
Abstract
Objectives
This study was designed to assess the demographic characteristics, prevalence of metabolic syndrome (MetSy) among patients with schizophrenia in Saudi Arabia.
Methods
This is a disease-oriented and observational study. Schizophrenia was defined by DSM-IV criteria. MetSy were assessed based on the international criteria (NCEP-ATP III and AHA/NHLB).
Results
90% of the participants are without a university degree and 56.4% are single. Chronic and acute cases of schizophrenia were 95% and 5%, respectively. The treatment of schizophrenia was combination therapy and monotherapy with percentages of 56% and 44%, respectively. Systolic and diastolic blood pressures were 121.92±11.07 mmHg and 77.29±0.45 mmHg, respectively. Surprisingly, all patients have abnormal HDL. A mean waist circumference of 90.23±14.88 cm for men, and 93.38±15.28 cm for women. The analysis of 101 patients showed a prevalence of the MetSy is 15.8%. Chi-square test of independence showed lack of independency of MetSy on type of therapy. Modeling of MetSy and risk factors was also conducted.
Conclusion
The metabolic syndrome is greatly established among schizophrenic patients. It signifies a vital hazard for metabolic and cardiovascular ailments. Evaluation of the incidence and examining of the related threats of the metabolic syndrome should be an element of the clinical managing of patients cured with antipsychotics.
Author Contributions
Academic Editor: Pushpendra kumar, Department of Chemistry, Lovely Professional University, Phagwara, Punjab, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright 2019 Rashad Mohamed Alsanosy.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors declare that they have no competing of interests.
Citation:
Introduction
Schizophrenia is a mental illness that influences about one percent worldwide. Schizophrenic patients have shorter life span as balanced to their healthy associates 1,2. Mortality and morbidity among patients with schizophrenia has been related to high occurrence of cardiovascular diseases and metabolic syndrome (MetSy)3,4. Olanzapine, amisulpride, quetiapine, risperidone, clozapine are the most frequently used anti-schizophrenic drugs in Saudi Arabia (KSA) with no previous research reported to evaluate their side effects5. Weight gain, obesity, increased risk for dyslipidemia, accelerated cardiovascular ailment, diabetes, and premature fatality have been connected to drugs in this group as well. Previous research showed that Saudi patients on antipsychotic medications acquire numerous risk factors. The need for detailed studies on these issues is supported by a metabolically unwanted postnatal and gestational environment, which is common in the KSA, adjoins to the receptivity of the previously genetically predisposed people to a lifetime of insulin resistance. Moreover, the prevalence of ordinary risk factors for diabetes mellitus type 2, such as the full MetSy and its individual indicators and criteria, has been documented in Saudi adults, 37% of whom have the full MetSy6,7,8. Literature survey is indicative of an urgent demographical study and epidemiological assessment to determine individuals affected with schizophrenia, this will appendage the ways to create strategy to address different issues pertaining to structural alterations in health care services provided to the mentally ill patients in KSA. 22.4% of Saudi patients reporting to services for mental disorders are suffering from schizophrenia 9,10,11.
Earlier studies were only highlighted on the incidence of mental sickness without attempt to examine the characteristics of schizophrenia 12,13. Nevertheless, a few studies have revealed that amongst all the psychoactive drugs, antipsychotics were intensely used and the promptness was noticed to be considerably increased in the case of inpatients balanced with out-patients14,15. Side effects of antipsychotic medications in KSA have been reported16 with, no specific research conducted on the prevalence of MetSy on schizophrenic patients using antipsychotic medications. Therefore, the current study was designed to assess the demographic characteristics, prevalence of MetSy and metabolic abnormalities among Saudi schizophrenic patients. Correlation between MetSy and risk factors among schizophrenic patients was examined as well.
Methods
Research Design, Selection Criteria and Sample Size Determination
This is disease-oriented and observational study was conducted in Saudi Arabia from August 2016 until December 2016. All patients attending Jazan Psychiatric Hospital Center during the course of the study with the next criteria were requested to contribute: 1) their age should be above 16 years old, and 2) they were recognized with schizophrenia as stated by DSM-IV criteria17. In order to evaluate with sufficient accuracy the prevalence of MetSy, we used 22.4% as a previous prevalence of MetSy for sample size calculation (99% confidence interval ±10%). A sample size of at least 100 patients was recruited. On the measurement day, demography and clinical data were collected. The following types of information were collected: age, gender, marital status, occupation, admissions history, length of psychiatric illness, antipsychotic medications; waist circumference (WC), weight and height, fasting plasma glucose (FPG) measured in mg/dL, and lipid profile.
Quality Control
Focus group discussions were conducted to preserve consistency and rationality of the research data acquiring process. Evaluations were done regularly during the study to recognize any troubles in data collection, the elucidation of variables, and the application of study guidelines. Before starting data analysis, a wide sequence of checks was done for data uniformity, suitable sequences of data, and an assessment of incomplete or missing data. The questionnaire was modified by the principal researchers and the customized version was checked by experts to guarantee construct and content validity. Data from the pre-test assessment was not incorporated in the final analysis.
Ethical Approval
Approval to conduct the study was obtained from Standing Committee for Biomedical Research Ethics (SCBRE) at Jazan University (Approval No. 37/60/37532). A written consent was obtained to use the medical records according to the local regulations. Metabolic screening and blood tests for schizophrenia patients were considered standard of care in schizophrenia treatment in Psychiatry and Mental Health Centers according to European and American Standards18,19. Therefore, the ethical committee approved that obtaining blood samples did not hinder as this observational study. Medical cases such as schizophrenia in themselves were no longer referred to be an obstacle to individual permission or research contribution. If the consent is going to be obtain from a proxy, the consent of the participant is still always necessary18.
The Antipsychotic Use Patterns
The types and dosages of antipsychotic medications were obtained. The number of antipsychotics used was classified as monotherapy, presently using only one type of antipsychotic medication, and combination, presently taking more than one type of antipsychotic. Medical data concerning the period of current antipsychotic treatment or preceding antipsychotic treatment was not attained due to restrictions related to information in their documents.
Waist Circumference, Weight and Height
Waist circumference (WC) was obtained by a stretched tape-meter, without any force to the body exterior, and was recorded to the closest 0.1 cm. The waist measurement was obtained with the tape-meter in a horizontal plane, midway between the inferior margin of the ribs and the superior border of the iliac crest20. To avoid inter-researcher inaccuracy, all measurements were obtained by the same person. We utilized a portable spring balance to measure weight. The scale was obtained to zero before weighing. The weight is recorded to nearest 0.1Kg. Height is the distance from the crown of the head to the soles of the feet. The subject stood erect and bare foot on stadiometer with movable head piece was leveled with skull vault and height was recorded to nearest 0.1cm.
Blood Pressure
Blood pressure (BP) was measured in a sitting position. Two measurements were taken made by two independent medical officers in the right arm after the participant sat and rested for at least 5 min. In case of difference in BP reading, a third one was obtained out and the arithmetic mean was calculated.
Fasting Blood Pressure
For fasting plasma glucose (FPG), blood samples were obtained from all fasted participants in the morning while they were in a sitting position according to the standard protocol. Blood was obtained from an antecubital vessel punctures. Blood samples were centrifuged within 30 to 45 minutes of collection. Glucose in plasma was measured using Chemistry Auto-analyzer.
Biochemical Analysis
Fasting plasma samples were used to conduct biochemical analysis. Lipid profile was performed at Jazan Psychiatric Hospital laboratory on the day of blood collection. For lipid measurement, LDL-C, HDL-C, TC, and TG were measured using commercially available kit. The MS was defined according to ATPIII and NCEP definitions as shown in Table 121.
Table 1. Definitions and reference ranges for metabolic syndrome according to NCEP-ATP III and AHA/NHLB| Risk factor | Defining measure NCEP | ATP III Defining measure AHA/NHLB |
| Abdominal obesity(waist circumference) | ||
| Men | > 102 cm | ≥102 cm |
| Women | > 88 cm | ≥88 cm |
| Triglycerides | ≥ 150 mg/dL | ≥ 150 mg/dL or on drug treatment for elevated triglycerides |
| High density lipoprotein (HDL) | ||
| Men | < 40 mg/dL | < 40 mg/dL or on drug treatment for reduced HDL-cholesterol |
| Women | < 50 mg/dL | < 50 mg/dL or on drug treatment for reduced HDL-cholesterol |
| Blood pressure | Systolic ≥ 130 or diastolic ≥ 85 mmHg | Systolic ≥ 130 or diastolic ≥ 85 mmHg or on antihypertensive medication |
| Fasting glucose | ≥ 110 mg/dL | ≥ 100 mg/dL or on antidiabetic medication |
Statistical Analysis
Descriptive statistics included frequencies and percentages were calculated for all categorical variables. Means and standard deviations were obtained for all continuous variables. Inferential statistics including t-test and Chi-square test were performed for mean differences and association, respectively. Risk factors for MetSy were analyzed using logistic regression. The presence of MetSy was used as the dependent categorical variable. SPSS for Windows was used to analyze the data. The conventional 5 percent significance level was used throughout the study.
Results
The current study includes 101 schizophrenic patients recruited according to meet the diagnostic criteria defined by DSM-IV. 90% of the participants are without a university degree and 56.4% are single. The age ranged between 18 and 69 years, with upper and lower quartiles of 38 and 42 years, respectively. Women had a mean age of 38.69±14.89 years, for men it was 40.98±11.13 years. For details on demographics, see Table 2. Chronic and acute cases of schizophrenia were 95% and 5%, respectively Table 3. The mean time since first diagnosis was 12.70±8.77 years, ranging from 2 to 38 years. 59.4% of the patients were admitted to the hospital at least a once during the last 12 months with average of 12 days per admission. Adherence to the treatment of schizophrenia is shown in Table 3, whereby, 72.4% of the studied sample was partially adhered to the treatment. And the treatment of schizophrenia was combination therapy and monotherapy with percentages of 56% and 44%, respectively. As shown in Table 4, 25% of the sample uses valporate as a concurrent non-antipyschotic medication. It is also observed that 50.5% of patients are using combined medications, while resperidone, haloperidol and olanzapine were used by 17.8%, 9.9% and 8.9%, respectively, of sample.
Table 2. Demography of the study sample| Variable | Frequency | Percentage |
| Nationality | ||
| Saudi | 98 | 97.0 |
| Non-Saudi | 3 | 3.0 |
| Gender | ||
| Male | 88 | 87.1 |
| Female | 13 | 12.9 |
| Marital status | ||
| Single | 57 | 56.4 |
| Married | 30 | 29.7 |
| Divorced | 14 | 13.9 |
| Educational level | ||
| Illiterate | 28 | 27.7 |
| Primary | 20 | 19.8 |
| Intermediate | 21 | 20.8 |
| Secondary | 26 | 25.7 |
| University degree | 6 | 5.9 |
| Financial situation | ||
| High | 1 | 1.0 |
| Normal | 34 | 33.7 |
| Poor | 64 | 63.4 |
| None | 2 | 2.0 |
| Occupation | ||
| Government employee | 4 | 4.0 |
| Free businees | 1 | 1.0 |
| House wife | 2 | 2.0 |
| Retired | 22 | 21.8 |
| Unemployed able to work | 29 | 28.7 |
| Unemployed unable to work | 43 | 42.6 |
| Classification of housing type | ||
| Rural | 64 | 63.4 |
| Urban | 37 | 36.6 |
| Accommodation type | ||
| Residence | 60 | 60.0 |
| Rent | 28 | 28.0 |
| Private House | 12 | 12.0 |
| Age (years) | ||
| (Mean±SD) | 40.68±11.62 | |
| Upper and lower quartiles | 38 and 42 | |
| Number of family members(Mean±SD) | 7.83±3.39 | |
| Frequency | Percentage | |
| Status | ||
| Chronic disease | 96 | 95.0 |
| Acute disease | 5 | 5.0 |
| Treatment adherence | ||
| Consistently adhered | 25 | 25.5 |
| No adherence treatment | 2 | 2.0 |
| Partially adhered | 71 | 72.4 |
| Hospital admission (Last 12 months), days | ||
| 1 | 60 | 59.4 |
| 2 | 29 | 28.7 |
| 3 | 10 | 9.9 |
| 4 | 1 | 1.0 |
| 5 | 1 | 1.0 |
| Days admitted (Last 12 months) | 12.70±8.77 | |
| Duration since initial diagnosis | 106.51±119.41 | |
| Type of therapy | ||
| Monotherapy | 44 | 44.0 |
| Combination therapy | 56 | 56.0 |
| Frequency | Percentage | |
| Non-antipsychotic drugs | ||
| Valporate | 25 | 25.0 |
| Benzotropine | 13 | 13.0 |
| Benzhexol | 1 | 1.0 |
| Valporate+Benzhexol | 1 | 1.0 |
| None | 60 | 60 |
| Antipsychotic | ||
| Olanzapine | 9 | 8.9 |
| Resperidone | 18 | 17.8 |
| Quetiapine | 2 | 2.0 |
| Amisulpiride | 5 | 5.0 |
| Haloperidol | 10 | 9.9 |
| Aripirazole | 3 | 3.0 |
| Trifluperazine | 2 | 2.0 |
| Paliperidone | 1 | 1.0 |
| Combined medications | 51 | 50.5 |
Measurements of metabolic syndrome indicators according to the guidelines (Table 1) are depicted in Table 5. Systolic and diastolic blood pressures were 121.92±11.07 mmHg and 77.29±.45 mmHg, respectively. Surprisingly, all patients have abnormal HDL with an average of 18.63±5.23. A mean waist circumference of 90.23 ± 14.88 cm for men, and 93.38 ± 15.28 cm for women indicated overweight in a considerable proportion of the patients. Anthropometric parameters of weight and height are shown in Table 5. As shown in Figure 1, the prevalence of metabolic syndrome among schizophrenic patients as defined by the Adult Treatment Panel (ATP) III in 2001 is 15.8%.
Table 5. Measurements of metabolic syndrome indicators according to the guidelines| Mean | SD | Normal (n,%) | Abnormal (n,%) | |
| Systolic Blood Pressure | 121.92 | 11.07 | 87(86.1) | 14(13.9) |
| Diastolic Blood Pressure | 77.29 | 6.45 | 92(91.1) | 9(8.9) |
| Triglycerides (mg/dl) | 26.56 | 16.44 | 74 (73.3) | 27(26.7) |
| HDL-C (mg/dl) | 18.63 | 5.23 | 100 (100) | 0(0) |
| LDL (mg/dl) | 45.14 | 17.30 | ||
| Waist Circumference | 90.61 | 14.89 | 74(73.3) | 27(26.7) |
| Fasting Blood Glucose FBG (mg/dl) | 91.53 | 29.95 | 81(80.2) | 20(19.8) |
| BMI (kg/m2) | 61.02 | 3.04 | ||
| Height (cm) | 164.25 | 7.94 | ||
| Weight (kg) | 69.31 | 17.09 |
Figure 1.Prevalence of metabolic syndrome among schizophrenic patients as defined by the Adult Treatment Panel (ATP) III in 2001 21.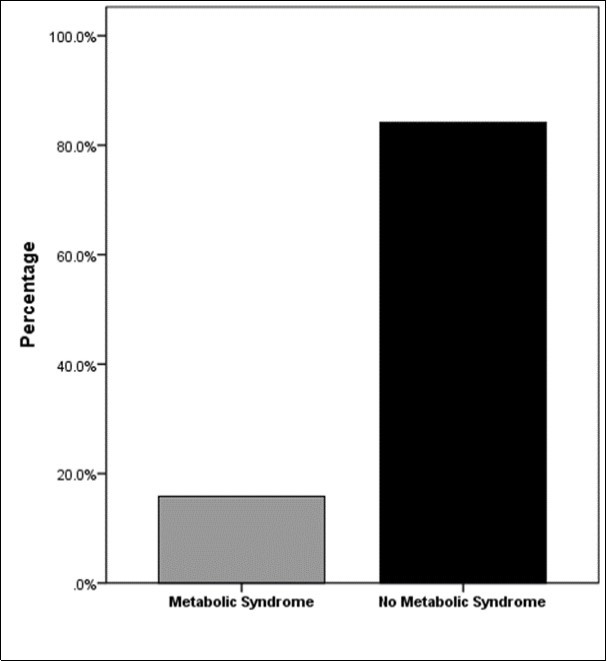
This study included metabolic syndrome (16 metabolic syndrome and 84 non-metabolic syndrome) and type of therapy (44 monotherapy and 56 combination the). A 2X2 chi-square test of independence was used to determine if metabolic syndrome is dependent on type of therapy. Given α = 0.05, the results suggest lack of dependency, χ2 (1, N = 101) = 0.278, p = 0.598. The results also show that metabolic syndrome is independent of the participants gender (P>0.05). The mean age for metabolic syndrome (n = 16) and no metabloic syndrome (n = 85) was statistically compared using a two-tailed independent sample t-test at α = 0.05. The results suggest that average metabolic syndrome scores (M = 48.63, SD = 11.212) are significantly greater than average no metabloic syndrome scores (M = 39.19, SD = 11.135), t(99) = 3.107, p = 0.002. Logistic regression model findings are shown in Table 6. Varaibles included in the model were gender, age, residence, accommodation type, number of family members and duration. Odd ratios for all variables are shown in Table 6 with their upper and lower confidence intervals. OR considered statistically significant if the intervals don’t enclose the value of 1. In the current study, only age and duration are the significant factors with the values of 0.855 and 1.121, respectively. At 0.05 level of significance, only age and duration of the disease have contributed significantly in the development of MetSy.
Table 6. logistic regression model| Variables | B-coefficient | P-value | OR | 95% C.I. for OR | |
| Lower | Upper | ||||
| Gender | |||||
| Male | 1.468 | 0.106 | 4.340 | 0.734 | 25.681 |
| Female (reference) | |||||
| Age* | -0.157 | 0.001* | 0.855 | 0.782 | 0.935 |
| Marital status | 0.999 | ||||
| Divorced(reference) | |||||
| Single | -0.035 | 0.975 | 0.966 | 0.114 | 8.160 |
| Married | -0.003 | 0.998 | 0.997 | 0.112 | 8.886 |
| Residence | 0.945 | ||||
| Urban (reference) | |||||
| Rural | 0.049 | 0.954 | 1.051 | 0.197 | 5.615 |
| Accommodation type | 0.249 | ||||
| Private House (reference) | |||||
| Residence | -2.203 | 0.131 | 0.110 | 0.006 | 1.922 |
| Rent | -3.123 | 0.098 | 0.044 | 0.001 | 1.784 |
| Number of Family members | 0.029 | 0.805 | 1.030 | 0.815 | 1.301 |
| Duration* | 0.114 | 0.017* | 1.121 | 1.021 | 1.231 |
| Constant | 29.067 | 0.999 | 420 | ||
Discussion
The current study was designed to assess the demographic characteristics, prevalence of MetSy and metabolic abnormalities among Saudi schizophrenic patients. Correlation between MetSy and risk factors among schizophrenic patients was examined as well. Side effects of antipsychotic medications in KSA have been reported and were found to be associated with numerous risk factors, such as overweight, dyslipidemia, obesity and smoking16,21,22,23. However, no specific research was conducted on the prevalence of MetSy on schizophrenic patients undergoing antipsychotic medications. A recent study noticed that patients on antipsychotic drugs in Saudi Arabia possess numerous risk factors14. Prevalence of MetSy among patients with various psychiatric diagnoses and treatments were also reported with no an in-depth emphasis on schizophrenic patients and that study also did not consider Jazan region [24]. Whereby, our study only focuses in Jazan region.
Amisulpride, olanzapine, risperidone, clozapine, quetiapine are the most commonly used anti-schizophrenic medications in KSA with no previous studies reported to assess their unwanted side effects specially on schizophrenic patients5,24. The need for detailed research on this matter is compounded by a metabolically undesirable postnatal and gestational environment, which is widespread in the KSA, adjoins to the receptiveness of the already genetically predisposed person to a lifetime of insulin resistance and associated morbidities25. More, the prevalence of conventional risk factors for diabetes mellitus type 2, such as the full metabolic syndrome (MetSy) and its individual symptoms and criteria, have been reported in adult Saudis, 37% of whom have the full MetSy, while just recently partial MetSy21,26. The published literature survey is suggestive of an urgent demographical analysis and epidemiological survey to ascertain number of individuals affected with schizophrenia, this will paw the ways to formulate strategy to address various issues pertaining to structural adjustments in health care services provided to the mentally ill patients in KSA.
The prevalence (15.8%) of MetSy among schizophrenic patients in our study is lower than that reported in other studies with Asians including reports from Thailand (22.8%), Taiwan (34.9% and 23.8%), Japan (27.5%), and Korea (31.7%) and was more comparable to the rates reported from western countries. The current study used NCEP and ATP III criteria which considered abdominal obesity (waist circumference) to be more than 88cm, whereby these countries used a lower criterion (≥80 cm) of abdominal obesity than we did (≥88 cm). Previous studies on MetSy obtained in the Arabian world are not many. A study carried in 63 Egyptian schizophrenic patients to investigate the risk factors of MetSy using the IDF criteria found that twenty four schizophrenic patients (38.09%) met the criteria for MetSy27. Another research conducted using 220 UAE psychiatric inpatients found that the prevalence of MetSy was about 48.1% 28. To get also more comparable results; we can consider a Palestine study which recruited 250 patients with schizophrenia. The MetSy prevalence was assessed based on Adult Treatment Panel III Adapted criteria. The overall MetSy prevalence among patients with schizophenia in Palestine was 43.6% 29. Current studies on MetSy in the general population have certainly supplied substantiation for the expansion of ethnic-/race-specific criteria. Even though there is a substantial discrepancy in criteria and methodology among published studies, the MetSy prevalence in our study was within the range of prior reports published regionally and worldwide. It is difficult to identify the reasons for this discrepancy because many factors affect the development of MetSy, including medication, age, gender, definition of MetSy, and lifestyle. However, one of the important causes may be the trend for an increase in obesity and MetSy during the past two decades in the Saudi healthy population. A community-based study (n=17,293) has reported that the overall age-adjusted prevalence of Metsy in Saudi subjects is 39.3%.25. Another study conducted using total of 4578 Saudis aged 15-64 selected from 20 regions in Saudi Arabia showed the prevalence of 28.3% 21.
Predisposing and risk factors for MetSy of the Saudi population are a warranting feature of schizophrenic patients21,22,30. Our current study revealed new findings on the prevalence of MetSy and its associated risk factors among schizophrenic patients. The present findings may highlight the serious need for metabolic screening and supervision particularly among older patients with chronic schizophrenia. Further future studies are required to corroborate the current results and assess different preventive initiatives to address metabolic disturbances in the population with schizophrenia.
Acknowledgements
This research was funded by Deanship of Scientific Research, Jazan University, Saudi Arabia (SABIC#2 Project No: 1667).
References
- 1.Nakazawa K. (2012) et al.,GABAergic interneuron origin of schizophrenia pathophysiology.Neuropharmacology. 62(3), 1574-1583.
- 2.G D Pearlson, Etiologic phenomenologic. (2015) and endophenotypic overlap of schizophrenia and bipolar disorder.Annual review of clinical psychology. 11, 251-281.
- 3.A J Mitchell. (2013) et al.,Prevalence of metabolic syndrome and metabolic abnormalities in schizophrenia and related disorders—a systematic review and meta-analysis.Schizophrenia bulletin. 39(2), 306-318.
- 4.Roshanaei-Moghaddam Babak, M, W. (2015) Katon,Premature mortality from general medical illnesses among persons with bipolar disorder: a review.Psychiatric services.
- 5.R M Alsanosy.(2017).The Role of Antipsychotic Medications in Metabolic Syndrome Amongst a Predisposed Population: Review of The Saudi Case.Journal of Metabolic Syndrome. 6(1), 1000223.
- 8.Al-Nozha M M.(2004).Coronary artery disease. in Saudi Arabia.Saudi medical journal 25(9), 1165-1171.
- 9.Al-Subaie A S.(1996).Psychiatric emergencies in a university hospital in Riyadh. , Saudi Arabia.International Journal of Mental Health 25(4), 59-68.
- 10.Sharaheeli J, Alswaidi F. (2015) Mandil,Characteristics of Mental Illnesses among Psychiatric Patients Admitted to theAlamalComplex for Mental Health in Riyadh, Saudi Arabia in 2013.Journal of Psychiatry.
- 11.Sharaheeli J, Nooh R, Medical. (2016) Illnesses among Chronic Psychiatric Inpatients inTaifMental Hospital,Taif, Saudi Arabia.J Psychiatry. 19(375), 2.
- 12.Rasic D. (2013) et al.,Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: a meta-analysis of family high-risk studies.Schizophrenia bulletin. 40(1), 28-38.
- 14.F D Alosaimi.(2016).Patterns of psychotropic medication use in inpatient and outpatient psychiatric settings insaudiarabia.Neuropsychiatric disease and treatment. 12, 897.
- 15.Alshowkan A, Curtis J, Y. (2015) White,Factors affecting the quality of life for people with schizophrenia in Saudi Arabia: a qualitative study.Journal of Psychiatry.
- 16.Dossenbach M.(2006).Effects of atypical and typical antipsychotic treatments on sexual function in patients with schizophrenia:. 12-month results from the Intercontinental Schizophrenia Outpatient Health Outcomes (IC-SOHO) study.European Psychiatry 21(4), 251-258.
- 17.Tandon R.(2013).Definition and description of schizophrenia. in the DSM-5.Schizophrenia research 150(1), 3-10.
- 18.Kraemer S.(2011).Prevalence of metabolic syndrome in patients with schizophrenia, and metabolic changes after 3 months of treatment with antipsychotics - results from a German observational study.BMC psychiatry. 11(1), 173.
- 19.S M Grundy.. (2005).Diagnosis and Management of the Metabolic Syndrome.An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement 112(17), 2735-2752.
- 20.P J Akholkar, A, M C. (2017) Shah,The metabolic syndrome among hypertensive patients: a cross-sectional study.International. , Journal of Advances in Medicine 2(3), 188-191.
- 23.Al-Nozha M M.(2007).Prevalence of physical activity and inactivity among Saudis aged 30-70 years: a population-based cross-sectional study.Saudi Med. , J 28.
- 24.F D Alosaimi.(2017).Prevalence of metabolic syndrome and its components among patients with various psychiatric diagnoses and treatments: A cross-sectional study.General Hospital Psychiatry, 45(Supplement C):. 62-69.
- 25.Brocato J.(2014).Particulate matter from Saudi Arabia induces genes involved in inflammation, metabolic syndrome and atherosclerosis.Journal of Toxicology and Environmental Health. , Part A 77(13), 751-766.
- 26.D A Al-Qahtani.Imtiaz M.L. (2005).Prevalence of metabolic syndrome. in Saudi adult soldiers.Saudi medical journal 26(9), 1360-1366.
- 27.Hatata H.(2009).Risk factors of metabolic syndrome among Egyptian patients with schizophrenia.Curr. , Psychiatry 16, 85-95.
- 28.Shahda M, A. (2010) El-Sayed,Study of the prevalence of metabolic syndrome among psychiatric patients and its correlation with diagnosis and medications.Egyptian. , Journal of Psychiatry (Print) 31, 2.