
Influence of Visual Impairment on The Quality of Life: A Survey of Patients Reporting at The Low Vision Centre of the Eastern Regional Hospital Of Ghana
Abstract
Our aim was to evaluate the influence of visual impairment on the quality of life of patients reporting at the low vision centre of the Eastern Regional Hospital in Koforidua. The World Health Organization Quality Of Life (WHOQOL-Bref) which assesses quality of life in four main domains was administered to two hundred and ninety four (294) patients who visited the low vision centre of the Eastern Regional Hospital, for various eye services. Additional information on patient demographics and their visual acuities were obtained. The mean quality of life scores were determined for the visually and non-visually impaired. 86(29.3%) of the participants were visually impaired (presenting vision worse than 6/18). A significant difference in mean age was realized between subjects who were visually impaired (53.7 ± 18.4) (mean ± SD) and subjects who were not visually impaired (34.3 ± 13.1) (p = 0.001). The visually impaired participants had a lower quality of life scores in all four domains of quality of life naming, environmental, physical, social and psychological with 7.5% unadjusted reduction in overall quality of life.
Visual impairment is associated with significant reduction in different quality of life domains for this population. Quality of life is poorer with increasing severity of visual impairment.
Article Information
- Received
- Accepted
- Published
Academic Editor: Federico Gonzalez-Fernandez1,
Checked for plagiarism: Yes
Review by: Single-blind
Academic Editor: State University of New York Buffalo,
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Angela Ofeibea Amedo, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Angela Ofeibea Amedo, Department of Optometry and Visual Science, Kwame Nkrumah University of Science and Technology, Private Mail Bag, Kumasi, Ghana —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Visual impairment refers to loss of vision due to blindness and or low vision state of a person, which cannot be corrected by conventional ophthalmic therapy such as refractive correction, use of medication or surgery and consequently affects visual capabilities 1,2. The World Health Organization expands this definition by including that, persons with visual impairment have a visual acuity of less than 6/18 up to light – perception, and may also have a visual field of less than ten degrees (10°) which they use or can potentially use for the planning and or execution of visual tasks 3. Many visually impaired persons have some form of residual (low) vision that may be sufficient for their visual needs upon receiving some form visual rehabilitation and expert clinical counseling 1.
Global estimates of visual impairment as of 2012 were 285 million (39 million blind people versus 246 people with low vision) 4. Some 80% - 90% of world’s visually impaired people live in third world countries. Reports from Sub – Saharan Africa show that, 3% of Ghana’s population is visually impaired from a number of causes 5.This underscores visual impairment as enormous public health problem, particularly in the developing world.
The causes of visual impairment are many and varied; some of them are present at birth and others acquired later in life. Congenital conditions namely, glaucoma, amblyopia, cataract, nystagmus and malformation of the visual system have been implicated in visual impairment. Some other cited causes of visual impairment include ocular injuries; age related diseases such as age related macular degeneration (ARMD), diabetic retinopathy and other forms of degenerative eye diseases 6, 7, 8, 9.
Individuals who are visually impaired experience a significant impact on their quality of life which may vary per age. The visually impaired child may suffer delayed development of gross and fine motor skills as well as perception. Certain studies mention that, the life span of a visually impaired person could be significantly affected. Apart from these, impaired vision may cause disabilities by interfering with a person’s ability to function independently – depriving them of their ability to perform everyday tasks such as traveling or navigating safely in one’s environment 10, 11, 12, 13, 14.
Other people may suffer from visual impairment – specific problems including but not limited to difficulty in recognizing faces, inability in reading standard – sized prints, challenges with driving or using other forms of vehicular transport. For some people, visual impairment may deprive of them their ability to pursue leisure. Generally, visual impairment is thought to negatively affect the mental and physical well – being of affected individuals 15, 16, 17
While clinical evaluation of visual impairment is helpful in quantifying the extent of vision loss, relating visual impairment to its impact on the quality of life (QoL) and functional ability also proves useful – in providing a complete picture of the burden of visual impairment that is beyond conventional methods of clinical evaluation 11, 18, 19, 20. Outcome of quality of life assessments can help in choosing suitable management or modifying existing management plans for people with various degrees of visual impairment; either by prescription of low vision aids or other visual rehabilitation programs.
Herein, was an attempt to evaluate the influence of visual impairment on the quality of life of patients reporting at the Low Vision Centre of the Eastern Regional Hospital in Koforidua, Ghana.
Methods
This study was a descriptive cross-sectional survey. We employed the convenience sampling technique in the selection of the participants who comprised all consenting persons aged 14 years and above reporting at the Low Vision Centre of the Eastern Regional Hospital from January 2014 to March 2014 were enlisted in the study.
Data relevant to the study were gathered using an interviewer – administered questionnaire. We adopted the WHO’s Quality of Life assessment tool and created additional sections to collect information on participants’ age, gender, occupation, cause of visual impairment and their presenting visual acuities.
We analyzed data collected using the Statistical Package for the Social Sciences (SPSS v 20.0) software (SPSS Inc., Chicago, IL, USA). Graphs were plotted using Microsoft Excel version 2010. Descriptive statistics were employed. Test of associations were performed. Differences between comparable groups were studied using Independent sam
Description of the WHO’S Quality of Life Instrument
The WHOQOL-BREF contains a total of 26 questions that provides a broad and comprehensive assessment of each individual facet relating to quality of life. One question addresses one item from each of the 24 facets of quality of life. These are grouped into four domains of quality of life which are Physical, Psychological, Social and Environmental. In addition, two items from the Overall quality of Life and General Health facet are included. Items of the questionnaire were answered in the following manner: “how satisfied,” “amount of time”, “amount of difficulty,” and “how often” they experienced certain things within the last two weeks before the day of the interview. Quality of life scores were computed on a scale of 20 and converted to a score between 0 and 100 with higher scores indicating better quality of life.
Classification of Visual Impairment
The World Health Organization’s (WHO) International Classification of Diseases definition of VI as a visual acuity less than 6/18 was used to select the participants for the study. The degree of visual impairment was classified using the WHO ICD-10 classification as presented in the table 1
Table 1. WHO’s Classification of Visual Impairment based on Severity| CATEGORY OF VI | CORRECTED VA (Better Eye) | DEGREE OF VI |
| 0 | 6/6 – 6/18 | Normal |
| 1 | less than 6/18 – 6/60 | Moderate Visual Impairment |
| 2 | less than 6/60 – 3/60 | Severe Visual Impairment |
| 3 | less than 3/60 – 1/60 | Blind |
| 4 | less than 1/60 - PLα | Blind |
| 5 | NPLβ | Blind |
Ethical Consideration
Permission was sought from the hospital administration for the survey to be carried out in the hospital. Informed consent was also sought from the patients before they were enlisted as participants of the research. All of the study protocol was thoroughly explained to participants. The study conformed to the Declaration of Helsinki.
Results
Participants’ Demographics and Distribution of Visual Characteristics
Overall, we interviewed 294 patients (males = 53.1%, females = 46.9%) visiting the said Low Vision Center for various ophthalmic services. Participants presented various degrees of visual impairment. The mean age recorded for all participants was 39.99 ± 17.26 years. We did not detect a significant difference between the mean ages of both the male and female participants t = . There was a significant difference between the mean age of the normal sighted participants (34.31 ±13.08) and that of the visually impaired participants (53.74±18.43). A significant difference in age was realized between subjects who were visually impaired and subjects who were not visually impaired t = . Some 29.3% (86 out of the total 294) were visually impaired – presenting with a visual acuity of 6/18 or worse in the better eye. Table 2 and Table 3 show the age and gender distribution of the participants and how visual acuity and the degree visual impairment distribute among them, respectively.
Visual impairment was distributed differently among the various age group of the study respondents. Table 4 provides a summary of this finding. The study participants (visually impaired and non – visually impaired) belonged to different working groups. Some of them were teachers, nurses, and physiotherapists. Students formed 25.2% of the total number of respondents and 10.90% of the total number of respondents had no form of work ( this included 30.32% of the visually impaired individuals) while the rest belonged to either of the mentioned occupations. Figure 1 shows the how the different occupations distributed among the participants.
Figure 1. istribution of working status and status of visual impairment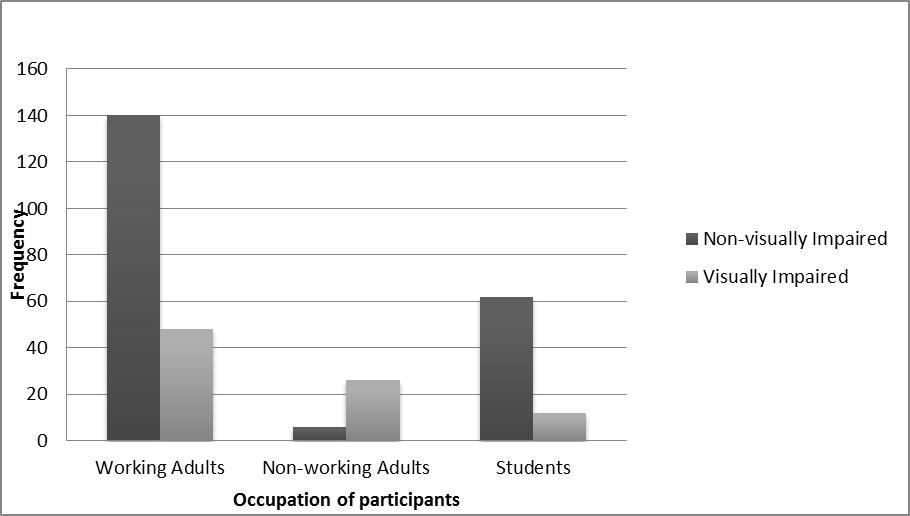
Download figure
| Age Group | Gender | TOTAL | |
| Male | Female | ||
| 11 – 20 | 20 | 16 | 36 |
| 21 – 30 | 54 | 34 | 88 |
| 31 – 40 | 20 | 30 | 50 |
| 41 – 50 | 24 | 18 | 42 |
| 51 – 60 | 18 | 20 | 38 |
| 61 – 70 | 12 | 14 | 26 |
| 71- 80 | 8 | 6 | 14 |
| TOTAL | 156 | 138 | 294 |
| c | Degree of Impairment | Frequency | Percentage |
| 6/6 – 6/18 | Normal | 208 | 70.7 |
| less than 6/18 – 6/60 | Moderate Visual Impairment | 70 | 23.8 |
| less than 6/60 – 3/60 | Severe Visual Impairment | 10 | 3.4 |
| less than 3/60 – NPL | Blind | 6 | 2 |
| TOTAL | 294 | 100 |
| Age Group | Visual Impairment Status | TOTAL | |
| Not Visually Impaired (Frequency) | Visually Impaired(Frequency) | ||
| 10 – 20 | 28 | 8 | 36 |
| 21 – 30 | 80 | 8 | 88 |
| 31 – 40 | 46 | 4 | 50 |
| 41 – 50 | 28 | 14 | 42 |
| 51 – 60 | 22 | 16 | 38 |
| 61 – 70 | 4 | 22 | 26 |
| 71 – 80 | 0 | 14 | 14 |
| TOTAL | 208 | 86 | 294 |
| Quality of Life Rating | Non-visually Impaired | Visually Impaired | TOTAL |
| Very Poor | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Poor | 0 (0.0%) | 6 (7.0%) | 6 (2.0%) |
| Neither Poor nor Good | 16 (7.7%) | 32 (37.2%) | 48 (16.3%) |
| Good | 140 (67.3%) | 46 (53.5%) | 186 (63.3%) |
| Very Good | 52 (25.0%) | 2 (2.3%) | 54 (18.4%) |
| TOTAL | 208 (100.0%) | 86 (100.0%) | 294 (100.0%) |
Figure 2. Highest level of formal education of the non-visually impaired participants
Download figure
Figure 3. Highest level of formal education of the visually impaired participants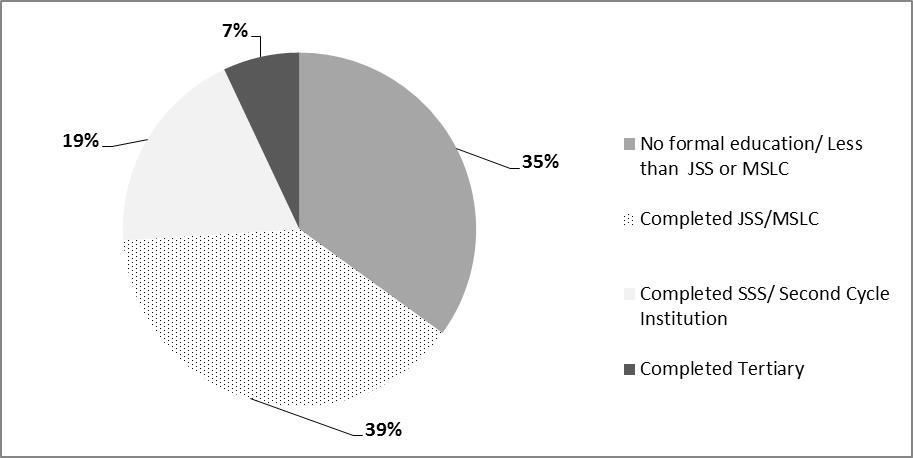
Download figure
Level of Education of Participants
The level of formal education attained, differed for each respondent sub-group (visually impaired vs. non - visually impaired); 28% of the non-visually impaired 28% had no formal education whiles 14% had completed tertiary education. For the visually impaired persons, 35% of them had no formal education (or less than the Junior Secondary School (JSS) or Middle School Leaving Certificate (MSLC). Some 7% of the visually impaired had completed Tertiary Education. Figure 2 represents the highest level of formal education of the non-visually impaired participants and figure 3represents the highest level of formal education of visually impaired participants.
Causes of Visual Impairment
The causes of visual impairment differed from respondent to respondent. The named conditions responsible for the visual impairment among the 86 visually impaired participants ranged from retinal diseases, refractive error, cataract, glaucoma and corneal diseases. Some of the visually impaired participants had no knowledge of the underlying cause of their visual impairment. Figure 4 represents the various causes of visual impairments among the study participants.
General Quality of Life of Participants
Interviewing the participants revealed a quality of life rating between “poor” to “very good”. Approximately 54% of the visually impaired rated their quality of life as “good” whiles » 17% rated their quality as “poor”. Information of participant’s quality life is represented in Table 5.
Influence of Visual Impairment on Quality of Life
Analysis of the mean scores from the WHO QoLBref administered to the participants, revealed differences in the impact of vision impairment on quality of life among the among participants. The participants without visual impairment had a mean score 81 out of the possible total score of 100 on the physical domain of quality of life. The mean score of those with visual impairment was 69%. Thus, an unadjusted decrement in quality of life of 12% was observed.
Similarly, those with no visual impairment had a mean of 75% on the psychological domain of life whiles the visually impaired had a mean of 69%. Scores on the social domain showed that persons with no impairment of vision again obtained a mean of 75% of the possible total score on while the visually impaired vision had 69% mean score on this domain – yielding an unadjusted decrement in quality of life of 6%. The Environmental domain average quality of life score of the non-visually impaired was 69% whiles that of the visually impaired persons was 63%. For all of the four domains studied, differences in QoL was significant (p - <0.001) Table 6 summarizes these findings.
We also detected that, mean QoL scores declined with the severity of visual impairment. Respondents with the defined “normal” visual acuity ( 6/6 – 6/18) scored a higher mean on the QoL assessment whereas those with < 3/60 visual acuity up to NPL and worse scored the lowest mean QoL score. Table 7 shows this observation
Figure 4. Causes of visual impairment.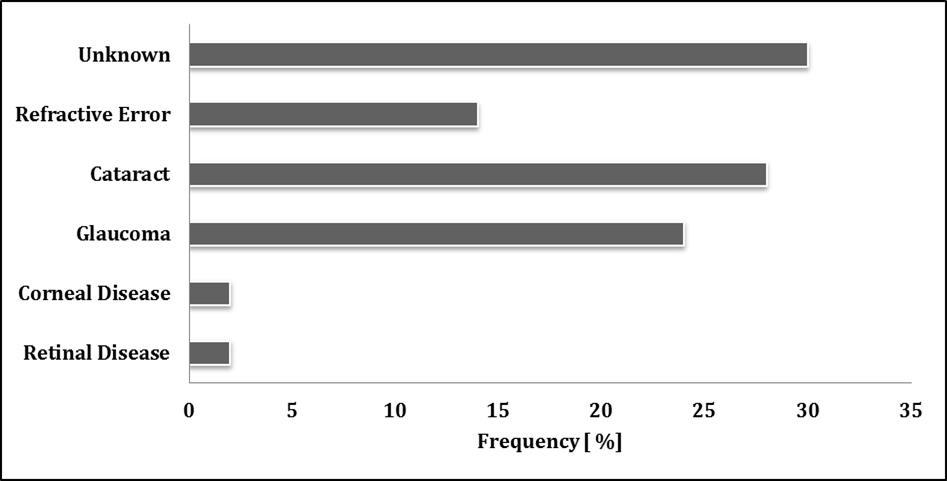
Download figure
Discussion
Results from this study indicated that more males (53.5%) were visually impaired than females. This is consistent with other findings and may have arisen due to the globally known discrepancies of gender in accessing eye care 21, 22, 23. These figures may therefore not be a true reflection of the proportion of males versus females with visual impairment in the community. It may only reflect the proportion of males and females that access eye care at this particular centre.
In many communities in Ghana, women are mostly house wives and therefore depend on the men (husbands) for support and for that matter cannot afford the cost of eye care on their own. Thus when a man and his wife both have an eye problem and he can afford the cost of treatment for only one person, it is often agreeable that the man seeks eye care since he is the one working to support the family. There was a generally higher literacy rate among males – this perhaps makes them more aware of the signs and symptoms of the various eye diseases prompting them to access eye care 24, 25
Table 6. Effect of Visual Impairment on Quality of Life (QoL) scores| WHO QOL Bref domains | Persons with Normal | Persons with Visual Impairment | Percentage reduction in QOL | |
| MEAN | MEAN | MEAN | P -Value | |
| Physical | 81 | 69 | -12 | 0.001 |
| Psychological | 75 | 69 | -6 | 0.001 |
| Social | 75 | 69 | -6 | 0.001 |
| Environmental | 69 | 63 | -6 | 0.001 |
| Overall quality of life | 75 | 67.5 | -7.5 | 0.001 |
We recorded a higher number of males (53.1%) than females. This probably translates into our finding that most of the visually impaired were males. While this was what we found, a study conducted in an Indian aged population 18 , on the impact of impaired vision and eye disease on quality of showed the contrary; 56.5% of the visually impaired in that study populations were females, with the others being males.
A significant difference in age was realized between participants who were visually impaired and participants who were not visually impaired. The mean age of “normal” sighted participants was 34.31 ± 13.08 and that of the visually impaired participants was 53.74 ±18.43.Though it may prove challenging to explain this finding, a possible inference that could be drawn to account for this observation is that most of the causes of visual impairment – glaucoma, cataract and other retinopathies are commoner among people of in the fourth to fifth decades of life and beyond 26, 27, 28. It is interesting to note that most studies on the impact of visual impairment on the quality of life reviewed were carried out in the elderly population aged 40 years and above because visual impairment is generally known or assumed to be a problem of the elderly 8, 29, 30.
Table7. Severity of Visual Impairment vs. Quality of Life (QoL) Score| Presenting VA | Degree of Impairment | Mean QOL score (20) | Mean QOL score (100) |
| 6/6 - 6/18 | Normal | 16.12 | 75 |
| <6/18 - 6/60 | Moderate Visual Impairment | 15.21 | 70 |
| <6/60 - 3/60 | Severe Visual Impairment | 14.44 | 64 |
| <3/60 - NPL | Blind | 13.45 | 59 |
However, visual impairment in childhood has far reaching implication for the affected child since the child will live with the impairment for a greater period of time. Thus and throughout life, the visual impairment will profoundly affect the influences educational, employment, personal and social prospects of the individual (child) in question. In this study, 23% of the visually impaired were younger than 40 years and therefore future research on the impact of visual impairment on quality of life must not exclude them.
Visual impairment is more prevalent in the elderly population especially after the age of 50 years. According to WHO, about 65% of all people who are visually impaired are aged 50 years and older 4. The observation that a greater percentage of 60.47% of the visually impaired were aged 50 years or greater in this study is in line with WHO reports. It was found that the proportion of the visually impaired participants increased with increasing age. Most of the visually impaired participants (25.6%) were within the age group of 61 and 70 years.
Our study showed that, relative to adult participants with no visual impairment, a greater proportion of adult participants with visual impairment were not working. Similarly, a study 31 carried out in the US to assess the impact of unilateral and bilateral visual impairment and its severity on health-related quality of life in Latinos 40 years and older revealed that a greater proportion of the visually impaired were unemployed as compared to the visually impaired. This is expected due to the visual requirements of many occupations. Every occupation requires some level of good vision in order to perform functions effectively at the work place. A high level of unemployment among the visually impaired further negatively impacts their quality of life since they do not make any income and become financially dependent on family to cater for themselves and to buy any medication and low vision aids that can help improve their quality of life. The importance of taking steps to prevent visual impairment should be a public health priority.
This study determined that, on the average, people with visual impairment were less educated than those with no visual impairment. Consistent with our study, were two different investigations 18, 31, 32 which reported that level of education was likely to be affected by visual impairment with lower number of years of formal education among the visually impaired. The exact association between level of education and visual impairment could not be revealed since we do not know the age of onset of the visual impairment and the presence of other factors like age, gender and socioeconomic status that influences level of education.
Further, our study found causes of visual impairment similar to what others haveother reported. The major causes of visual impairment were cataract (32.6%), glaucoma (27.9%) and refractive error (16.3%). A study done on cataract in Wenchi district 33 , Ghana shows that it is a leading causes of visual impairment. That study showed that cataract (62.5%) was the most common cause of blindness in individuals aged 30 years and older. Studies done in China, Indonesia and Ethiopia have also shown that cataract was the leading cause of low vision, accounting for 49.83%, 61.30% and 55.00% in China, Indonesia and Ethiopia respectively 4. According to reports from WHO, the principal causes of visual impairment globally are uncorrected refractive errors and cataracts, 43% and 33 % respectively. Other causes are glaucoma, 2%, age related macular degeneration (AMD), diabetic retinopathy, trachoma and corneal opacities, all about 1%.
We also found that as many as 37.5% and 15.4% of the participants with normal vision had refractive error and glaucoma respectively. This shows that management of the eye disease or condition can prevent visual impairment and its impact on the quality of life. It is important though that this “normal” or no visual impairment group is monitored closely, as operational definition for vision impairment encompasses people with visual acuity of 6/6 – 6/18 in the better eye. Some are close to the 6/18 end of the spectrum thus making them borderline visual impairment candidates.
Quality of life was measured by self-report; we used the generic WHOQoL-Bref rather than a vision-specific questionnaire. We chose this tool because it has particular utility in a population in which studies of quality of life have been rarely conducted and is designed for use across diverse cultures 34. By allowing assessment to be made in four life domains, the instrument provides an opportunity to examine the specific impacts of visual impairment in these areas.
As presented in the results, our study demonstrates that visual impairment is associated with a significant decrease in quality of life. The impact of visual impairment on quality of life was all encompassing, with significant reductions in the physical, psychological, social as well as environmental domains, and accounting for 7.5% unadjusted reduction in the overall quality of life of the participants in this sample. The decrement in quality of life was greatest in the environmental domain which indicates that visual impairment greatly affects our capacity for work, ability to get around and dependency on medication. A comparable study in Nigeria 32 found an association of visual impairment with reduced quality of life among the aged 65 years and older 35. They explored the impact of distance and near visual impairment on quality of life separately. Whiles the effect of distance visual impairment was limited to quality of life in the environmental domain, that of near visual impairment affected all the four domains. The reduction in quality of life scores for distant visual impairment was only remarkable in the environmental domains since affected older persons would be less able to move about and socialize.
We also detected intragroup differences in terms of how the participants rated their quality of life (Table 5). This finding should be considered in the light of the subjectivity of the individual participants in terms how they interpret and experience each of the elements in the four domains of quality of life studies. By this, it for example, proves challenging to explain why “67.3%” of the visually impaired rated quality of life as good while 25.0% rated quality of life as “very good” for them.
Moreover, this study predictably showed a distinct pattern of greater reduction in quality of life with increasing severity of visual impairment. Compared to participants with moderate visual impairment, participants with severe visual impairment had significantly lower QoL score which was lowest among the blind participants. One other study 31 found that impact of visual impairment on quality of life was profound in people with poorer vision. Similarly, it was observed in a large population-based study of Mexican Americans 36 that there were steeper decreases in scores for driving, distance vision, and mental health with worsening vision. Such findings further substantiate the view that the impact of visual impairment on quality of life is determined by the severity of the impairment 37.
Other reports 10 have ranked that vision loss is as one of the world’s major causes of loss of wellbeing. These reports have also indicated that limitations in the performance of desired tasks bring about frustrations which can consequently lead to depression. This finding further agrees with what is reported in one other similar study 38. This latter study indicated that most low vision patients worried about the effect of the visual impairment on their quality of life 38.
Additional reduction in quality of life was observed when participants indicated that they were frustrated, had less control over what they do, relied on others a lot and also needed more help from others in the performance of desired tasks. As a result of this, the visually impaired accomplished less than they desired to. This clearly points to the fact that, generally, the visually impaired is not satisfied with the heights they reach in activities they perform. Generally, for a person to accomplish something, it may be required that the individual works longer and harder than what he/she can normally do. Results show that their visual impairment affected the attainment of their desired goals. This was also realized from the findings of this study. It can thus be said that, the issue of visual impairment and its consequences cannot be relegated to the affected individuals only. If these individuals are relying on others and requiring more help from other people in their homes, work places and schools and wherever they find themselves, it then implies the active involvement of the family, friends, colleagues and schoolmates, the community and entire society. It has also been reported that there existed significant individual, public health, and community consequences of visual impairment for people caring for and assisting the visually impaired 38, 39.
Conclusion
It suffices to say that, visual impairment affects the quality of life of the participants of this study. The reduction in the quality of life in the physical, environmental, social and psychological domains of their lives was invariably significant. Quality of life was severely affected when there was remarkable vision impairment. We realized that visual impairment was a problem of both the younger and aged participants.
Recommendation
Visual impairment should be treated as an issue of major public concern. Efforts should be made to include quality of life assessment in the care protocol for the visually impaired. This will help in effective rehabilitation of the visually impaired, maximizing the residual vision and helping to enjoy life and to perform everyday tasks to the optimum. We further encourage future studies to include participants belonging to a wide age range and presenting with different causes of visual impairment. This will provide useful insight into how quality of life may be affected in visual impairment.
References
- 1.Arditi A, Rosenthal B, editors. (1998) Developing an objective definition of visual impairment. Vision'96: Proceedings of the International Low Vision Conference; .
- 3.Organization W H. (2007) . Diseases of the Eye and Adnexa International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) .
- 4. (2010) Word Health Organization. Global Data on Visual Impairment2010.Available at :http://www. who int/blindness/GLOBALDATAFINALforwebpdf.
- 6.Congdon N G, Friedman D S, Lietman T. (2003) Important causes of visual impairment in the world today. , Jama; 290(15), 2057-60.
- 7.Attebo K, Mitchell P, Smith W. (1996) Visual acuity and the causes of visual loss in Australia: the Blue Mountains Eye Study. , Ophthalmology; 103(3), 357-64.
- 8.Klaver C C, Wolfs R C, Vingerling J R, Hofman A, de Jong PT. (1998) Age-specific prevalence and causes of blindness and visual impairment in an older population: the Rotterdam Study. , Archives of Ophthalmology; 116(5), 653-8.
- 9.Resnikoff S, Pascolini D, Etya’ale D, Kocur I, Pararajasegaram R et al. (2004) Global data on visual impairment in the year 2002. Bulletin of the world health organization. 82(11), 844-51.
- 11.Chia E-M, Wang J J, Rochtchina E, Smith W, Cumming R R et al. (2004) Impact of bilateral visual impairment on health-related quality of life: the Blue Mountains Eye Study. , Investigative Ophthalmology & Visual Science; 45(1), 71-6.
- 12.Rosenblum L P. (2000) Perceptions of the impact of visual impairment on the lives of adolescents. , Journal of Visual Impairment & Blindness(JVIB);94(07)
- 13.Mason H, McCall S. (2013) Visual impairment: Access to education for children and young people: Routledge;.
- 14.Keeffe J, Lam D, Cheung A, Dinh T, McCarty C. (1998) Impact of vision impairment on functioning. Australian and New Zealand journal of ophthalmology;26(S1):S16-S8.
- 15.Evans J R, Fletcher A E, Wormald R P. (2007) Depression and anxiety in visually impaired older people. , Ophthalmology; 114(2), 283-8.
- 16.Freeman KF CR, Faye E F, Freeman P B, Goodrich G L, Stelmack J A. (2007) Optometric clinical practice guidelines: care of the patient with visual impairment (low vision rehabilitation).U.S.A.:American Optometric Association.
- 17.Kelly M. (1995) Consequences of visual impairment on leisure activities of the elderly: Elders with vision impairment need additional information and assistance to achieve adaptation in the area of vision and vision-related tasks. , Geriatric Nursing; 16(6), 273-5.
- 18.Nutheti R, Shamanna B R, Nirmalan P K, Keeffe J E, Krishnaiah S et al. (2006) Impact of impaired vision and eye disease on quality of life in Andhra Pradesh. , Investigative ophthalmology & visual science; 47(11), 4742-8.
- 19.Scott I U, Smiddy W E, Schiffman J, Feuer W J, Pappas C J. (1999) Quality of life of low-vision patients and the impact of low-vision services. , American journal of ophthalmology; 128(1), 54-62.
- 20.HJB Weih M L, Keeffe J. (2002) Assessment of the Impact of Vision Impairment. , Invest Ophthalmol Vis Sci; 43, 927-35.
- 21.Khandekar R, Mohammed A. (2009) Gender inequality in vision loss and eye diseases: evidence from the Sultanate of Oman. Indian journal of ophthalmology;. 57(6), 443.
- 22.Khandekar R, Mohammed A J, Raisi A A. (2007) Prevalence and causes of blindness & low vision; before and five years after ‘VISION 2020’initiatives in Oman: a review. Ophthalmic epidemiology;. 14(1), 9-15.
- 23.Courtright P, Lewallen S. (2007) Improving gender equity in eye care: advocating for the needs of women. , Community Eye 20(64), 68.
- 24.Ensor T, Cooper S. (2004) Overcoming barriers to health service access: influencing the demand side. Health policy and planning;. 19(2), 69-79.
- 25.Ntim-Amponsah C, Amoaku W, Ofosu-Amaah S. (2006) Alternate eye care services in a Ghanaian District. Ghana medical journal;. 39(1), 19-23.
- 26.Bressler N M. (2004) Age-related macular degeneration is the leading cause of blindness. , Jama; 291(15), 1900-1.
- 27.Evans J, Fletcher A, Wormald R. (2004) Causes of visual impairment in people aged 75 years and older in Britain: an add-on study to the MRC Trial of Assessment and Management of Older People in the Community. , British Journal of Ophthalmology; 88(3), 365-70.
- 28.S de Voogd, Ikram M K, Wolfs R C, Jansonius N M, Hofman A et al. (2005) Incidence of open-angle glaucoma in a general elderly population: the Rotterdam Study. , Ophthalmology; 112(9), 1487-93.
- 29.Tomany S C, Wang J J, R van Leeuwen, Klein R, Mitchell P et al. (2004) Risk factors for incident age-related macular degeneration: pooled findings from 3 continents. , Ophthalmology; 111(7), 1280-7.
- 30.Khurana A. (2007) Comprehensive Ophthalmology. Edition 5.New Age International Limited Publishers,New Delhi,India.
- 31.Varma R, Wu J, Chong K, Azen S P, Hays R D et al. (2006) Impact of severity and bilaterality of visual impairment on health-related quality of life. , Ophthalmology; 113(10), 1846-53.
- 32.Bekibele C O, Gureje O. (2008) Impact of self-reported visual impairment on quality of life in the Ibadan study of ageing. , British Journal of Ophthalmology; 92(5), 612-5.
- 33.Moll A, Linden A Van der, Hogeweg M, Schader W, Hermans J et al. (1994) Prevalence of blindness and low vision of people over 30 years in the Wenchi district, Ghana, in relation to eye care programmes. British journal of ophthalmology;. 78(4), 275-9.
- 34.Group W. (1995) The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. , Social Science and Medicine; 41(10), 1403-9.
- 35.Ekpenyong B, Ndukwe O. (2010) Provision of low vision service in the department of ophthalmology university of Calabar teaching hospital. , Journal of the Nigerian Optometric Association; 16(1), 34-8.
- 36.Broman A T, Munoz B, Rodriguez J, Sanchez R, Quigley H A et al. (2002) The impact of visual impairment and eye disease on vision-related quality of life in a Mexican-American population: Proyecto VER. , Investigative ophthalmology & visual science; 43(11), 3393-8.
- 37.Langelaan M, de Boer MR, van Nispen RM, Wouters B, Moll A C et al. (2007) Impact of visual impairment on quality of life: a comparison with quality of life in the general population and with other chronic conditions. Ophthalmic epidemiology;. 14(3), 119-26.
Cited by (24)
This article has been cited by 24 scholarly works according to:
Citing Articles:
European Journal of Preventive Medicine (2026) Crossref
British Journal of Visual Impairment (2026) Crossref
World Neurosurgery (2025) Crossref
Occupational Therapy In Health Care (2025) Crossref OpenAlex
Lulwah Almulhim, Talal Alshammari, Elizabeth Barstow - Occupational Therapy in Health Care (2025) Semantic Scholar
Lecture notes in electrical engineering (2025) OpenAlex
Disability & Society (2024) Crossref OpenAlex Semantic Scholar
Journal of Korean Biological Nursing Science (2024) Crossref OpenAlex Semantic Scholar
Artificial Intelligence in Medicine (2023) Crossref OpenAlex Semantic Scholar
Asian Medical Journal and Alternative Medicine (2023) Crossref
International Journal of Environmental Research and Public Health (2023) Crossref OpenAlex Semantic Scholar
Social Indicators Research (2023) Crossref OpenAlex Semantic Scholar
European Journal of Humanities and Social Sciences (2023) OpenAlex
Journal of Family Medicine & Community Health (2023) OpenAlex
Healthy Populations Journal (2023) OpenAlex
Ksenija Stanimirov, Branka Jablan, L. Mijatović, Aleksandra Grbović - Specijalna Edukacija i Rehabilitacija (2022) Semantic Scholar Crossref OpenAlex
Scientific Dental Journal (2022) Crossref OpenAlex Semantic Scholar
E. Caputo, Rafael B. Porcellis da Silva, Larissa Leal da Cunha, G. R. Krüger, F. Reichert - Journal of Visual Impairment & Blindness (2022) Semantic Scholar Crossref OpenAlex
International Ophthalmology (2022) Crossref OpenAlex Semantic Scholar
K. Omoto - Asian Journal of Human Services (2020) Semantic Scholar Crossref OpenAlex
Research Square (Research Square) (2020) OpenAlex
J. Tetteh, Gladys Fordjour, G. Ekem-Ferguson, A. O. Yawson, V. Boima et al. - BMJ Open Ophthalmology (2020) Semantic Scholar Crossref OpenAlex
Nabeela Ebrahim, F. Karim, Mvelo Gasa, Kereshni Poonvaganum, Faaizah Gangat et al. - African Vision and Eye Health (2019) Semantic Scholar Crossref OpenAlex