
Severe Vitamin D Deficiency in Saudi Patients with Type 2 Diabetes Mellitus
Abstract
Introduction
It has been demonstrated that vitamin D deficiency is associated with type 2 diabetes mellitus (T2DM). We conducted a cross sectional study to investigate the prevalence severe vitamin D deficiency in patients with T2DM.
Method
A cross-sectional single centre study was conducted in 4053 patients with T2DM. Patients with T2DM attended the Diabetes Centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia between January 2018 and December 2018 were recruited.
Results
There were 4053 patients with T2DM, 1145 male and 2908 female (28 % vs.72% respectively). The mean age was 53.9 ±16.5 years. The mean and median 25-OHD concentrations were 57.8±30.5 and 51.9 respectively. Severe vitamin D deficiency (25-OHD<25 nmol/l) was found in 1916 (9.5%). Moreover, severe vitamin D deficiency was not statistically significant more prevalent among females than males with male to female ratio 1:2.3 (70% vs. 30% respectively, p=0.6). In addition, severe vitamin D deficient patients were statistically significant younger than non-vitamin D deficient (48.0±16.7 vs. 54.6±16.3 respectively, p<0.0001). Severe vitamin D deficient patients have statistically significant higher HbA1c than non-vitamin D deficient (8.3 ±2.3 vs. 7.6±1.9 respectively, p<0.0001). The mean 25-OHD was upward as age advanced with highest frequency of vitamin D deficiency was found in the age group ≥60 years (27%) with males statistically significant most frequent than females in the age group ≥60 years (39 s, 22 respectively, p=0.003).
Regression analysis of odd ratio of risk factors for patients with severe vitamin D deficiency showed that age and HbA1c were statistically significant associated with vitamin D deficiency.
Conclusions
The prevalence of severe vitamin D deficiency in patients with T2DM is low and that more females with T2DM are affected with vitamin D deficiency than males.
Article Information
- Received
- Accepted
- Published
Academic Editor: Qianqian Song, Wake Forest School of Medicine, Wake Forest Baptist Comprehensive Cancer Center, Medical Center Boulevard, Winston-Salem, NC 27157, United States.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 K.S. Aljabri, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: K.S. Aljabri, Department of Endocrinology, King Fahad Armed Forces Hospital, Jeddah, Kingdom of Saudi Arabia, PO Box 9862. Jeddah 21159. Kingdom of Saudi Arabia —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
There is no any financial support or relationships that may pose conflict of interest.
Citation:
Introduction
Vitamin D deficiency remains a major health problem in many parts of the world.1 The main marker of vitamin D status is the metabolite 25-hydroxyvitamin D (25(OH)D), which is synthesized in the liver.1, 2 It is now increasingly recognized that vitamin D deficiency is defined as serum 25(OH)D concentration <50 nmol/L and a concentration <75 nmol/l are physiologically important, and probably indicate vitamin D insufficiency.3 Serum concentration of 25 (OH)D <25 nmol/l is widely accepted as indicative of severe deficiency. Studies confirmed that the prevalence of vitamin D deficiency in the general world population was as high as 50-80%.4 The Middle East region including Saudi Arabia has very high prevalence of vitamin D deficiency even in the normal asymptomatic population. 5, 6, 7
The prevalence of type 2 diabetes mellitus (T2DM) in Saudi Arabia is one of the highest reported in the world, reaching up to 30% in a recent study.8 It has been demonstrated that vitamin D deficiency was associated with T2DM.9, 10, 11, 12, 13, 14, 15, 16, 17 It has been reported that insulin secretion was dependent upon vitamin D and there was a positive correlation of vitamin D concentration with insulin sensitivity.18, 19, 20, 21, 22, 23 The prevalence of vitamin D deficiency in patients with T2DM varied from 70 to 90%, depending on the threshold used to define vitamin D deficiency.24, 25, 26Few published researches have found that surveyed the prevalence of severe vitamin D deficiency in patients with T2DM in Saudi Arabia. 27 We conducted a cross sectional study to investigate the prevalence severe vitamin D deficiency in patients with T2DM.
Methods
A cross-sectional single centre study was conducted in 4053 patients with T2DM. Patients with T2DM attending the Diabetes Centre at King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia between January 2018 and December 2018 were recruited. Eligible patients were 20 years or older. Exclusion criteria were known hepatic or renal disease, metabolic bone disease, malabsorption, hypercortisolism, malignancy, immobility for more than one-week, pregnancy, lactation, and medications influencing bone metabolism. The serum concentration of 25(OH)D was measured by competitive protein binding assay using kits (Immunodiagnostic, Bensheim, Germany). Severe vitamin D deficiency was defined as serum 25-OHD concentration < 25 nmol/L.1 Glycosylated hemoglobin (HbA1c) was measured by the high performance liquid chromatography method (Bio-Rad Laboratories, Waters, MA, USA). The total number of cohort were separated on basis of age values into five groups: 20-29 years, 30-40 years, 40-49 years, 50-59 years and ≥60 years. The study was approved by the ethical committee board of King Fahad Armed Forces Hospital.
Statistical Analysis
Data are presented as means ± standard deviation (SD) or numbers (%). Quantitative variables were compared between two groups by using the Student’s test. Differences in categorical variables were analysed using the chi-square test. The relationship between continuous variables was assessed using coefficients of correlation. Logistic regression analysis was carried out to identify the independent predictors of vitamin D deficiency considering age, gender and HbA1c as risk factors and to estimate odds ratio (OR) and 95% confidence interval (95% CI). P value <0.05 indicates significance. The statistical analysis was conducted with SPSS version 23.0 for Windows.
Results
There were 4053 patients with T2DM, 1145 male and 2908 female (28 % vs.72% respectively) (Table 1). The mean age was 53.9 ±16.5 years. The mean and median 25-OHD concentrations were 57.8±30.5 and 51.9 respectively. Severe vitamin D deficiency (25-OHD<25 nmol/l) was found in 1916 (9.5%) (Table 2). Moreover, severe vitamin D deficiency was not statistically significant more prevalent among females than males with male to female ratio 1:2.3 (70% vs. 30% respectively, p=0.6). In addition, severe vitamin D deficient patients were statistically significant younger than non-vitamin D deficient (48.0±16.7 vs. 54.6±16.3 respectively, p<0.0001). Severe vitamin D deficient patients have statistically significant higher HbA1c than non-vitamin D deficient (8.3 ±2.3 vs. 7.6±1.9 respectively, p<0.0001). As expected, the mean 25-OHD concentration was statistically significant lower in the vitamin D deficient patients compared to non-vitamin D deficient (20.2 ±3.8 vs. 61.7±29.4 respectively, p<0.0001).
Table 1. Patient characteristics mean ± standard deviation or number (%)| Variable | Values | Total | 4053 | |
| Age (years) | 53.9 ±16.5 | |||
| Gender | Male | 1145 ( 28.3 ) | ||
| Female | 2908 ( 71.7 ) | |||
| HbA1c (%) | 7.7 ±1.9 | |||
| 25-hydroxyvitamin D ( nmol/L ) | 57.8 ±30.5 | |||
| Variable | Severe vitamin D deficiency | P values | ||
| present | Absent | |||
| Numbers | 385 ( 9.5 ) | 3668 ( 90.5 ) | ||
| Age (years) | 48.0 ±16.7 | 54.6 ±16.3 | <0.0001 | |
| Gender | Male | 114 ( 29.6 ) | 1031 ( 28.1 ) | 0.6 |
| Female | 271 ( 70.4 ) | 2637 ( 71.9 ) | ||
| HbA1c (%) | 8.3 ±2.3 | 7.6 ±1.9 | <0.0001 | |
| 25-hydroxyvitamin D (nmol/L) | 20.2 ±3.8 | 61.7 ±29.4 | <0.0001 | |
The mean 25-OHD was upward as age advanced with highest frequency of vitamin D deficiency was found in the age group ≥60 years (27%) (Figure 1 A and B) with males statistically significant most frequent than females in the age group ≥60 years (39 s, 22 respectively, p=0.003) (Figure 2).
Figure 1. The mean of vitamin D concentration ( nmol/l ) (A) and the percentage of severe vitamin D deficiency (B) in correlation to age groups.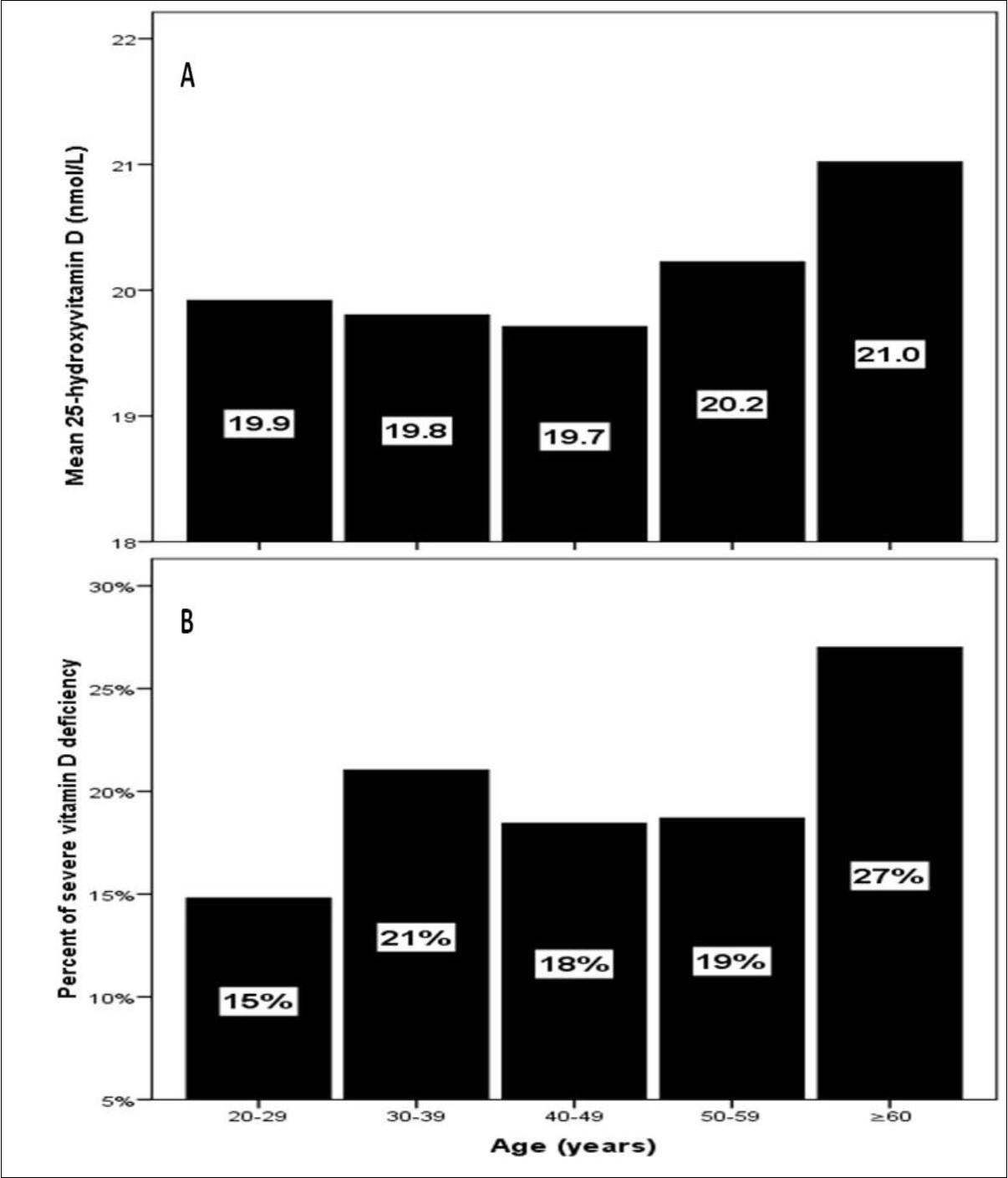
Download figure
Figure 2. The percentage of severe vitamin D deficiency according to gender in correlation to age groups.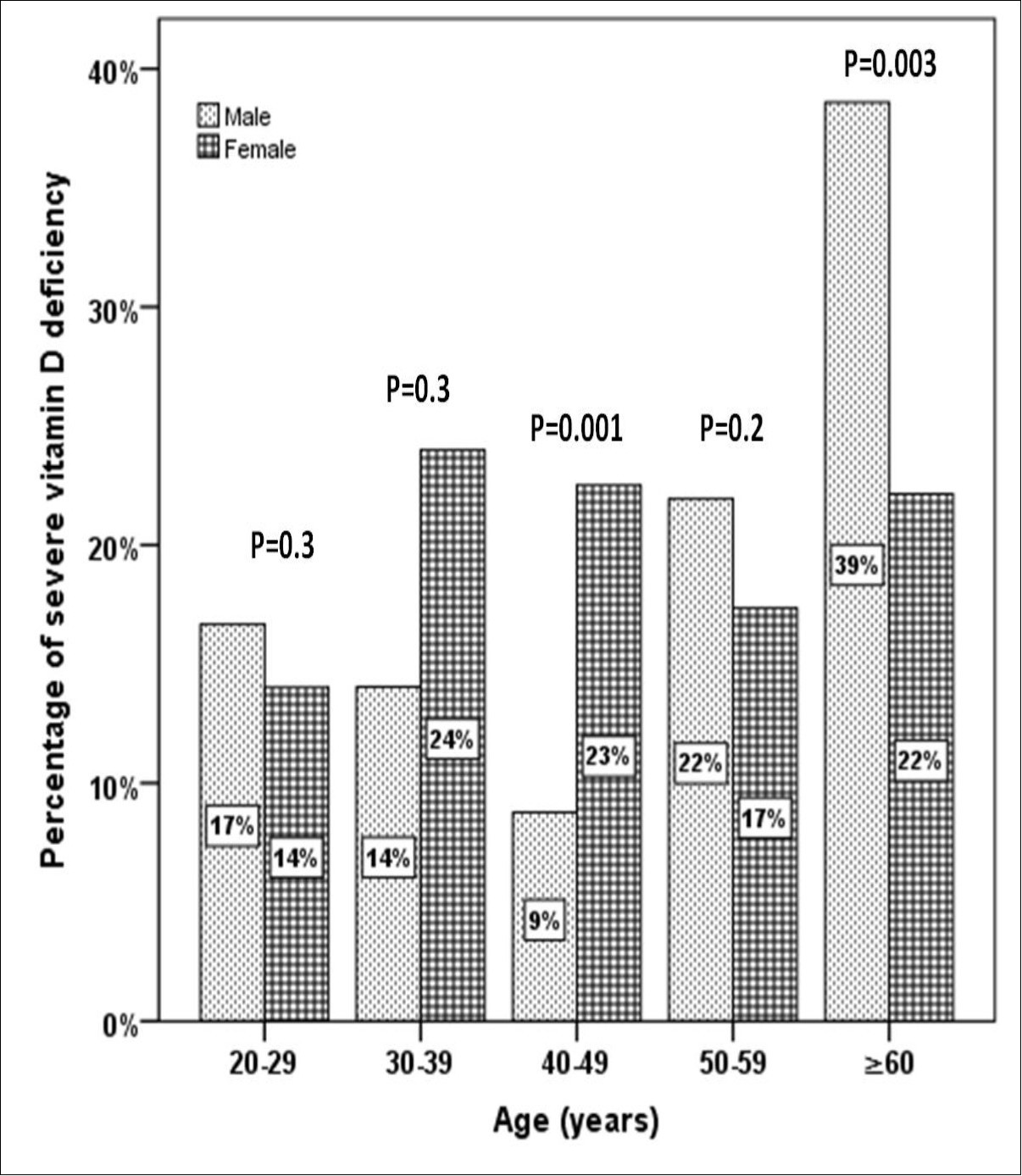
Download figure
25-OHD concentration was not significantly positively correlated with age (r=0.079, p=0.1) and not significantly negatively correlated with HbA1c (r= - 0.055, p=0.4) (Figure 3 A and B).
Figure 3. Correlation of 25-hydroxyvitamin D concentration and age (A) and HbA1c (B) in the study population
Download figure
Regression analysis of odd ratio of risk factors for patients with severe vitamin D deficiency showed that age and HbA1c were statistically significant associated with vitamin D deficiency, (OR=0.975; 95% CI=0.967,0.984), p<0.0001) and (OR=1.192;95% CI=1.118,1.271, p<0.0001) respectively (Table 3).
Table 3. Regression analysis for odd ratio of risk factors for patients with severe vitamin D deficiency| Parameters | Odd Ratio (95% CI) | P value | Age (years) | 0.975 (0.967-0.984) | <0.0001 |
| HbA1c | 1.192 (1.118-1.271) | <0.0001 |
Discussion
Our result confirmed the prevalence of severe vitamin D deficiency was 9.5% among the adult population and an even higher prevalence among older adults. It is of importance to state that the sample size is representative for a number of subjects suffering from T2DM in the area and study population of one institution does not represent the entire city of Jeddah, in addition the study sample confined to patients with T2DM but without comparable groups. The causes of vitamin D deficiency could be due to changing life style with people adopting a more sedentary life, little exposure to sunlight, reduced outdoor activity, changes in dietary habits. These factors also contributed to both development of T2DM and poor control of diabetes. Hashemipour et al. reported in Iran that the prevalence of severe vitamin D deficiencies was similar to our prevalence (9.5%) among the general population, aged 20-64 years.28 The prevalence of severe vitamin D deficiencies was 2% in Arizona, an area with high exposure to sun, using the same definition as we had used in this study. 29 In a study based on data from the National Health and Nutrition Examination Survey III (NHANES III) by Looker et al., the prevalence of severe vitamin D deficiency (25-OHD < 17.5 nmol/l) among adolescents and adult population of the United States was reported to be 1%.30 Prevalence of severe vitamin D deficiency (,25 nmol/l) was remarkably higher in one report from India (46·4 %) 31
Moreover, our findings showed that females were not significantly more likely to have severe vitamin D-deficient than males (OR=1.08). According to legislation, all females are required to wear a scarf and long-sleeve clothes. This is why they might have more severe vitamin D deficiency. Although other studies reported similar results in this field, however, seems that factors involved in vitamin D deficiency may be different more between males and females in some ethnic groups than others. 32, 33, 34
Vitamin D deficiency was reported as quite common in young and normal Saudi adults in 1981. 6 Back then however, vitamin D deficiency was more common among the elderly. In our study, the prevalence of severe vitamin D deficiency was much higher among the older age-group (27%), however, serum 25(OH)D was not statistically significant positively correlated with age r= 0.079 (p=0.1), in consistent with most studies whereas other studies reported the higher prevalence of vitamin D deficiency among the young people. 7, 35, 36, 37, 38, 39, 40, 41, 42 The positive correlation of 25(OH)D to age is in disagreement with a study carried out in the US, where severe vitamin D deficiency was found to be more common among the young, and less common among the elderly. 43 Recent studies have shown vitamin D deficiency among healthy young Saudi women of age 25 to 35 years was 30% and 55% in women of 50 years or more, indicating that it is common in young and postmenopausal women.7 In another study on male population from Saudi Arabia, the prevalence of vitamin D deficiency was found to between 28% and 37%.42
We found severevitamin D deficient patients have statistically significant higher HbA1c than non-vitamin D deficient (8.3±2.3 vs. 7.6±1.9 respectively), p<0.0001. Moreover, 25-OHD concentration was inversely not statistically significantcorrelated with HbA1c (r= - 0.055, p=0.4). These findings are supported by a number of international studies. In contrast some studies show no association of a low vitamin D with HbA1c levels.44 But inverse correlation between the level of vitamin D and glucose level is well known. 45, 46, 47 In many studies vitamin D levels were low in subjects having higher HbA1c values in patients with T2DM indicating that they are inversely related. 16, 25, 48 Vitamin D has various effects on glucose homeostasis. Besides its role in insulin secretion, it also has an influence on insulin resistance directly or via Ca indirectly. 21, 49 The results from the trials on the effect of vitamin D and/or Ca supplementation on insulin resistance have showed improvement on insulin action. 50
Growing scientific evidence has implicated vitamin D deficiency in a multitude of chronic conditions including T2DM. 40 With the growing prevalence of vitamin D deficiency across Saudi Arabia and its association with these leading causes of mortality, it has become more important than ever to delineate vitamin D’s role in the pathogenesis of these diseases and use data to pinpoint established risk factors for vitamin D deficiency. The relationship between vitamin D deficiency and diabetes has long been explored, with growing evidence suggesting vitamin D deficiency is a contributing factor to the development of T2DM. 41 We had several limitations, the study was done at one centre and was done at one point of time. The study sample confined to patients with T2DM but without comparable groups. In conclusion, we report severe vitamin D deficiency in Saudis with T2DM patients and that more females with T2DM are affected with vitamin D deficiency than males. Intervention studies are needed to clarify if supplementation of vitamin D leads to improvement in insulin sensitivity or glycemia in Saudis with T2DM patients.
References
- 1.Holick M F. (2006) High prevalence of vitamin D inadequacy and implications for health. Mayo Clin Proc. 81, 353-373.
- 2.Mathieu C, Badenhoop K. (2005) Vitamin D and Type 1 diabetes mellitus: state of the art. Trends in Endo and Met. 16, 261-267.
- 4.Gind A A, M C Liu, Camargo CA Jr. (2009) . Demographic differences and trends of vitamin D insufficiency in the US population,1988-2004. Arch Intern Med 169(6), 626-32.
- 5.Maalouf G, Gannage-Yared M H, Ezzedine J, Larijani B, Badawi S et al. (2007) Middle East and North Africa consensus on osteoporosis. , J Muskuloskelet Neuronal Interact 7, 131-143.
- 6.Sedrani S H, Elidrissy A W, El Arabi KM. (1983) Sunlight and vitamin D status in normal Saudi subjects. Am J Clin Nutr. 38, 129-132.
- 7.Al-Turki H A, Sadat-Ali M. (2008) Al-Elq AH, Al-Mulhim FA, Al-Ali AK. 25-Hydroxyvitamin D levels among healthy Saudi Arabian women. Saudi Med J. 29, 1765-1768.
- 8.Alqurashi K A, Aljabri K S, Bokhari S A. (2011) Prevalence of diabetes mellitus in a Saudi community. , Ann Saudi Med 31(1), 19-23.
- 9. (1999) study group. Vitamin D supplement in early childhood and risk for type 1 (insulin dependent) diabetes mellitus. , EURODIAB Substudy 2, 51-4.
- 10.Soltesz G, Patterson C C, Dahlquist G. (2007) EURODIAB Study group worldwide childhood type 1 diabetes incidence- what can we learn from epidemiology? Pediatr Diabetes. 8, 6-14.
- 11.Hypönen E, Läärä E, Reunanen A. (2001) Intake of vitamin D and risk of type 1 diabetes: a birth cohort study. , Lancet 358, 1500-3.
- 12.Zippitis C S, Akobeng A K. (2008) Vitamin D supplementation in early childhood and risk of type 1 diabetes: a sysytemetic review and meta-analysis. , Arch Dis Child 93, 512-7.
- 13.Matilla C, Knekt P, Mannisto S. (2007) Serum 25-hydroxyvitamin D concentration and subsequent risk of type 2 diabetes. , Diabetes Care 30, 2569-70.
- 14.Pittas A G, Dawson- Hughes B, Li T. (2006) Vitamin D and calcium intake in relation to type 2 diabetes in women. , Diabetes Care 29, 650-6.
- 15.Thorand B, Zierer A, Huth C. (2011) Effect of serum 25-hydroxyvitamin D on risk for type 2 diabetes may be partially mediated by subclinical inflammation: results from the MONICA/KORA Augsburg study. , Diabetes Care 34, 2320-2.
- 16.Cigolini M, Iagulli M P, Miconi V, Galiotto M, Lombardi S et al. (2006) Serum 25-hydroxyvitamin D3 concentrations and prevalence of cardiovascular disease among type 2 diabetic patients. , Diabetes Care 29, 722-4.
- 17.Scragg R, Holdaway I, Singh V, Metcalf P, Baker J et al. (1995) Serum 25-hydroxyvitamin D3 levels decreased in impaired glucose tolerance and diabetes mellitus. Diabetes Res Clin Pract. 27, 181-8.
- 18.Zeitz U, Weber K, Soegiarto D W, Wolf E, Balling R et al. (2003) Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. 17, 509-11.
- 19.Clark S A, Stumpf W E, Sar M. (1981) . Effect of 1,25 dihydroxyvitamin D3 on insulin secretion. Diabetes 30, 382-6.
- 20.Johnson J A, Grande J P, Roche P C, Kumar R. (1994) Immunohistochemical localization of the 1,25(OH)2D3 receptor and calbindin D28k in human and rat pancreas. , Am J Physiol 267, 356-60.
- 21.Maestro B, Campion J, Davila N, Calle C. (2000) Stimulation by 1, 25 dihydroxy vitamin D3 of insulin receptor expression and insulin responsiveness for glucose transport in U-937 human promonocytic cells. , Endocr J 47, 383-91.
- 22.Williams P F, Caterson I D, Cooney G J, Zilkens R R, Turtle J R. (1990) High affinity insulin binding and insulin receptor effector coupling: modulation by Ca2+. Cell Calcium. 11, 547-56.
- 23.Zemel M B. (1998) Nutritional and endocrine modulation of intracellular calcium: implications in obesity, insulin resistance and hypertension. , Mol Cell Biochem 188, 129-36.
- 24.Mori H, Okada Y, Tanaka Y. (2015) Incidence of vitamin D deficiency and its relevance to bone metabolism in Japanese postmenopausal women with type 2 diabetes mellitus. , Intern Med 54, 1599-04.
- 25.Tahrani A A, Ball A, Shepherd L, Rahim A, Jones A F et al. (2010) The prevalence of vitamin D abnormalities in South Asians with type 2 diabetes mellitus in the UK. , Int J Clin Pract 64(3), 351-5.
- 26.Miñambres I, Sánchez-Quesada J L, Vinagre I, Sánchez- Hernández J, Urgell E et al. (2014) Hypovitaminosis D in type 2 diabetes: relation with features of the metabolic syndrome and glycemic control. Endocr Res. 40(3), 160-5.
- 27.Al-Zaharani M. (2013) The prevalence of Vitamin D deficiency in Type 2 Diabetic patients. , Majmaah J. HEALTH SCIENCES 1(1), 18-22.
- 28.Adibi H. (2004) Vitamin D deficiency and causative factors in population of Tehran. , BMC Public Health 4, 38.
- 29.Jacobs E T, Alberts D S, Foote J A, Green S B, Hollis B W et al. (2008) Vitamin D insufficiency in southern Arizona. , Am J Clin Nutr 87, 608-13.
- 30.30 Looker AC, Dawson-Hughes B, Calvo M S, Gunter E W, Sahyoun N R. (2002) Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. , Bone 30, 771-7.
- 31.Tiwari Shalbha, Pratyush D, Daliparthy, Gupta Balram, Dwivedi Awanindra et al. (2012) Prevalence and severity of vitamin D deficiency in patients with diabetic foot infection. The British journal of nutrition. 109, 1-4.
- 32.el-Sonbaty M R, Abdul-Ghaffar N U. (1996) Vitamin D deficiency in veiled Kuwaiti women. , Eur J Clin Nutr 50, 315-18.
- 33.Meddeb N, Sahli H, Chahed M, Abdelmoula J, Feki M et al. (2005) Vitamin D deficiency in Tunisia. , Osteoporos Int 16, 180-3.
- 34.Guzel R, Kozanoglu E, Guler-Uysal F, Soyupak S, Sarpel T. (2001) Vitamin D status and bone mineral density of veiled and unveiled Turkish women. , J Womens Health Gend Based Med 10, 765-70.
- 35.Omdahl J L, Garry P J, Hunsaker L A, Hunt W C, Goodwin J S. (1982) Nutritional status in a healthy elderly population: vitamin D. , Am J Clin Nutr 36, 1225-32.
- 36.Kinyamu H K, Gallagher J C, Balhorn K E, PetranicK K M, Rafferty K A. (1997) Serum vitamin D metabolites and calcium absorption in normal young and elderly free-living women and in women living in nursing homes. , Am J Clin Nutr 65, 790-7.
- 37.Burnard B, Sloutskis D, Gianoli F, Cornuz J, Rickenbach M et al. (1992) Serum 25-hydroxyvitamin D: distribution and determinants in the Swiss population. , Am J Clin Nutr 56, 537-42.
- 38.Lips P. (2001) Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone wloss and fractures and therapeutic implications. , Endocr Rev 22, 477-501.
- 39.Hovsepian Silva, Amini Massoud, Aminorroaya Ashraf, Amini Peyvand, Iraj Bijan. (2011) . , Prevalence of Vitamin D Deficiency among Adult Population of Isfahan City, Iran. J HEALTH POPUL NUTR 29(2), 149-155.
- 42.Sadat-Ali M, Al-Elq A M, Al-Turki H. (2009) Vitamin D levels among Healthy Saudi Arabian Men. Annals of Saudi Med. 29, 378-82.
- 43.Plotnikoff G A, Quigley J M. (2003) Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 78, 1463-1470.
- 44.LLN Husemoen, Thuesen B H, Fenger M, Jorgensen T, Glumer C et al. (2012) . Serum 25 (OH)D and Type 2 Diabetes Association in a General Population:A prospective study. Diabetes Care 35(8), 1695-700.
- 45.Palomer X, Gonzalez-Clemente J, Blanco-Vaca F, Mauricio D. (2008) Role ofvitamin D in the pathogenesis of type 2 diabetes mellitus. , Diabetes 10(3), 185-97.
- 46.Boucher B J, Mannan N, Noonan K, Hales C N, Evans S J. (1995) Glucose intoleranceand impairment of insulin secretion in relation to vitamin D deficiency in eastLondonAsians. , Diabetologia 38(10), 1239-45.
- 47.Hutchinson M S, Figenshau Y, Schirmer H NjølstadI, Jorde R. (2011) Serum25-hydroxyvitamin D levels are inversely associated with glycatedhaemoglobin (HbA(1c)).The TromsøStudy. , Scand J Clin Lab Invest 71(5), 399-406.
- 48.Kositsawat J, Freeman V L, Gerber B S, Geraci S. (2010) Association of A1Clevels with vitamin D status in U.S. adults: data from the National Health and Nutrition Examination Survey. Diabetes Care. 33(6), 1236-8.
Cited by (1)
This article has been cited by 1 scholarly work according to:
Citing Articles:
Diabetes Metabolic Syndrome and Obesity (2024) OpenAlex Semantic Scholar Crossref