan road, Underbridge, Shahibaug, Ahmedabad – 380 004, Gujarat, India —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Serpiginous choroiditis is a progressive, chronic, recurrent inflammatory disease primarily affecting the inner choroid and retinal pigment epithelial (RPE) cell layer.1 Serpiginoid multifocal choroiditis (MSC) is a distinct clinical entity that begins usually as multifocal choroiditis lesions that coalesce and progress in a serpiginoid pattern. (MSC) a designation that better reflects the clinical features of presumed tubercular etiology and is preferable to the previously used serpiginous-like choroiditis(SLC).2 While the choriocapillaries have been shown to be the most affected layer in serpiginous choroiditis (SC), the primary site of inflammation in MSC is not yet known and is at best speculated, presumably the choriocapillaries.3
Since its introduction in 1991, optical coherence tomography (OCT), has found its place as a widely accepted imaging technique, especially in ophthalmology and other biomedical applications. It represents an interferometric, non-invasive optical tomographic imaging technique offering millimetre penetration with submicrometre axial and lateral resolution.4
The simultaneous recordings of topographic and tomographic images by using combination of scanning laser ophthalmoscopy and optical coherence tomography (OCT) have increased our understanding of the pathogenesis of various diseases of the retina and choroid.3 The Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Germany) is a novel multimodal imaging device that enables us to correlate confocal angiograms, fundus autofluorescence (FAF) images, and other imaging modes with the high resolution spectral domain (SD)-OCT scans.3The Spectralis HRA+OCT has been used in imaging the choroid in intraocular inflammation using the inverted scan technique.
The role of OCT in patients with uveitis is complementary to the conventional fundus photography and fundus fluorescein angiography (FA).In the last years, noninvasive FAF imaging has been introduced into the ophthalmological clinical practice, providing for the first time a qualitative measure of the status of RPE layer in terms of function and structure.5 This has been shown to especially useful for the evaluation of various retinal disorders. As a result, there has been an increased interest in the role of FAF in the assessment and follow-up of inflammatory diseases of retina and RPE choroid complex.6
We describe the changes in high-resolution SD-OCT scans that were simultaneously obtained with FAF signals on Spectralis HRA+OCT in 14 patients with MCS who were followed from the stage of acute lesion to the healed stage over a period of 3–6 months.
In an attempt to explore the extent of choroidal involvement during various phases of MSC, we prospectively studied the EDI-OCT changes in eyes with tubercular MSC.
Methods
We retrospectively review of 20 eyes (14 patients) with MCS. The diagnosis of MCS was made in the presence of multifocal choroiditis lesions with central healing and active edges that were hyperautofluorescent in areas of active edges and hypoautofluorescent in healed areas and showed early hypofluorescence and late hyperfluorescence of active lesions on FAF. The etiology was presumed to be tubercular if there was at least two of the following criteria (1) a positive tuberculin skin test (2) QuantiFERON-TB Gold test (3) abnormal chest radiography (4) history of relative who has TB (5) a favorable therapeutic response to antitubercular therapy . We exclude of all other known causes of infectious uveitis except tuberculosis and noninfectious uveitic syndromes.
Besides a complete clinical evaluation that included best-corrected visual acuity (BCVA), intraocular pressure (IOP), slit lamp biomicroscopic examination, and conventional imaging methods (digital photography and FA, when required, on
Visupac 450 Plus, Carl Zeiss, Jena, Germany), these patients additionally underwent Spectralis HRA+OCT (Heidelberg Engineering, Heidelberg, Germany) imaging with simultaneously obtained FAF and OCT images at all follow-ups. The Spectralis system uses Heidelberg Eye Explorer Software Version 1.5.0 with Image Capture Module Version 1.1.0. An infrared fundus image was acquired parallel to OCT scan to ensure correct placement of image before acquiring FAF images simultaneous with OCT scans. The pupils were dilated before acquiring all scans. The Spectralis scans along with the FAF images were obtained before doing FA, using the 30° field-of-view mode. All images were recorded using the automatic real time mode. The image acquisition was done by selecting the dense volume scan type over a scan angle of 20° or 30°and by the width/height of the OCT scan(depending upon the extent of the lesions in the fundus).
We routinely perform dense volume scan with simultaneous FAF and SD-OCT mode. We use infrared mode to focus the fundus image, and once focused, we switch to combined FAF and SD-OCT mode and capture the images simultaneously.
An integrated eye tracking allowed for live averaging of FAF images and the SD-OCT scans. The baseline FAF-OCT images were defined as the reference images to enable acquisition of images at the same site during follow-up visits. Patients were seen every 2 weeks until the lesions healed.
In addition to oral corticosteroids, all patients received four-drug antitubercular therapy including isoniazid (5 mg/kg/day), rifampicin (450 mg/day if body weight was ≤50 kg and 600 mg/day if body weight was >50 kg), ethambutol (15 mg/kg/day), and pyrazinamide (25 to 30 mg/kg/day) initially for 3 to 4 months. Thereafter, rifampicin and isoniazid are used for another 9–14 months. Pyridoxine supplementation was given to all patients receiving antitubercular therapy until cessation of therapy.
The corticosteroids were tapered depending upon the clinical response. All patients were receiving antitubercular therapy until their last visit and did not show any recurrence of inflammation. Demographic details and treatment response to oral corticosteroids and antitubercular therapy were also noted. The OCT scans were analyzed and correlated with FAF/FA images in acute as well as healing stages.
Results
We studied 20 eyes (14 patients) with active MSC, who were followed-up from acute stage up to the final healed stage. Ten patients had unilateral active MSC, and 4 patients had bilaterally active disease at the time of presentation to our clinic. There were 8 men and 6 women. The mean age was 34.35+10.77 years (range, 19–53 years). TB Mantox test was positive in all patients except one case was diagnosed by chest CT-scan. Presenting BCVA Rt (mean 0.63+0.79) and Lt (mean0.40+0.63). 8 patient present at acute stage , 6 at healing stage and only one case at healed stage. The mean follow-up was10.53 +11.78 months (median, 4 months; range, 2–42 months).
During the course of the disease in patients with MSC, we observed a progressively changing pattern on SD-OCT scans that was consistent with the abnormal FAF signals detected simultaneously.
1. In an acute lesion of MCS, there was an ill-defined area of increased autofluorescence around the lesion. The SD-OCT passing through the area showed a localized, fuzzy area of hyperreflectivity in the outer retinal layers involving the RPE, photoreceptor outer segment tips (POST), photoreceptor inner segment–outer segment (IS/OS) junction, external limiting membrane (ELM), and the outer nuclear layer (ONL). The lesion was localized external to the outer plexiform layer with a mild distortion of the inner retinal layers. Choroidal and intra retinal layer cells infiltrate with corresponding increase thickness of choroid and inner retinal layers more obvious in EDI-OCT. There was no increased backscattering from the inner choroid.
2. As the lesions started to heal, they became well defined and acquired a thin border of hypoautofluorescence while remaining predominant hyperautofluorescent centrally. The SD-OCT scan through the hyperautofluorescent area showed disappearance of the hyperreflective fuzzy areas that were replaced by irregular, hyperreflective knobbly elevations of the outer retinal layers. The RPE, the POST, IS/OS junction, and the ELM could not be distinguished. The ONL appeared normal. At this stage, there was an increased reflectance from the choroidal layers due to attenuating RPE–photoreceptor complex.
3. As the lesions healed further over the next 3–6 months, they appeared stippled with predominantly hypoautofluorescence. The SD-OCT scan showed loss of RPE, POST, IS/OS junction, and ELM with absent of the choroidal and intraretinal cells. The increased reflectance from the choroid persisted.
Case Example
Patient1
A 34-year-old male presented with decreased vision in Right eye since one and half month. On examination, the BCVA was 6/ 60 and 6/6 in the right and left eyes, respectively. Both eyes showed unremarkable anterior segment and multifocal lesions of active as well as inactive choroiditis in the posterior pole of Right eye and healed choroditis on left eye (Figure 1). Simultaneous FAF and SD-OCT imaging of the right eye revealed findings as explained in the “Results” Section (1.) (Figure 2). The tuberculin skin test was positive. He received four-drug antitubercular therapy with oral corticosteroids. About 2 weeks later, the lesions started to heal and appeared as described in “Results” Section (2.) (Figure 3). Three months later, the lesions healed further and appeared as explained in “Results” Section (3.) (Figure 4). Figure 5, Figure 6.
Figure 1. Color photograph of the right eye of patient 1shows an active MSC (blue arrows) and left eye shows healed MSC from her initial visit
Download figure
Figure 2. FAF (left) and corresponding eye-tracked SD-OCT image (right) of patient 1 an acute stage of the right eye shows fuzzy area of hyperreflectivity in the outer retinal layers involving the RPE, photoreceptor outer segment tips (POST), photoreceptor inner segment–outer segment (IS/OS) junction, external limiting membrane (ELM), and the outer nuclear layer (ONL) with vitreal and choroidal cells
Download figure
Figure 3. FAF (left) and corresponding eye-tracked SD-OCT image (right) of patient 1 during healing stage of the right eye shows hyperreflective knobbly elevations of the outer retinal layers. The RPE, the POST, IS/OS junction, and the ELM could not be distinguished. The ONL appeared normal with increased reflectance from the choroidal layers.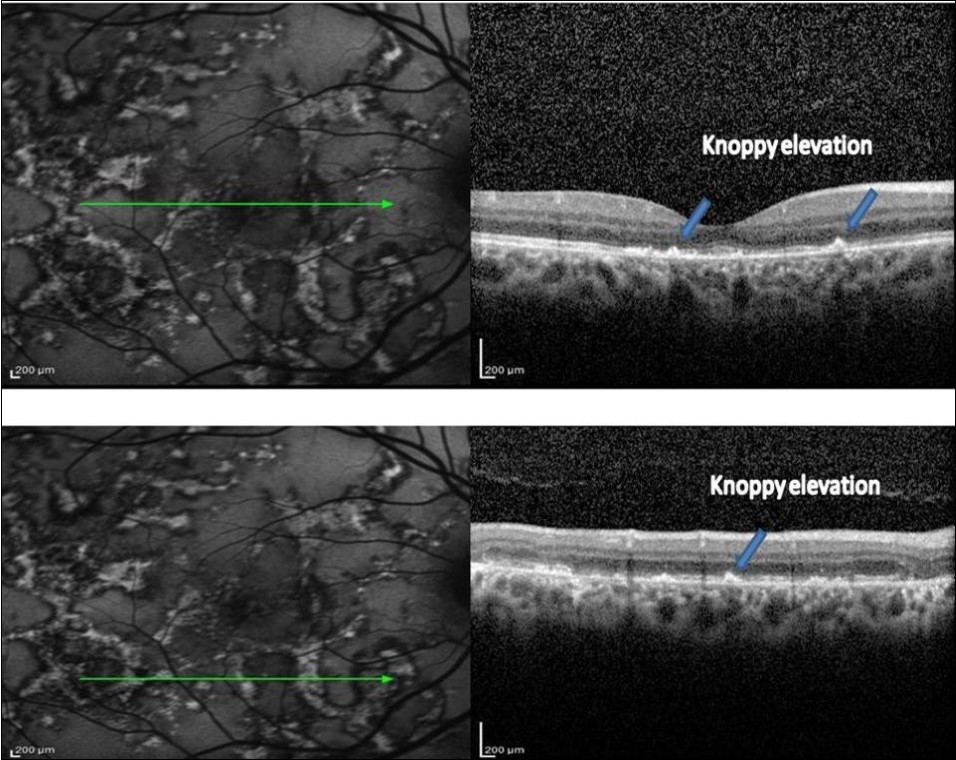
Download figure
Figure 4. FAF (left) and corresponding eye-tracked SD-OCT image (right) of patient 1 healed stage of the left eye shows showed loss of RPE, POST, IS/OS junction, and ELM with increased reflectance from the choroidal layers. absent of the choroidal and intraretinal cells.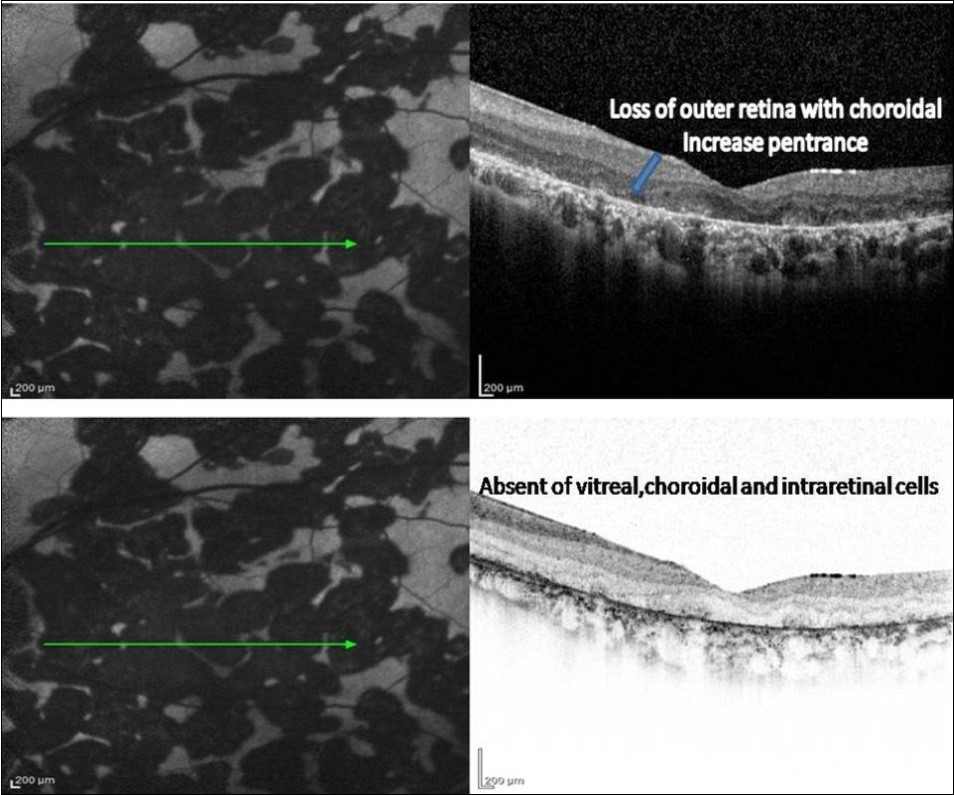
Download figure
Figure 5. FAF (left) and corresponding eye-tracked SD-OCT image (right) of an example of transition area of anactive MSC (between red arrows) with no backscattering from the choroid .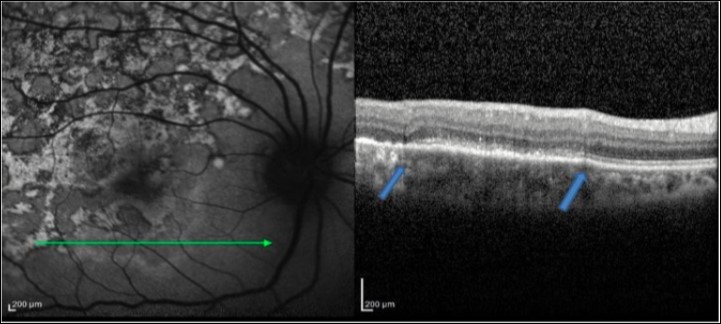
Download figure
Figure 6. EDI-OCT in acute stage of MSC reveled increase choroidal thickness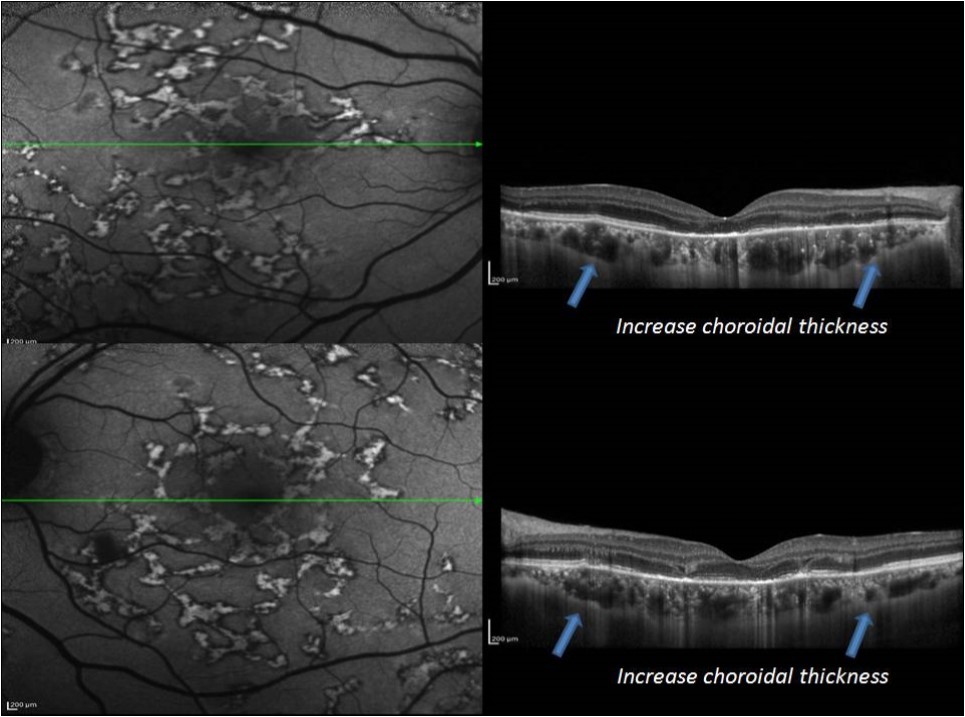
Download figure
Discussion
Tuberculosis –Infectious causes of what might clinically be called SC have been referred to as both ‘‘serpiginous-like choroiditis’’ and, more recently, multifocal serpidinoid choroiditis (MSC).7 In North India, MSC is frequently bilateral, typically associated with vitreous inflammation, and affects young to middle-aged men predominantly. Anterior chamber inflammation is typically mild or absent. The choroiditis of MSC tends to begin as multiple, discrete lesions in the posterior pole and mid-periphery, which then coalesce over time. A combination of systemic corticosteroids and antituberculosis treatment (ATT) is highly effective at controlling the inflammation and preserving the visual acuity.7
Although pathogenesis, etiology, and differential diagnosis of the SC and MSC remain a challenge, PCR studies to detect microbial DNA reveal that Mycobacterium tuberculosis (MTB) play a role in patients with MSC.2 The main histological findings described in SC are atrophy of the choriocapillaries, the RPE, and the photoreceptors.8,9 While the choriocapillaries was reported to be the most affected layer that appeared acellular, the large choroidal vessels were unremarkable. Moderate, diffuse lymphocytic infiltration of the choroid has been reported, with predominant RPE atrophy. Occasionally, RPE hypertrophy has been seen correlating with areas of pigment clumping clinically.8,9On the other hand, clinicopathological correlation in tubercular MSC is still not known.
Clinically, MSC appears to involve primarily the inner choroid and the RPE. However, isolation of Mycobacterium tuberculosis from the RPE in an eye with tubercular panuveitis has strongly suggested preferential localization of the mycobacteria in the RPE, even in eyes with panuveitis or related intraocular inflammation, including multifocal choroiditis or serpiginous like choroiditis.10High-speed, high-resolution OCT, by providing unprecedented details, has enhanced our understanding of the ultrastructure of the retina.3
Hossein Nazari and et al study OCT features of active SC lesions and they observe disruption of photoreceptor layer associated with outer retinal and choriocapillaris hyperreflectivity.2 In active choroiditis, the outer retina shows a uniform increased reflectivity, but the inner retina is usually spared. Outer retina may appear hyperreflective in healed lesions also, but in contrast to the active phase, outer retinal hyperreflectivity in healed lesions originates from RPE proliferation and migration. Consequently, outer retinal hyperreflectivity in healed lesions is more granular and non-uniform. Retinal and RPE inflammation in active choroiditis is often associated with limited subretinal fluid overlying the area of choroiditis. Also, retinal thickness is normal or slightly increased in the active choroiditis phase, but in a healed lesion, it is mildly attenuated because of outer retinal atrophy.2
Choroid may also appear hyper-reflective on OCT. This increased choroidal reflectivity is described as a “waterfall effect” and is attributed to inflammatory cell infiltration of the Choroid. The choroidal hyperreflectivity in healed SC lesions is attributed to enhanced light transmission through overlying RPE atrophy.
Reema Bansal and et al in their prospective study of 3 patients during active and heald phase they observe eyes with active lesions of MSC in their patients illustrate the progressive changes in the outer retinal layers on OCT scans that correlated with the FAF changes.2 Acute lesions of MSC (diffusely hyperautofluorescent) corresponded to hyperreflective areas on SD-OCT involving RPE, POST, IS/OS, ELM, and ONL with a minimal distortion of inner retinal layers. There was no backscattering from inner choroid. During healing, lesions became discrete with a hypoautofluorescent border and predominant hyperautofluorescence centrally. The hyperreflective fuzzy areas on SD-OCT scans disappeared, and irregular, knobbly elevations of outer retinal layers appeared. The RPE, POST, IS/OS junction, and ELM could not be distinguished. The ONL appeared normal. The choroid showed an increased reflectance. As the lesions healed further over the next 3–6 months, they became predominantly hypoautofluorescent with loss of RPE, POST, IS/OS junction, and ELM in SD-OCT scan.2 Absence of any demonstrable changes in the inner choroid during the active stage of the lesion on OCT scans may suggest a primary involvement of the RPE and not the choroid in tubercular MSC lesions.2In our 8 patients during the course of MSC SD-OCT observation reveled the same observation of what Reema Basnal and et al observe with the addation of our observation of the vitreal, intraretinal and choroidal cells which has been seen in acute stage of the disease with absent cells during healing processes. This cells in SD-OCT observation of MSC conform the clinical finding of sever vitritis.7
Also our EDI-OCT observation demonstrated a diffuse choroidal thickening as well as localized changes in the deeper choroid beneath the active as well as healed lesions. This could suggest a choroidal involvement deeper to choriocapillaris. we believe that a diffuse increase in choroidal thickness may indicate an immunological trigger. The predominant and an early involvement of RPE may indicate the infective trigger which is go with Yeh et al who have hypothesized that RPE may be the site of primary insult and hence, more severely damaged in presumed tuberculosis-associated serpiginous-like choroidopathy based on the report of the isolation of mycobacterial DNA from RPE cells .11
Panagiotis Malamos et al in their correlation of fundus autofluorescence (FAF) with indocyanine green angiography (ICGA) in patients with various posterior uveitis disorders they found in 4 eyes of 4 pations of TB-serpigious like choroditis that Choriocapillaris and RBE are the Primary insult with predominat RPE involvement which is Similar evidence that has been recently reported by Gupta et al.12,13
Takahashi and associates used (EDI-OCT) to evaluate a 40-year-old woman with active, peripapillary SC with testing for known infectious causes of MSC was unrevealing in their study. They found that Prior to treatment subfoveal choroid was found to be markedly thickened (average713.3 ± 4.5 microns) and EDI-OCT localized the active peripapillary placoid lesions to just beneath the RPE, supporting published pathological studies showing diffuse choroidal inflammation with primary involvement of the choriocapillaris in areas of active placoid lesions in eyes with SC. Following treatment, subfoveal thickening decreased dramatically to 330 microns. This finding support the cilinical evidence that choroidal involvement is primary and the predominat insult in SC.12,13
The advantage of this study that all vitreoretinal layers, choroidal thickness vitreal and retinal cells infiltrate were observed during different stages of MSC by using SD-OCT and EDI-OCT. This observation can play a role into differention between infectious and non-infectous cause of serpiginous choroditis and give us a clue to start the patient on anti-tuberculosis treatment or no.
References
- 1.Schatz H, Maumenee A E, Patz A. (1974) Geographic helicoids peripapillary choroidopathy: clinical presentation and fluorescein angiographic findings. , Trans Am Acad Ophthalmol Otolaryngol 78, 747-761.
- 2.Nazari Hossein, Narsing A Rao. (2013) Serpiginous choroiditis and infectious multifocal serpiginoid choroiditis. , Surv Ophthalmol 58(3), 203-232.
- 3.Bansal Reema, Kulkarni Pandurang, Gupta Amod. (2011) High-resolution spectral domain optical coherence tomography and fundus autofluorescence correlation in tubercular serpiginouslike choroiditis. , J Ophthal Inflamm Infect 1, 157-163.
- 4.M J Gallagher, Yilmaz T, RA Cervantes-Castan eda. (2007) The characteristic features of optical coherence tomography in posterior uveitis. , Br J Ophthalmol 91, 1680-1685.
- 5.Delori F C, Dorey C K, Staurenghi G, Arend O, Goger D G.JJ Weiter.(1995).“In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium lipofuscin characteristics.”InvestigativeOphthalmology and Visual Science.36(3):. 718-729.
- 6.. Panagiotis Malamos,1 PanosMasaoutis,2 Ilias Georgalas,et al. The Role of Fundus Autofluorescence Imaging in the Study of the Course of Posterior Uveitis Disorders. BioMed Research International Volume 2015, Article ID 247469, 11 pages.
- 7.Emmett T Cunningham, Gupta Amod, Zierhut Manfred. (2014) The Creeping Choroiditides –Serpiginous and Multifocal Serpiginoid Choroiditis. Ocular Immunology & Inflammation. 22(5), 345-348.
- 8.Wu J S, Lewis H, Fine S L. (1989) Clinicopathologic findings in a patient with serpiginous choroiditis and treated choroidal neovascularization. , Retina 9, 292-301.
- 9.JDM Gass. (1987) Stereoscopic atlas of macular diseases: diagnosis and treatment, vol 1, 3rd edn. 136-144.
- 10.Rao N A, Saraswathy S, Smith R E. (2006) Tuberculous uveitis: distribution of Mycobacterium tuberculosis in the retinal pigment epithelium. , Arch Ophthalmol 124, 1777-1779.
- 11.Yeh S, Forooghian F.Wong WT et al (2010) Fundus autofluorescence imaging of the White Dot Syndromes. , Arch Ophthalmol 128, 46-56.
Cited by (1)
This article has been cited by 1 scholarly work according to:
Citing Articles:
Clinical ophthalmology (2021) OpenAlex Crossref Semantic Scholar